
Abstract
Introduction
Older adults frequently use urgent and emergency medical care services. 1,2 The demand for acute illness care is expected to continue to increase as the population of older adults expands and stresses the U.S. healthcare system. 3 –6 Older adults with functional limitations, including those residing in nursing homes and senior living communities (SLCs), including both independent and assisted living residences, often have difficulty accessing acute illness care and present to the emergency department (ED) for care that could have been rendered in an ambulatory setting. 7 Although the ED offers the advantage of 24/7 access, care of older adults in EDs has been associated with increased cost, as well as risks of adverse events, such as falls and delirium.
Telemedicine has been proposed as a model to expand access to acute illness care and reduce the need for ED-based care. 8 –12 In pediatrics, telemedicine has been demonstrated to decrease ED use among children in childcare and schools. 13,14 Telemedicine has also been associated with a reduction in acute hospitalizations by residents of nursing homes, but only in those nursing homes that were more engaged in telemedicine. More engaged nursing homes realized an 11.3% reduction in hospitalization rates with telemedicine, compared with a 5.2% reduction in less engaged homes. 15 Our group has shown that access to high-intensity telemedicine in SLCs decreased the rate of ED use by 18%, but the effect of the level of SLC engagement with high-intensity telemedicine programs on ED use has not been specifically investigated. 16
Carman et al. 17 have defined engagement as “patients, families, their representatives, and health professionals working in active partnership at various levels across the health care system.” We follow this approach, measuring the degree to which SLC residents, families, and facility staff work with health professionals to provide acute illness care through telemedicine. Improving our understanding of SLC engagement may be critically important to designing, implementing, and sustaining cost-effective telemedicine programs. This may be particularly relevant for SLCs, compared with other settings, where wide variation in facility features and services exist. 18 –20 This study evaluated the relationship between level of SLC engagement with a high-intensity telemedicine program, represented by the rate of telemedicine use, and change in the rate of ED use among residents. Additionally, we evaluated which characteristics were associated with highly engaged facilities.
Materials and Methods
We present a secondary analysis of data from a broader study examining the effectiveness of a high-intensity telemedicine model (technician-assisted, with diagnostic capability similar to an office visit, using numerous peripheral devices for data capture). This model was provided for acute illness care for older adults residing in SLCs (Health-E-Access). Full details of program operations (the intervention) have been published previously. 9,16 In this analysis we compared ED use among subjects at three levels of intervention: (1) those with the opportunity to use high-intensity telemedicine for acute illness care at more engaged units (units in which residents used the telemedicine service more frequently), (2) those with the opportunity to use high-intensity telemedicine for acute illness care at less engaged units (units in which residents used the telemedicine service less frequently), and (3) control subjects who lived at facilities without access to telemedicine services. The University of Rochester Research Subjects Review Board approved this study.
The Intervention
Subjects were enrolled from a geriatrics practice that cares for residents of SLCs. Over the course of the study, the practice provided in-person primary care services at 26 SLC (assisted or independent) units operated by 22 SLC facilities. The practice has a separate administrative office staffed by nurses and advanced practice providers to handle administrative and clinical issues. This office or an on-call physician receives and manages all acute illness concerns.
Before starting this study, seven of these SLC facilities representing nine SLC units were invited to participate in the telemedicine intervention. These facilities were chosen carefully to ensure variation in site characteristics (e.g., size, resources, and resident demographics) within both the intervention and control groups, as well as similar resident characteristics between the two groups. One site that initially agreed to participate subsequently declined and was excluded from analyses, leaving eight units in the intervention (telemedicine) group.
Individuals were eligible to enter the intervention group as long as their primary care physician was a member of the geriatrics practice and they lived in an intervention unit. The control group included all practice patients at control units. Patients at intervention units who did not consent to the intervention were excluded from these analyses. We began following subjects on May 1, 2010, collecting data at each intervention site prior to program implementation. We introduced the program sequentially at the units to allow us to devote resources to program initiation one site at a time. The first and last units to participate initiated the program in December 2010 and August 2011, respectively. Individual subjects continued in the study until they left the geriatrics practice or died, or until the study ended (November 30, 2013).
