
Abstract
Introduction
The devastating complications and costs of diabetes rise exponentially as hemoglobin A1c (HbA1c) increases. 1 –3 Individuals with HbA1c >9.0%—approximately 13% of diabetes patients—are at particularly high risk for complications and costs. 4 Because improved control can reduce diabetes complications, 5 patients with persistent poorly controlled diabetes mellitus (PPDM), or maintenance of an HbA1c >9.0% for >1 year, represent a high-priority target for intervention.
Patients with PPDM often remain poorly controlled despite receiving clinic-based diabetes care with primary care providers or endocrinologists. PPDM is difficult to manage in the clinic because many factors that underlie poor control, including unreliable or unavailable blood glucose data, medication nonadherence, complex treatment regimens, and comorbid depression, 6 –8 are difficult to address with the infrequent patient–provider contact achievable in the clinic setting. 9 When clinic-based care fails to resolve PPDM, approaches are needed that can better counter factors contributing to poor control.
Telemedicine, or use of information exchanged via electronic communications for medical purposes, 10 may enhance diabetes outcomes versus clinic-based management. In studies, telemedicine approaches that address specific factors underlying poor diabetes control have proven superior to usual care. Examples of such successful telemedicine-based strategies include (1) telemonitoring to facilitate blood glucose data collection, 11 (2) self-management support to improve medication adherence, 12 (3) medication management for complex diabetes treatment regimens, 13 and (4) management for comorbid depression. 14 Given these data, a comprehensive, telemedicine-based intervention that addresses multiple factors underlying PPDM could potentially lower HbA1c levels in this high-risk, clinic-refractory group.
However, although some organizations use telemonitoring for diabetes, 15 healthcare systems have rarely integrated comprehensive telemedicine interventions into practice, even for PPDM. 16 Some of this gap stems from the fact that many studied approaches lack scalability—that is, they are not designed to broadly and effectively reach the target population. 17 In order for telemedicine to fulfill its potential as a means to reduce the burden of PPDM, interventions must be developed with a focus on scalability, such that effective implementation under real-world conditions is achievable. 18 Without such practical telemedicine options, clinicians will continue with little recourse when clinic-based diabetes care proves insufficient for PPDM.
In order to foster telemedicine-based management of clinic-refractory PPDM as a practical option within the Veterans Health Administration (VHA), the largest integrated healthcare system in the United States, 19 we developed Advanced Comprehensive Diabetes Care (ACDC). ACDC bundles telemonitoring, self-management support, medication management, and depression management—four evidence-based approaches that target factors underlying PPDM—into a comprehensive telemedicine intervention specifically designed for delivery using existing VHA clinical staffing and equipment. We constructed this approach to be (1) potent enough to reduce HbA1c levels in clinic-refractory PPDM and (2) amenable to practical delivery using existing VHA clinical resources, enhancing its potential scalability.
Materials and Methods
We conducted a pilot trial to evaluate the feasibility and effectiveness of using existing VHA clinical staffing and equipment to deliver ACDC for PPDM. We randomized 50 veterans with clinic-refractory PPDM to receive ACDC-augmented care or usual care for 6 months. This study was approved by the Durham Veterans Affairs Medical Center (VAMC) Institutional Review Board.
Study Population and Enrollment
Eligible veterans had type 2 diabetes with maintenance of HbA1c continuously >9.0% for >1 year, a minimum of two HbA1c measurements during this period, and an assigned Durham VAMC primary care provider; the presence of these three criteria indicated clinic-refractory PPDM. Given challenges initiating insulin via telephone, established insulin use was also required for inclusion. Exclusion criteria included inability to communicate by telephone (e.g., no access, hearing/speech impediment), dementia, psychosis, life-limiting illness, recent cardiovascular event or stroke, active alcohol/substance abuse, prior hypoglycemic seizure or coma, refusal to perform self-monitoring of blood glucose (SMBG), or use of continuous subcutaneous insulin infusion pumps.
A research assistant sent recruitment letters to potentially eligible veterans, followed up by telephone, conducted a baseline interview, and obtained written, informed consent. Using a computer-generated, blocked sequence, a research assistant randomized consenting veterans in an unblinded fashion. Participants in both study arms attended 3-month and 6-month outcome visits, during which they were interviewed and underwent phlebotomy for HbA1c measurement. Veterans were not compensated for study participation.
