
Abstract
Introduction
Increased distance to care can reduce patients' access to healthcare services. For instance, patients who have to travel for care attended fewer checkups for chronic conditions 1 or fewer preoperative assessments prior to surgery. 2 Distance can also adversely affect patients' health, for example, through increased deaths from heart attacks and unintentional injuries. 3 Facilitating access to medical services via telecommunications technology is one way to reduce barriers caused by distance and time. In this study we used road travel time to examine potential access to telemedicine units in the medically underserved region of Northern Ontario, Canada.
Northern Ontario covers an area of 802,775 km2 (larger than France), with 775,000 people, which represents 88% of Ontario's landmass and 6% of the population. 4 Approximately 66% of Northern Ontario's population resides in urban centers, and the remainder is scattered across the region, including many small communities, some of which are accessible only by train, airplane, or winter (ice) road. 5 The sparse population across a large area creates travel barriers to medical services for people in Northern Ontario communities—barriers that are different from those experienced by people in the rest of Ontario or in other more developed and densely populated regions.
Although the idea of improving access to medical care seems simple, the concept of access is complex, 6,7 and medical care providers and policy makers must consider various aspects to optimize access and, ultimately, utilization. This article focuses on the geographic dimension of access as per Fortney et al. 8 and includes the location of Ontario Telemedicine Network (OTN) units (health system characteristic), road networks (the built environment within community characteristics), and population size. OTN is a not-for-profit organization funded by the Ontario Ministry of Health and Long Term Care to facilitate virtual care services throughout the province. 9 OTN is the largest telemedicine service provider in Canada 10 and one of the largest in the world. 11
An OTN unit is made up of a collection of telemedicine equipment connected to OTN's secure virtual private network communications system. OTN units are often located in healthcare centers, including hospitals, nursing stations, health/medical care clinics, public health units, and treatment centers. 12 Facilities are responsible for the purchase and maintenance of equipment. Connection to the virtual private network, which includes access to the secured network as well as videoconferencing, educational, and technical support services, 13 costs $0 CAD (Canadian dollars) for facilities funded by the Ontario Ministry of Health and Long-Term Care and up to $5,250 CAD annually for not-for-profit organizations. The telemedicine equipment, which includes videoconferencing equipment and peripheral devices, may be fixed or mobile within a given facility. For clinical visits, the patient is generally in a private room at one OTN unit accompanied on-site by a healthcare professional and connected through the virtual private network to the consulting clinician at another OTN unit. 14 Staff can book appointments through an online scheduling tool, and technical support is provided centrally. Workload varies with volume of OTN activity, and OTN coordinator tasks are typically included in the duties of existing personnel. Note that OTN uses the term site rather than unit, which is our preferred term as units can be mobile, whereas the term site implies a fixed location.
Telemedicine clinical utilization in Ontario has been reported at almost 100 visits per 10,000 people, which is the second highest in Canada. 15 Utilization is highest in mental health and addictions services, but telemedicine in Canada is also widely used for internal medicine, oncology, nephrology, and surgery. 15
Future research will explore clinical utilization in greater detail, whereas our focus in the present article is on potential access as a first step toward optimal use.
We examined road distance travel time to an OTN unit as a measure of potential access to clinical care services for Northern Ontario communities to assess whether OTN has the geographic reach to facilitate access to healthcare in this medically underserved region. Our findings may be of interest to policy- and decision-makers responsible for rural and other underserved areas throughout the world. Although OTN connects communities throughout Ontario, our focus was on Northern Ontario, which has a less-developed road system spanning a much larger and less densely populated area than Southern Ontario.
Materials and Methods
This project is part of a larger multiphase research program funded by the Ontario Ministry of Health and Long Term Care. OTN data were obtained under a data sharing agreement, and, although this research project was exempt, ethics approval for the full research program was obtained from Laurentian University's Research Ethics Board.
Geographic Analysis
We obtained a list of units from OTN in July 2014 that we matched to the community name on the Ontario Ministry of Natural Resources Settlement layer. 16 We used postal codes to link OTN units to a community when community names did not match.