Intervention subjects had the option to use Health-e-Access, the older adult high-intensity telemedicine program, when they had acute illness needs. 16 We defined this as “high-intensity” because it was technician-facilitated and it provided images, video, clinical auscultation, and electrocardiogram information from the patient to the provider in real time. Information collected with these tools could also be stored and forwarded for later review.
When an intervention subject or caregiver contacted staff of the geriatrics practice about an acute illness, the responsible clinic provider had the option to manage the concerns through traditional means or through telemedicine. When telemedicine was used, a telemedicine assistant went to the subject's SLC residence and gathered illness history and specific clinical data based on established protocols. The telemedicine assistant then uploaded information to the electronic medical record. Based on this information, a provider rendered a clinical assessment and plan.
Data and Analyses
To characterize the SLC facilities, we performed two different surveys. First, leaders at all of the SLC facilities covered by the geriatrics practice were asked to complete a survey describing the organizational features, location, staffing. and services available at each of their program units. They were also asked to describe the model and philosophy of care provided in their program by distributing a total of 100 points between a medical model of care and a social model of care (i.e., what percentage of the SLC model of care was medical versus social). Then, at the end of the study period, all staff members at the telemedicine intervention units were asked to complete the modified for Assisted Living version of the Nursing Home Survey of Patient Safety Culture describing their workplace. 21 Depending on the site and the level of services provided, staff members included clinical and nonclinical individuals. Descriptive statistics were generated from these surveys, both overall and by level of intervention (more engagement, less engagement, and control).
We used person-month as the unit of analysis, defined as the observation of a single subject during a given 28-day period. From the electronic telemedicine medical records, we generated descriptive statistics on the frequency and type of telemedicine visits in each SLC. Telemedicine utilization rates in intervention SLC units (telemedicine visits per 100 person-months) were used to categorize SLC units as having more engagement or less engagement in the telemedicine intervention. After each telemedicine visit, we surveyed the individual at the geriatrics practice who initiated the telemedicine visit to determine who participated in the decision to use telemedicine. We abstracted the geriatrics practice's medical records to obtain patient-level clinical information and obtained billing data from the geriatrics practice and the hospitals where patients received care. We compared the demographic characteristics of the subjects across levels of intervention.
Combining the billing data and medical records, we determined the rates of ED use, overall and by disposition, across the levels of intervention. In addition to the facility surveys, we collected data and considered as potential confounders those variables that predict ED use and are associated with intervention status. We included six patient-level characteristics in analysis: age, independent versus assisted living setting, gender, race, advance directives, and Charlson score. 22 We also included two facility-level characteristics: profit status and specialization in dual-diagnosis (medical and psychiatric) patients. Person-months with missing data for potential covariates were excluded from the multivariable analyses.
All analyses were performed using SAS version 9.3 software (SAS Institute Inc., Cary, NC). Because each subject contributed multiple person-months, our analysis accounted for the clustered data structure within subjects. Generalized estimating equations were used to estimate the effect of telemedicine on rates of ED use by fitting marginal Poisson models. Sandwich estimators were calculated to provide robust estimation of standard errors. Intervention level (more engagement versus less engagement versus control) was treated as a three-level categorical variable. Intervention level, time from study enrollment (months), and the interaction of the two were included in the model as independent variables. The interaction assessed whether rates of ED use changed differently with respect to time among subjects in the more engaged SLCs, subjects in the less engaged SLCs, and control subjects. Stratified analyses were also performed to evaluate the effect of time on ED utilizations at each intervention level. For ease of interpretation, estimated monthly rate ratios and 95% confidence intervals (CIs) were further converted to reflect annual use. Each person-year included 13 person-months of 28 days in duration.
Results
SLC organization leaders completed surveys on the features and services available at a total of 22 independent or assisted living residence units, including all 8 intervention units and 14 control units. Three control units, housing 22 subjects through the study period, did not provide any information of the features or services of their communities and were therefore excluded from analysis. The 22 units providing information housed a total of 1,219 subjects during the study period (479 intervention subjects and 740 control subjects).