ACDC Intervention
We partnered with Durham VHA Home Telehealth (HT) program nurses to create ACDC. VHA has implemented HT programs nationwide, for which all veterans with poor diabetes control qualify. 15 Although HT nurses regularly telemonitor diabetes, they do not currently deliver comprehensive diabetes management interventions like ACDC. ACDC's delivery relies on existing VHA HT staffing and equipment; repurposing ubiquitous HT infrastructure in this manner creates the potential for scaling throughout VHA.
Veterans randomized to ACDC-augmented care were contacted by one of two study-affiliated HT nurses (A.T.M. or S.K.), who provided the standard Durham VAMC HT orientation and standard telemonitoring equipment (TELERESPONSE™ interactive voice response system; Cardiocom®, Chanhassen, MN). As would be the case in real-world practice, HT implemented the intervention; research staff managed only study-specific tasks (e.g., recruitment, randomization, outcome ascertainment). HT delivered ACDC's four components during scheduled telephone encounters every 2 weeks for 6 months and documented encounters in the VHA electronic health record (EHR).
Telemonitoring
Participants were asked to perform SMBG before meals and at bedtime and instructed to transmit these data on a daily basis using their HT-issued equipment. Per local HT policy, participants received daily automated calls to prompt data transmission; upon receiving a call, veterans reported their SMBG data using the interactive voice response system or their telephone's number keys. Failure to submit data for 3 days triggered a call from HT, followed by a letter at 5 days. At 2-week intervals, HT contacted intervention participants by telephone to review submitted SMBG data, reconcile medications, and assess diabetes medication adherence.
Self-management support
During most 2-week telephone encounters, HT delivered a diabetes self-management support module. Modules were adapted for ACDC from a prior study 20 ; the eight topics were SMBG, hypoglycemia recognition and management, diabetes medication use, diet in diabetes (two modules), self-managing insulin, exercise in diabetes, and diabetes complications. Participants were given the option to repeat a module of their choice at two encounters.
Physician-guided medication management
Following each 2-week telephone encounter, HT compiled an EHR-based report summarizing SMBG data, reconciled medications, adherence, and other relevant information. HT then forwarded this report via EHR to the study physician (M.J.C.). Medication changes were at the discretion of the study physician; insulin titration based on SMBG was the primary emphasis, with adjustment of oral antihyperglycemic agents as indicated. Recommendations were transmitted via EHR back to HT, whose nurse then relayed changes to veterans by telephone. HT documented medication changes in the EHR, alerting primary care providers to all notes. HbA1c goals were individualized as per American Diabetes Association guidelines 21 ; in order to minimize hypoglycemia, <8.0% was the typical target.
Physician-guided depression management
If veterans endorsed depressive symptoms at baseline or 3 months, HT asked the study psychiatrist (J.A.W. or J.Z.) to call and arrange an in-person evaluation within 7–14 days. Our approach emphasized pharmacotherapy proven effective in diabetes populations. 22 If participants endorsed suicidal ideation during an outcome ascertainment interview, they received emergency assessment at the Durham VAMC. In cases where a psychiatry provider was already actively managing a veteran's depression, we deferred to the existing treatment plan.
Usual Care
Participants randomized to usual care were not contacted by HT but received an educational packet and continued diabetes management with existing providers.
Study Measures
Our primary effectiveness outcome was HbA1c measured at baseline and 3 and 6 months. Secondary outcomes were diabetes self-care (Self-Care Inventory–Revised), 23 depressive symptoms (Patient Health Questionnaire-9), 24 and self-reported medication adherence (Morisky Medication Adherence Scale-4, dichotomized using a validated approach). 25,26 We also examined blood pressure (BP); participants' BP was measured three times at each outcome assessment and averaged.
We ascertained adverse events through structured self-report and EHR review. 27 Because hypoglycemia was the primary potential adverse event, we carefully analyzed the ACDC group's HT-reported SMBG data for blood glucose values <70 mg/dL and <60 mg/dL. Because usual care participants did not transmit SMBG data as part of the study, we did not analyze these data for this group.