We included communities located in Northern Ontario as defined by the current Northeast and Northwest Local Health Information Networks boundaries. 17 We obtained community data using the “populated places” points from the Ontario Ministry of Natural Resources Cultural Points dataset. 18 We verified and, occasionally, corrected the population group of communities with 1,000 or more people and a minimum of 400 persons/km2 using population data from Statistics Canada. 19 We used a variety of Internet sources to verify data for a random sample of 20 of the 433 communities with populations under 50 people: 17 were correctly assigned to the group; 1 community had a population of 200; 1 was in a provincial park and had campers and seasonal employees but no residents; and 1 was no longer inhabited.
Communities were categorized along a rural–urban gradient based on the Statistics Canada Statistical Area Classification system. 20 Urban areas include Census Metropolitan Areas (CMAs) (comprising Census Subdivisions [CSDs] with a population of at least 100,000) and Census Agglomerations (CAs) (CSDs with population of at least 10,000). Rural areas include all other CSDs, collectively called Metropolitan Influenced Zones (MIZs), which are further categorized based on the percentage of the labor force that commutes to a nearby CMA or CA for work.
We conducted a service area analysis using the Network Analyst extension for ArcGIS version 10.0 (Esri, Redlands, CA) and Ontario road data. 21 We created polygons representing geographies within a travel time of 30 min and 60 min from OTN units. We used travel time by private vehicle because most of these communities do not have public transportation. Travel time was calculated using posted speed limits (i.e., 40–100 km/h) and road distance:
We used 30- and 60-min drive distance polygons to create the following categories: 1. Communities within a 30-min drive from the nearest OTN unit 2. Communities more than 30 min but within a 60-min drive from the nearest OTN unit 3. Communities more than a 60-min drive from the nearest OTN unit 4. Communities with limited or no road access to an OTN unit (such as communities linked to OTN units by winter [ice] roads or railroads and fly-in communities).
We visually verified the accuracy of the data by layering the service area polygons, facilities points, and color-coded community points and manually checked the distance to nearest unit for 20 randomly selected communities.
Statistical Analysis
We used Pearson's chi-squared tests to determine if there were differences in travel time among communities' population groups or between rural or urban communities. Asymptotic methods of computing chi-squared statistics would not be robust because there were many cells with no observations. Therefore, we used Monte Carlo methods based on 100,000 randomly sampled tables to obtain an unbiased estimate of the probability of getting the observed table or more extreme table configurations. 22 If the Pearson chi-squared test statistic was significant (p ≤ 0.05), then we examined the adjusted standardized Pearson residuals to determine which cell had an observed count higher or lower than the expected count, with the expected count estimated from column and row totals. 23 We used SPSS version 20 software (IBM, Armonk, NY) for these analyses.
Results
There were 2,331 OTN units as of July 2014, of which 2,026 (86.9%) were located in Ontario. Approximately one-quarter of Ontario OTN units (552/2,026) were located in Northern Ontario. Northern Ontario contained just over half of the units categorized as rural (286/549) and over three-quarters of units in the weak or no MIZ categories (181 + 26)/(243 + 28) (Table 1). Most of the units in the upper half of Northern Ontario (above Lake Nipigon) are fly-in communities, primarily First Nations (indigenous) communities, and most of the remaining units are located along highway or railway corridors, which restricts the direction of ground travel (Fig. 1).