Based on review of telemedicine utilization rates by intervention SLCs, we categorized four SLC units as more engaged in telemedicine (five or more telemedicine visits per 100 person-months), and we categorized four units as having less engagement in telemedicine (fewer than five telemedicine visits per 100 person-months). Figure 1 demonstrates the rates of telemedicine utilization. The 14 control units had no telemedicine use.
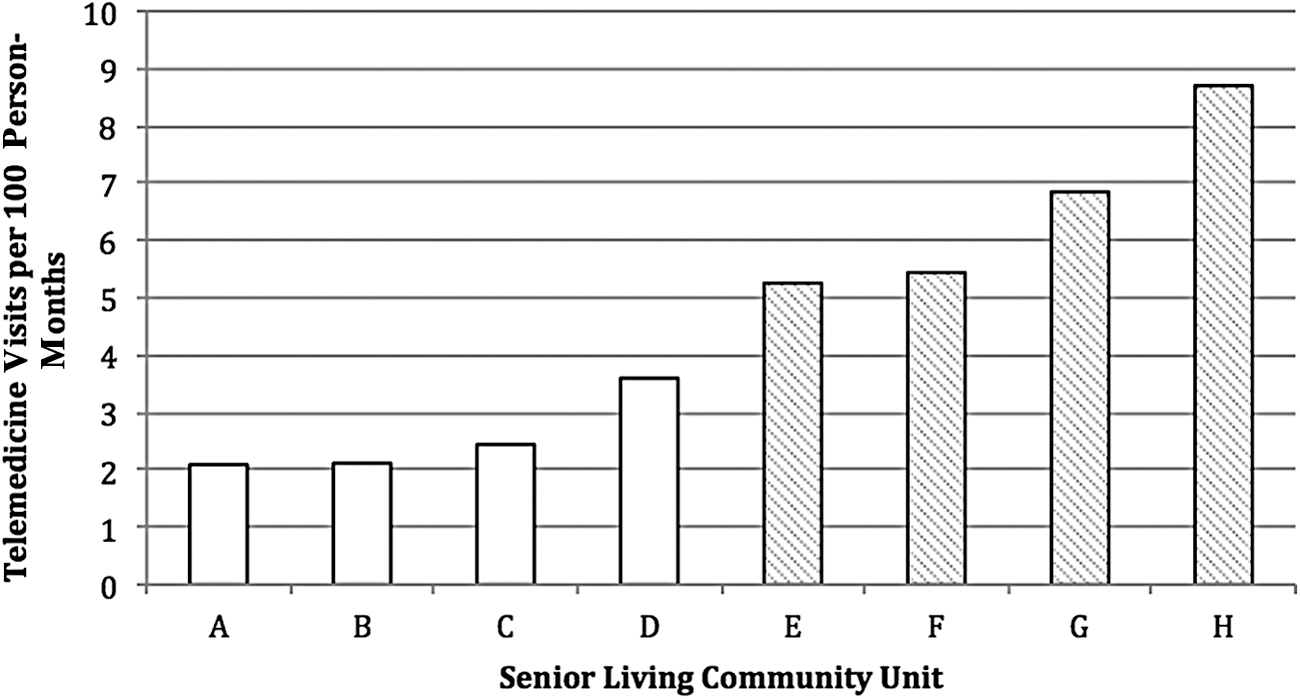
Engagement in telemedicine by senior living community unit. Units with more engagement (shaded bars) had more than five telemedicine visits per 100 person-months; open bars indicate less engaged units.
Overall, the demographic characteristics of the subjects residing in the more engaged, less engaged, and control facilities had slight differences (Table 1). Notably, subjects residing in more engaged SLC units were older, and a higher proportion was female. They were more likely to have a Medicare Advantage program as their primary insurance. There was no significant difference in the Charlson score or activities of daily living of subjects residing in more and less engaged units, although there was a statistically significant variation in dementia (p = 0.007), with fewer residents having that diagnosis at more engaged units.