Finally, in order to help refine ACDC and its delivery strategy, we tracked telephone encounters and nurse call times and assessed intervention acceptability at 6 months using the validated treatment acceptability and preferences (TAP) measure. 28 We also conducted semistructured interviews with intervention participants to explore perceptions about ACDC (qualitative analysis is ongoing so data are not presented).
Sample Size
Our main objective was to evaluate the feasibility of using existing VHA infrastructure to deliver ACDC; we chose our sample size of 50 veterans with this goal in mind. Because we also wished to assess ACDC's effectiveness, we performed power calculations for HbA1c based on our sample size. Assuming a standard deviation (SD) of 1.5% and a loss to follow-up of 20%, 29 we conservatively estimated that 50 participants would yield 80% power to detect a 1.4% HbA1c between-group difference (two-sided alpha = 0.05). 30
Analysis
All participants were analyzed in their assigned randomization group on an intention-to-treat basis. We examined baseline demographic/clinical data using descriptive statistics. We used linear mixed models with a constrained intercept and unstructured covariance to analyze the primary outcome and continuous secondary outcomes (diabetes self-care, depressive symptoms, BP). 31,32 We used all available data; no observations were deleted for missing follow-up. The estimation procedure used in our longitudinal analysis framework yields unbiased estimates of parameters when missing outcomes are assumed to be ignorable (i.e., related to observed covariates or response variables but not unobserved variables). 33 The primary model predictors included a common intercept, indicator variables for follow-up time, and treatment arm by follow-up time indicator interaction variables. We evaluated self-reported medication adherence as a binary outcome using a generalized estimating equation with a logit link function and an unstructured correlation structure. 34
We descriptively examined telephone encounters, nurse call times, and intervention acceptability. We descriptively characterized adverse events, including self-reported hypoglycemia and, for intervention participants, rates of hypoglycemia on HT-collected SMBG data (usual care participants did not transmit SMBG).
Results
Population Characteristics