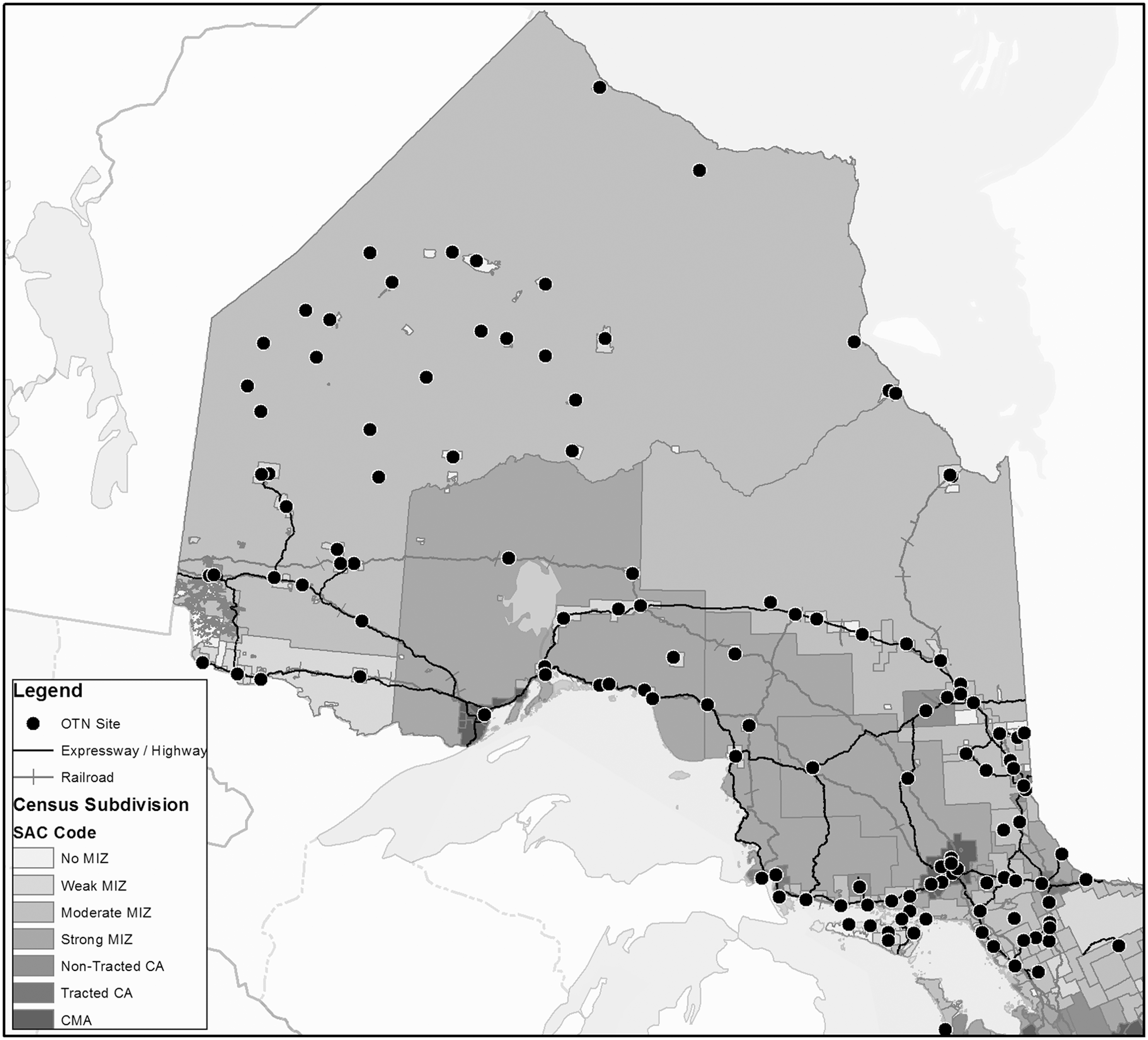
Ontario Telemedicine Network (OTN) unit locations in Northern Ontario by rural–urban continuum. Census Metropolitan Areas (CMAs) are Census Subdivisions with a population of at least 100,000, and Census Agglomerations (CAs) are Census Subdivisions with a population of at least 10,000. Rural areas include all other Census Subdivisions, collectively called Metropolitan Influenced Zones (MIZ). MIZ are further categorized based on the percentage of the labor force that commutes to a nearby CMA or CA for work: Strong MIZ has the highest percentage of commuters, and No MIZ has none. SAC, Statistical Area Classification.
Distribution of Ontario Telemedicine Network Units and Population in Ontario Along an Urban–Rural Gradient
Excludes 305 Ontario Telemedicine Network (OTN) units outside of Ontario: 192 located in other parts of Canada, 92 in the United States, 14 elsewhere, and 7 unknown/test units.
Data were obtained from Statistics Canada's Census Profile by Census Subdivision, with population data suppressed for 17 rural Northern Ontario Census Subdivisions.37
MIZ, Metropolitan Influence Zone.