Demographics of Subjects by Level of Engagement of Senior Living Community Unit in the Telemedicine Intervention
Data are number (%) except as indicated.
Median (25th, 75th percentile).
ADL, activities of daily living; DNI, do not intubate; DNR, do not resuscitate.
Characteristics of the SLC units are shown in Table 2. The more engaged SLC units reported that there was at least one registered nurse on duty for a median of 2.5 8-h shifts per week (out of 21 possible shifts) (interquartile range [IQR], 0–6) and at least one licensed nurse on duty for 3.5 shifts per week (IQR, 0–14). In contrast, less engaged SLCs in the telemedicine program reported no registered nurse staffing but did report that at least one licensed practical nurse was available for a median of 10.5 shifts (IQR, 0–21) per week in their facility. The more engaged units self-identified their focus as providing a social model of care. Of the 100 points that could be distributed between the social model and medical model of care, more engaged units attributed a median of 100 points (IQR, 80–100; n = 4) to the social model. In comparison, less engaged and control units attributed fewer points with a median of 85 points (IQR, 70–100; n = 2) and 50 points (IQR, 30–60; n = 13) attributed to the social model, respectively. The care focus (social versus medical) did not correlate with the type of care (assisted versus independent) or level of registered nursing. Staff at intervention units completed a total of 48 surveys on their safety culture. At more engaged units, 26 staff members responded with a median overall score of 76.3 (IQR, 55.3–86.8). At less engaged units, 22 staff members responded with a median culture score of 72.4 (IQR, 60.5–89.5).
Characteristics of Senior Living Community Units by Level of Engagement in Telemedicine
Data are number (%) unless indicated otherwise.
Median (interquartile range).
n = 20 (more engaged, n = 4; less engaged, n = 3; control, n = 13).
n = 17 (more engaged, n = 4, less engaged, n = 3; control, n = 10).
n = 17 (more engaged, n = 3, less engaged, n = 3).
ED, emergency department; LPN, licensed practical nurse; RN, registered nurse.
During the study period, 503 telemedicine visits were completed, with 362 (72.0%) occurring in more engaged SLCs and 141 (28.0%) in less engaged SLCs, respectively. At the more engaged SLC units, patients participated in the decision to use telemedicine for 45.8% of visits, whereas patients participated in this decision in only 8.9% of visits at less engaged units.
Table 3 demonstrates our primary outcome: healthcare utilization of subjects by level of engagement of their SLC site. Of note is that generalized estimating equations models that did not adjust for covariates showed that subjects residing in SLC units that were more engaged in telemedicine had significantly lower rates of ED use compared with control units (rate ratio [RR] = 0.76; 95% CI, 0.63–0.91; p = 0.003). Subjects at less engaged SLC units also had lower rates of ED use compared with those at control units, but the difference was not significantly different (p > 0.05).
Healthcare Utilization per Patient-Month by Level of Engagement of Senior Living Community Site in Telemedicine, Unadjusted
More engaged telemedicine intervention units were defined as those having a telemedicine visit rate of more than five visits per 100 patient-months.
Ci, confidence interval; ED, emergency department; PCP, primary care provider.
The relationship between level of engagement and ED use was sustained after adjusting for potential confounders (Table 4). The interaction effect between engagement and time was statistically significant between more engagement and control groups. Subjects residing in SLC units with more engagement in the telemedicine intervention had a significantly greater decrease of ED visits over time than subjects at control units, with an annualized decrease in ED visits of 28% compared with no significant change in ED use among subjects in control units (p = 0.036 for group × time interaction). No significant interaction effect was found for less engaged SLC units.
Annualized Rate of Change in Healthcare Utilization by Level of Facility Engagement
Estimations were based on generalized estimating equations to account for the clustering data structure. Adjusting was done for subject age, race, gender, Charlson score, residence type, care status, facility profit status (not-for-profit/for profit), and specialization in dual diagnosis (medical and psychiatric) patients.