Participants were enrolled from December 2013 to April 2014 and followed up through December 2014. The population was predominantly male and majority African American, with a mean age of 60 years and poor baseline diabetes control. Randomization groups were generally well balanced (Table 1). Observed baseline HbA1c was 10.2% in the ACDC group and 10.7% for usual care, with a linear mixed models–estimated common intercept of 10.5%. Forty-six of 50 veterans (n = 23 in each group) completed their 6-month assessment (Fig. 1).
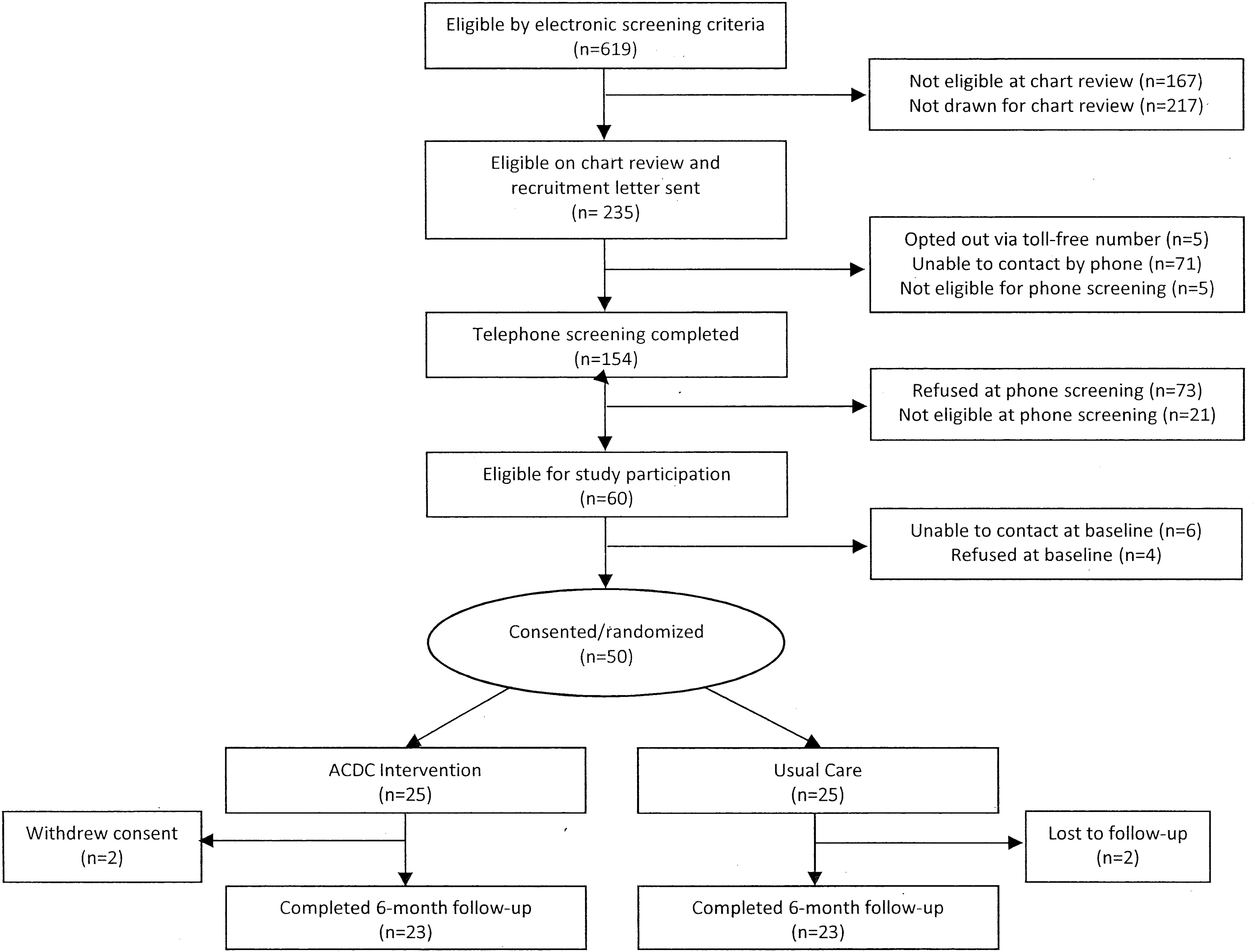
Study Consolidated Standards of Reporting Trials diagram. ACDC, Advanced Comprehensive Diabetes Care.
Study Population Baseline Data, Stratified by Intervention Arm
Unless otherwise noted, number with characteristic is given.
Inadequate income refers to patients who can pay bills only after cutting back expenditures or have difficulty paying bills despite cutting back expenditures.
Using a 4-point Likert scale, patients addressed the extent to which four statements applied to their medication-taking behavior during the past 30 days (responses ranged from “strongly agree” to “strongly disagree”); patients were classified as nonadherent if they responded “strongly agree,” “agree,” “don't know,” or “refused” for any of the four statements.
ACDC, Advanced Comprehensive Diabetes Care; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; PHQ-9, Patient Health Questionnaire-9; REALM, Rapid Estimate of Adult Literacy in Medicine; SBP, systolic blood pressure; SCI-R, Self-Care Inventory–Revised; SD, standard deviation.
Study Outcomes
At 3 months, mean HbA1c had improved by 1.3% for the ACDC group and 0.3% for usual care (estimated difference, −1.0%, 95% confidence interval [CI], −1.7 to −0.2; p = 0.012) (Table 2). A −1.0% difference was also seen at 6 months (95% CI, −2.0 to −0.0; p = 0.050). Although the intervention did not address hypertension, ACDC participants had significantly lower systolic (–7.7 mm Hg; p = 0.035) and diastolic (–5.6 mm Hg; p = 0.013) BP at 6 months versus usual care (Table 2).
Results of Longitudinal Data Models Comparing Study Outcomes in Intervention Versus Usual Care Patients
Primary analysis. Models include data from 50 patients (n = 25 in the intervention [Advanced Comprehensive Diabetes Care (ACDC)] group and n = 25 in the usual care [UC] group).
Values represent means of three measurements performed by research staff at study visit. Models include data from 49 patients (n = 25 in the intervention group and n = 24 in the UC group).
Models include data from 50 patients (n = 25 in the intervention group and n = 25 in the UC group).
CI, confidence interval; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; PHQ-9, Patient Health Questionnaire-9; SBP, systolic blood pressure; SCI-R, Self-Care Inventory–Revised; SE, standard error.