There were 802 communities in the Ontario Ministry of Natural Resources cultural points dataset for Northern Ontario, of which less than 1% contained populations of 10,000 people or more (7/802) and just over half contained populations of 50 or fewer (433/802) (Table 2). Most of the larger communities have multiple OTN units (Table 1). For instance, there were 66 units in Thunder Bay and 62 in the City of Greater Sudbury—the two largest urban centers in Northern Ontario. Thirty-two Northern Ontario communities had more than one unit, and 11 northern communities had 10 or more. There was a shift based on population size from having multiple units in a community to a single unit: communities with 1,000–10,000 people averaged 3.4 units (range, 0–17), whereas communities with 50–1,000 people averaged 0.3 units (range, 0–7). Many of the smaller communities that do not contain OTN units were in close proximity to a community with one or more units.
Number of Northern Ontario Communities and Ontario Telemedicine Network Units by Population Size Group
Count of communities may differ from that based exclusively on Statistics Canada data because (1) Statistics Canada data are suppressed if population is less than 1,000 or density is less than 400 persons/m2 or (2) communities are aggregated by Statistics Canada. For example, Temiskaming Shores, which Statistics Canada considers an urban area in Northern Ontario, was disaggregated on our maps into component communities because residents are dispersed throughout many small communities in the area and typically access healthcare at one of the two larger communities (New Liskeard and Englehart).
Excludes 465 Named Places with no permanent population.
OTN, Ontario Telemedicine Network.
Of communities with larger populations, a higher percentage was close to or had an OTN unit relative to communities with fewer residents (Table 3 and Fig. 2). All seven Northern Ontario communities with a population of 10,000 or greater contained 5–66 OTN units. Approximately 97% of communities (57/59) with a population over 1,000 had OTN units or were within a 30-min drive. The percentage of communities with an OTN unit or within a 30-min driving distance decreased as community population size decreased. A higher percentage of communities with populations under 1,000 were 30–60 min or over 60 min of driving time away from an OTN unit or had no all-season road access. Approximately 91% of communities located within urban CSDs had OTN units or were within 30 min of an OTN unit compared with 87% of communities in rural CSDs (Table 3). There were significant differences among population size groups or between urban and rural communities as well as statistically significant trends across travel time groups (chi-squared tests for independence and for linear-by-linear association, p < 0.001) (Table 3).
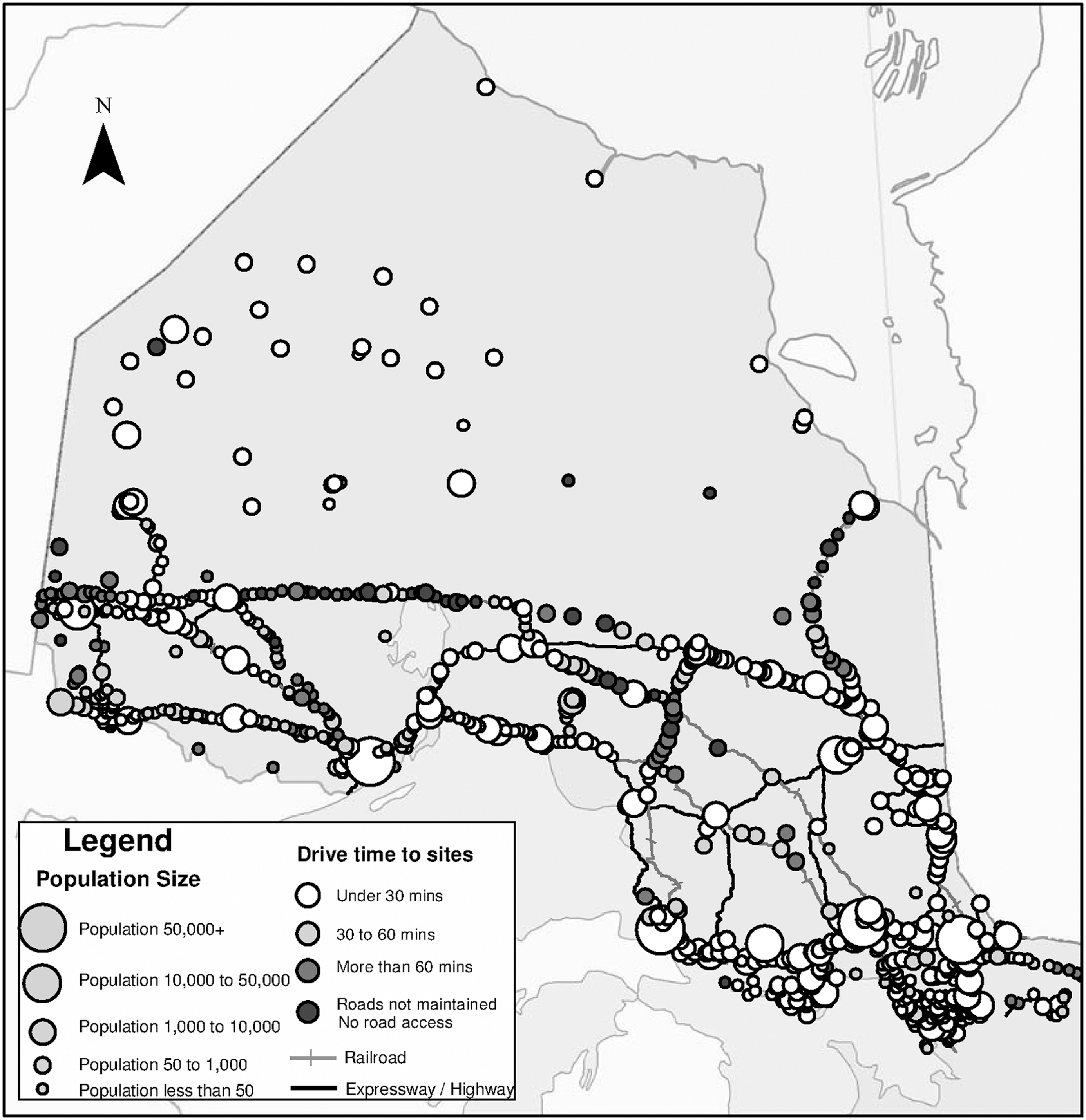
Northern Ontario communities categorized by drive time to nearest Ontario Telemedicine Network unit and population size group.
Number and Percentage by Population Size Group or Urban–Rural Group of Communities in Northern Ontario by Drive Time to Nearest Ontario Telemedicine Network Unit