More engaged telemedicine engagement facilities had a telemedicine visit rate of more than five visits per 100 patient-months.
Significant interaction effects with time were found between more engagement and no intervention.
ED, emergency department.
Discussion
This study demonstrates that subjects residing in more engaged SLC units experienced greater decrease in ED use from participation in Health-e-Access compared with subjects who reside in less engaged SLCs. Furthermore, the study identifies factors associated with SLC engagement. Engagement and associated factors may be critical to the success of the telemedicine model of care in SLCs in decreasing ED use and costs for patients, payers, and provider organizations.
Our finding that participants living in more engaged units benefitted more from telemedicine is not surprising. This finding is important, however, in highlighting the need to address the issue of engagement thoughtfully and thoroughly in order to achieve the potential of this innovation. The importance of engagement has never been addressed for telemedicine in the SLC setting, and the magnitude of the response has not been quantified previously. Grabowski and O'Malley 15 found decreased healthcare use among nursing home residents using telemedicine for acute illness care but no difference in the less engaged facilities.
We found that the more engaged SLC units included both independent and assisted levels of residence; thus the type of SLC likely did not predict the difference in engagement. There were some important facility characteristics that differed between engagement levels, however. The more engaged SLC units had a greater registered nurse presence, whereas the less engaged facilities were often staffed with licensed practical nurses. Even though the SLC registered nurses did not actively participate in the telemedicine visits, it is possible that the presence of registered nurses on site promoted initiation of telemedicine visits. Registered nurses may have contributed to initiation through their knowledge base, assessment skills, or interactions with residents.
Residents at the more engaged units appeared to be more involved in their own care than residents at less engaged units. This is supported by our finding that 45.8% of residents were involved in requesting the telemedicine visit in more engaged facilities, compared with 8.9% in less engaged facilities. Residents who had very high satisfaction levels with telemedicine may have advocated for telemedicine care instead of ED care for acute illnesses. 23 We also found that more engaged SLCs described their program as using a social model of care with minimal medical model presence. It is unclear why a social model may lead to increased telemedicine use. Further research is needed to understand this association.
Currently, there is no financial incentive for an SLC to become more engaged in telemedicine to reduce ED visits. SLC units do not receive payments from Medicare and infrequently receive Medicaid reimbursements. However, the residents of SLCs use EDs at high rates, and the health systems or insurance companies to which they belong may have financial incentives to reduce avoidable healthcare expenditures. Thus, these facilities, as well as any providers, payers, and financially at-risk organizations, such as accountable care organizations, should consider partnering with SLCs to promote their engagement in telemedicine, thereby decreasing rates of ED use. When health organizations consider which SLCs may make successful partners, they may wish to consider the factors that we found to be associated with more engagement.
Limitations
This work describes the impact of a high-intensity telemedicine through a single geriatric practice in a midsize metropolitan area. The findings may not be directly generalizable to other practices and communities. For this study, SLC facilities provided information about many features of their residential units. This self-report may be susceptible to inaccuracy. It also remains possible that other yet unmeasured facility site features, such as staff turnover rate, may also mitigate engagement in telemedicine.
Conclusions
Individuals residing in more engaged SLC units experienced a greater decrease in ED use compared with subjects who residing in less engaged SLCs or those without access to high-intensity telemedicine for acute illnesses. We identified potential factors associated with more engaged SLCs, but further research is needed to understand resident and staff engagement and how to increase it.
Footnotes
Acknowledgments
This project was supported by grant number R01HS018047 from the Agency for Healthcare Research and Quality.
Disclosure Statement
M.N.S. was a consultant to Fortress Investment Group and one of their companies, Lifeline2Care, which was, but no longer is, developing a senior living community telemedicine model. N.W. and K.M.M. were eligible to receive royalties while this research was active from Trifecta Technologies, which develops and maintains the software used in the study. They were no longer eligible to receive royalties as of December 31, 2013. S.M.G., E.B.W., H.W., K.N., D.N., and A.D. declare no competing financial interests exist.