ACDC participants had significantly better diabetes self-care at 6 months than usual care (estimated difference in Self-Care Inventory–Revised = 7.0; p = 0.047), but self-reported medication adherence and depressive symptoms did not differ between groups (Table 2). It is notable that of the seven ACDC participants with depressive symptoms at study baseline, six already had VHA psychiatry care; consequently, only one veteran required expedited study psychiatrist evaluation.
The ACDC group completed an average of 8.7 (SD 4.8) of the 12 scheduled telephone encounters. Of the 23 ACDC participants with 6-month follow-up data, 16 completed six or more encounters (Fig. 1). These “engaged” veterans had a particularly strong response to ACDC, with an observed mean HbA1c improvement from 10.2% at baseline to 8.3% at 6 months (Table 3). The remaining seven intervention participants completed three or fewer telephone encounters and had an observed mean HbA1c of 10.8% at 6 months, versus 10.3% at baseline (Table 3).
Change in Observed Hemoglobin A1c During the Study Period for Engaged (Six or More Study Encounters) Versus Nonengaged Intervention Patients (Three or Fewer Study Encounters)
HbA1c, hemoglobin A1c; SD, standard deviation.
Nurses spent approximately 30 min conducting each intervention telephone call. Although not formally tracked for the purposes of this pilot, estimated study physician time was <5 min per intervention encounter. Based on the four TAP measure components, participants found ACDC acceptable (Table 4). In particular, participants felt that ACDC was an effective way to address their diabetes and expressed willingness to continue applying the skills they had learned.
Treatment Acceptability and Preferences Measure for Intervention Patients
Using a 5-point Likert scale, patients addressed the extent to which four statements described their perceptions of the ACDC intervention; responses ranged from 0 (“not at all”) to 4 (“very much”).
One patient responded “don't know” to all items, and an additional patient responded “don't know” to Item 2.
ACDC, Advanced Comprehensive Diabetes Care; SD, standard deviation; TAP, Treatment Acceptability and Preferences.
Adverse Events
Adverse events were uncommon and similar between groups. No participants reported hypoglycemia requiring assistance. Among the 20 ACDC participants transmitting SMBG data during the study, hypoglycemia was most common during the period after enrollment but prior to the first intervention telephone encounter. Hypoglycemia was rare thereafter, with participants reporting a median of zero SMBG values <70 mg/dL (interquartile range, 0–4) and zero <60 mg/dL (interquartile range, 0–1). Three veterans had more than five blood glucose values <70 mg/dL after intervention initiation, and only one had more than five such values <60 mg/dL; this veteran was identified as having HbA1c–blood glucose discordance, and his hypoglycemia resolved by study end.
Discussion
In order to reduce the burden of PPDM, there is a need for comprehensive telemedicine interventions that can be practically and effectively implemented in real-world settings. This pilot study demonstrated that existing VHA clinical staff can deliver comprehensive telemedicine-based care for PPDM using standard VHA equipment. ACDC appeared to reduce HbA1c versus usual care among veterans whose diabetes had remained persistently poorly controlled despite clinic-based care. Given ACDC's potential for scalability and effectiveness, this approach may be a vital step toward reducing complications and costs in the clinic-refractory PPDM population, where such improvements are critically needed.
Implications of Findings
We designed ACDC to be effective for PPDM by combining four evidence-based strategies that target factors known to underlie poor diabetes control. We found that ACDC improved HbA1c by 1.0%; if sustained, this change could reduce microvascular complications by 37%, myocardial infarction by 14%, and diabetes-related death by 21% for participants. 1 It is interesting that HbA1c improved by 1.0% after 3 months but then appeared to plateau from 3 to 6 months. Although this may seem to suggest that ACDC had less impact after 3 months, we found that engaged participants (six or more encounters) did continue to improve between 3 and 6 months. Overall, participants with high intervention engagement responded especially well to ACDC, with observed HbA1c improving by 1.9%.
By contrast, veterans with lower engagement (three or fewer encounters) fared less well. Because factors that underlie PPDM, such as competing demands from employment and suboptimal self-management, 7 may likewise affect general participation with medical care, we anticipated challenges engaging participants. Our Consolidated Standards of Reporting Trials diagram (Fig. 1) indicated that 73 of 154 patients (47%) approached for telephone screening declined participation. This number may have been lower had we compensated participants and may decrease when ACDC is presented as clinical care rather than research. It is encouraging that, once enrolled, most intervention participants successfully engaged ACDC, found the intervention acceptable based on the TAP measure, and exhibited clinical improvement.