An arrow indicates that the observed count was significantly higher (↑) or lower (↓) than the expected count based on column and row totals.
Pearson chi-squared tests of independence and linear-by-linear association, p < 0.001.
Discussion
The majority (86%) of Northern Ontario communities contained at least one OTN unit or were within 1 h of road travel time to the nearest unit. In a study on access to healthcare services in Ontario, Meyer 24 mapped access to conventional as well as complementary and alternative medicine by CSD, which are largely congruent with municipal boundaries, and found that access to both complementary and conventional medicine was lower in Northern Ontario CSDs than in Southern Ontario CSDs and lower in rural CSDs than in urban CSDs. We found all communities within urban CSDs were proximate to an OTN unit, whereas just over 15% of communities in rural CSDs were not.
Tepper et al. 25 found that Northern Ontario communities were at a much greater distance from care than southern communities. Residents of northern rural communities had to travel four times farther than those in southern rural communities to access tertiary care (202 km versus 45 km). Similarly, an examination of the maps on proximity to primary care and hospitals for Ontario communities by Glazier et al. 26 showed that the majority of communities with the longest travel times to health and medical care services were in Northern Ontario. Our study found a similar pattern of access to OTN units by population size group and rurality.
Access, based on proximity to an OTN unit, is modulated by the number of units within a community as well as the number of nearby communities with units. Some communities have more OTN units, whereas others have fewer than their population size might suggest. For example, consider three communities with populations of approximately 3,000–5,000 each in Northern Ontario: Community A has 14 OTN units, Community B has 4, and Community C does not have any unit. Community A is a health service and travel hub, providing services to people in remote northwestern communities, many of which are First Nations (indigenous) communities, Community B is a relatively self-contained community about 2 h from the nearest large urban center, and Community C is within an hour's drive of a large urban center and within a 15-min drive of an OTN unit. Thus the number of OTN units in a community may reflect population size of the community or regional supply and demand.
The facility in which the OTN unit is found can also influence who is able to access OTN services. For example, OTN units may be attached to a Francophone or Aboriginal health center, to a long-term care facility for older adults, or to a specific health center's clinic, such as an addiction treatment facility. Even if these centers are open to anyone, their location can influence who would know about the service and whether residents of the community think they are eligible to use the unit or whether they are comfortable accessing the OTN unit. Maximum potential access and use may be further reduced in these circumstances.