ACDC is an intensive approach, and refinement for further study and eventual practical use will be crucial. As part of our ongoing qualitative work, we will explore if and how each intervention component benefitted participants. Enhanced medication management was likely important for many veterans, and their improvements in diabetes self-care suggest that self-management support was likewise helpful. By contrast, ACDC did not impact depression, which may relate to high baseline utilization of psychiatry services within VHA. Our depression component thus requires re-evaluation. As we continue to refine ACDC, we will incorporate a maintenance strategy to help patients retain improvements in glycemic control.
Although ACDC did not directly address hypertension, BP improved in the intervention group relative to usual care. Our future work will further explore this finding.
Findings in the Context of Current Literature
This work is innovative in two ways. First, we focused exclusively on veterans with clinic-refractory PPDM. Because complications and costs rise as HbA1c increases, 1 –3 patients with PPDM contribute disproportionately to the nationwide diabetes burden, 35 and so are a priority target for intervention. Even in this refractory population, ACDC had an estimated effect of 1.0%, exceeding that of many published telemedicine interventions for diabetes. 11 –13 ACDC's apparent potency may relate to its bundling of multiple evidence-based approaches. Furthermore, our cohort's markedly elevated baseline HbA1c provided ample opportunity for improvement as compared with better-controlled populations.
Second, in order to foster comprehensive telemedicine-based management as a real-world option for PPDM, we explicitly designed ACDC for practical delivery using existing clinical VHA staffing and equipment. ACDC repurposes telemedicine infrastructure that is ubiquitous at VHA centers nationwide, which gives this approach unique potential scalability. By leveraging VHA's investment in telemedicine infrastructure, ACDC has a natural avenue for dissemination throughout VHA and therefore substantial promise to widely impact PPDM. Our ongoing work will hone ACDC for broader study and clinical use.
Care delivery technology evolves continually, and for some patients intervention delivery using Web or smartphone platforms may be preferable to telephone. However, the potential advantages of leading-edge technology must be weighed against the potential for implementation. Given current VHA infrastructure, telephone-based care strikes a reasonable balance among effectiveness, reach, and potential scalability. As VHA increasingly implements alternatives to telephone-based care delivery, ACDC will evolve accordingly.
Limitations
Along with limitations discussed above, this was a single-center pilot study focusing on a small, primarily male, veteran population with insulin-requiring type 2 diabetes. Our findings should be interpreted accordingly. We used two HT nurses and a single physician for intervention implementation, all of whom were part of the study team; future work will test ACDC at different sites with local intervention teams to assure generalizability. Because ACDC is designed for implementation using VHA-specific infrastructure, our findings do not immediately translate to other settings.
This study was not specifically designed to examine effectiveness; although our results suggest that ACDC may be effective, future work is needed to confirm these findings. A formal cost-effectiveness assessment will also be needed to inform wider implementation.
Conclusions
We have demonstrated that existing VHA clinical staffing can deliver comprehensive, telemedicine-based care for PPDM using standard VHA equipment. ACDC's practicality and effectiveness may position it to meaningfully reduce the burden of diabetes within VHA, the largest integrated healthcare system in the United States. Extending our evaluation of the ACDC approach beyond VHA is critical. Given recent increases in reimbursement for chronic disease management, 36 the time is right to promote broad scaling of practical telemedicine-based disease management approaches for PPDM and other chronic illnesses that do not respond to clinic-based care.
Footnotes
Acknowledgments
We gratefully acknowledge contributions made by Stephanie Macy, research assistant at the Durham VAMC Center for Health Services Research in Primary Care. ACDC was supported by grant RRP 12-458 from the Veterans Affairs Diabetes QUERI. M.J.C. is supported by Career Development Award 13-261 from the Veterans Affairs Health Services Research and Development. H.B.B. is supported by Research Career Scientist award RCS 08-027 from the Veterans Affairs Health Service Research and Development.
Disclosure Statement
No competing financial interests exist.