Other factors, such as hours of operation and level of support toward OTN use by healthcare providers, may reduce maximum potential access. 8 Some OTN units may be used preferentially or exclusively for educational or administrative purposes, which can further reduce access for clinical consultations. The weather can impact access, especially in Northern Ontario when snow and ice can make traveling difficult or impossible in the winter. Some residents, such as older adults and people with low income, may not own vehicles, or vehicles may be needed for work and therefore not available for medical appointments, 27 further restricting access.
Limitations
Road distance analysis uses proximity as a measure of potential access based on the existence of an OTN unit and sets the upper limit for access to and subsequent utilization of clinical services. Maximum potential access and utilization may be reduced by a variety of factors as described above. 8
We were unable to fully reconcile population size groupings with Statistics Canada Census population data for Northern Ontario communities with fewer than 1,000 people or fewer than 400 persons/km2, 19 and so we were unable to calculate OTN units per capita within the population size groupings. However, our assessment of randomly selected data points for very small communities showed good congruency with external sources, and our population size groupings for communities with 1,000 or more people are up-to-date. Also, available data did not allow for an estimate of the percentage of population by road distance to the nearest OTN unit. Although population data are available for all but a few CSDs, the large surface area of many CSDs in Northern Ontario would mean that an unknown number of smaller communities and their populations could be assigned to the wrong travel time group. In our approach, access was assessed at the community population size group, which estimated differences in access for communities dispersed within large geographical areas but did not permit estimates of access per capita.
Next Steps
Future research program will examine utilization rates for each community and assess factors that affect OTN uptake through analyses of administrative data and interviews with key stakeholders. In Fiscal Year 2012/2013, OTN served 308,000 patients, providing clinical services that were categorized into broad therapeutic areas of care as 71% mental health, 9% internal medicine, 5% oncology, and 5% surgery. 28 Subsequent research will complement the findings in this article, providing a more complete picture of who is using OTN in Northern Ontario and where the use is occurring, as well as the nature of use. Collectively, these studies may help increase the accessibility and appropriate use of OTN units throughout Northern Ontario.
Conclusions
We estimated potential access to medical care and healthcare as measured by road distance to OTN units and found that there were OTN units in many rural and remote regions of Northern Ontario. However, there was room for improvement, as 14% of communities in Northern Ontario were still more than an hour's drive from the nearest OTN unit or did not yet have road access to an OTN unit. Placing a full OTN unit in all communities may not be feasible because utilization may not warrant the investment in financial or human resources. Other solutions include improved communications infrastructure combined with use of cell phone, smartphone, or computer desktop/laptop technology. For example, although patients still go to room-based OTN units, clinical consultants' use of personal videoconferencing has steadily increased since its introduction in 2012 and in May 2014 had surpassed that of room-based units (E. Brown and R. Williams, personal communication, July 2015). Although communications infrastructure is still required, these alternatives are not as firmly tied to specific geographic locations compared with current OTN units and hence have the potential to further improve access in underserved areas or populations.
Telemedicine is one method to improve the health of people through better access to care as well as realizing monetary and environmental benefits associated with reduced patient or provider travel. 9,29 –35 OTN is the largest telemedicine network in Canada 10 and one of the largest in the world. 11 As such, our findings are of interest to policy- and decision-makers responsible for rural or underserved areas in Ontario and elsewhere in the world. Our research provides strong evidence that OTN has the geographic reach to facilitate access to medical services and has the potential to increase clinical use and to reduce medically related travel for healthcare providers and residents of Northern Ontario.
Footnotes
Acknowledgments
We would like to thank Dr. Ed Brown, Dr. Rob Williams, and other colleagues at the OTN for their advice and support of the study and for sharing data on units and locations. We thank Tomasz Mrozewski and Jill Sherman for locating map data and Wayne Warry, PhD, for his comments on an earlier draft. We thank the Ontario Ministry of Health and Long-Term Care (MOHLTC) for supporting our research through the Health System Research Fund (grant 04254SB). The views expressed in this paper are those of the authors and do not necessarily reflect the views of the OTN or the MOHLTC.
Disclosure Statement
No competing financial interests exist.