
Abstract
Introduction
Fever is a common reason why about 10.5–25% of pediatric patients visit emergency departments (EDs). 1 Although a viral infection is the most common cause of fever, severe bacterial infection can also cause fever, and it should not be overlooked. 2 In the past, pathogens such as Haemophilus influenzae or Streptococcus pneumoniae mainly caused severe bacterial infection in pediatric patients. 2 However, as vaccinations for these pathogens are now available, the main cause of severe bacterial infection in pediatric patients for fever without the other symptoms has been urinary tract infection (UTI), which in turn causes fever in 4–6% of pediatric patients. 2
UTI could be diagnosed by a urine culture, a urine reagent strip, or both. 2 –4 A urine culture is regarded as the gold standard for diagnosis of UTI, but it takes at least 24 h to deliver the results. 4 For a urine reagent strip test, it cannot confirm whether UTI exists, but in an ED setting, it can be used to quickly rule out or rule in UTI in a patient in the ED also presenting urinary symptoms such as increased urinary frequency, dysuria (painful urination), or fever with flank pain. 2 –4
The urine reagent strip test, as an indirect measure of UTI, detects presence of leukocyte esterase (LE) for pyuria (a measure of granulocytic white blood cells or pus) and nitrite (NIT) (bacterial conversion of endogenous nitrates to nitrites) as indicators of bacteriuria. 5 It has been reported that high sensitivity and specificity for diagnosis of UTI were exhibited when either LE or NIT is positive: sensitivity was 93% (range, 90–100%), and specificity was 72% (range, 58–91%). 4 As such, urinalysis for LE and NIT is reported as a considerably reliable test that can predict the result of a urine culture, which in turn enables presumptive therapies for the patients. 4 Moreover, this test is cost-effective compared with other diagnostic modalities. 6
Analysis of a urine reagent strip is performed by a photometric analyzer in the department of laboratory medicine. However, if there is a sizable delay in the transfer process of urine samples from the ED to the department of laboratory medicine, the urinalysis results can be impacted. 1 According to clinical practical guidelines for UTI in pediatric patients from the American Academy of Pediatrics, it is recommended that urine sample before analysis should be kept at room temperature within 1 h and less than 4 h under refrigeration to ensure the sensitivity and specificity of the analyzed results and to reduce the risk of conversion of urine samples. 4 However, visual interpretation of a urine reagent strip by a researcher in the ED does not require much time, and a point-of-care test for LE and NIT could reduce the risk of conversion of urine samples. A color change test could be devised for this detection, as in a urine reagent strip, but it could lead to an ambiguous and inconsistent reading and a low sensitivity. 7 In addition, an experienced researcher would be required to perform the readings.
Alternatively, a smartphone could be used to read a urine reagent strip for consistent measures. 8 Many researchers have already used a smartphone camera for colorimetric diagnostics, 8 –14 particularly for the urine test. 8 –12 For example, Lee et al. 9 suggested a portable colorimetric reader of the urine dipstick, and Coskun et al. 10 reported a personalized digital albumin sensing platform. A recent study has introduced a smartphone application that is capable of performing the urine reagent strip test regardless of light conditions. 11 As these studies provide the possibility of more accurate and faster urine tests using a smartphone, the researchers evaluated their devices with artificial urine samples in the laboratory level. 8 –12 Accordingly, there is still an uncertainty about the reliability of such urine reagent strip tests in the clinical setting.
The present study was designed to assess a smartphone-based urine reagent strip test for detection of LE and NIT in urine. For this, a smartphone-based urine reagent strip reader was developed based on previous studies, 8 –12 and urine samples were collected from subjects who visited the ED. With clinical urine samples, the proposed reader was also evaluated in the clinical setting as follows: to assess the reliability of the smartphone-based reader, the detection performance of LE and NIT was compared with that of a reference photometric analyzer. To evaluate the efficiency of the proposed reader, turnaround times (TATs) for analysis and the time for the entire study procedure were also compared between the two devices.
Materials and Methods
This study protocol was approved (registration number H-1312-118-545) by the Institutional Review Board at Seoul National University Hospital, Seoul, Republic of Korea. The study was carried out in accordance with the 63th Declaration of Helsinki of the World Medical Association as revised in September 2013.
Hardware
To design the smartphone-based reader, two main structures would be required: the mobile platform and the smartphone to capture the image sequence of region of interest (Fig. 1). First, a mobile platform was made with the goal of maintaining the same measurement conditions during each repetition of the test. This platform was made of an opaque black poly(methyl methacrylate) (Plexiglas®; Arkema Group, Bristol, PA) 155 × 155 × 88 mm in size (Fig. 1). As shown in Figure 1, the smartphone is laid on the top of the platform on an opening to perpendicularly analyze regions of interest at a constant distance. In this study, the iPhone® 4 (Apple, Cupertino, CA) was used as the smartphone. Within the platform, a white light-emitting diode was set as a light source to keep a constant light condition. A reference color chart (Multistix® 10 SG; Siemens Medical Solutions, Forchheim, Germany) was also set in the platform. As shown in Figure 1, this fixed, horizontal alignment allowed each position of the urine reagent strip to be easily compared with corresponding reference colors on the reference color chart.
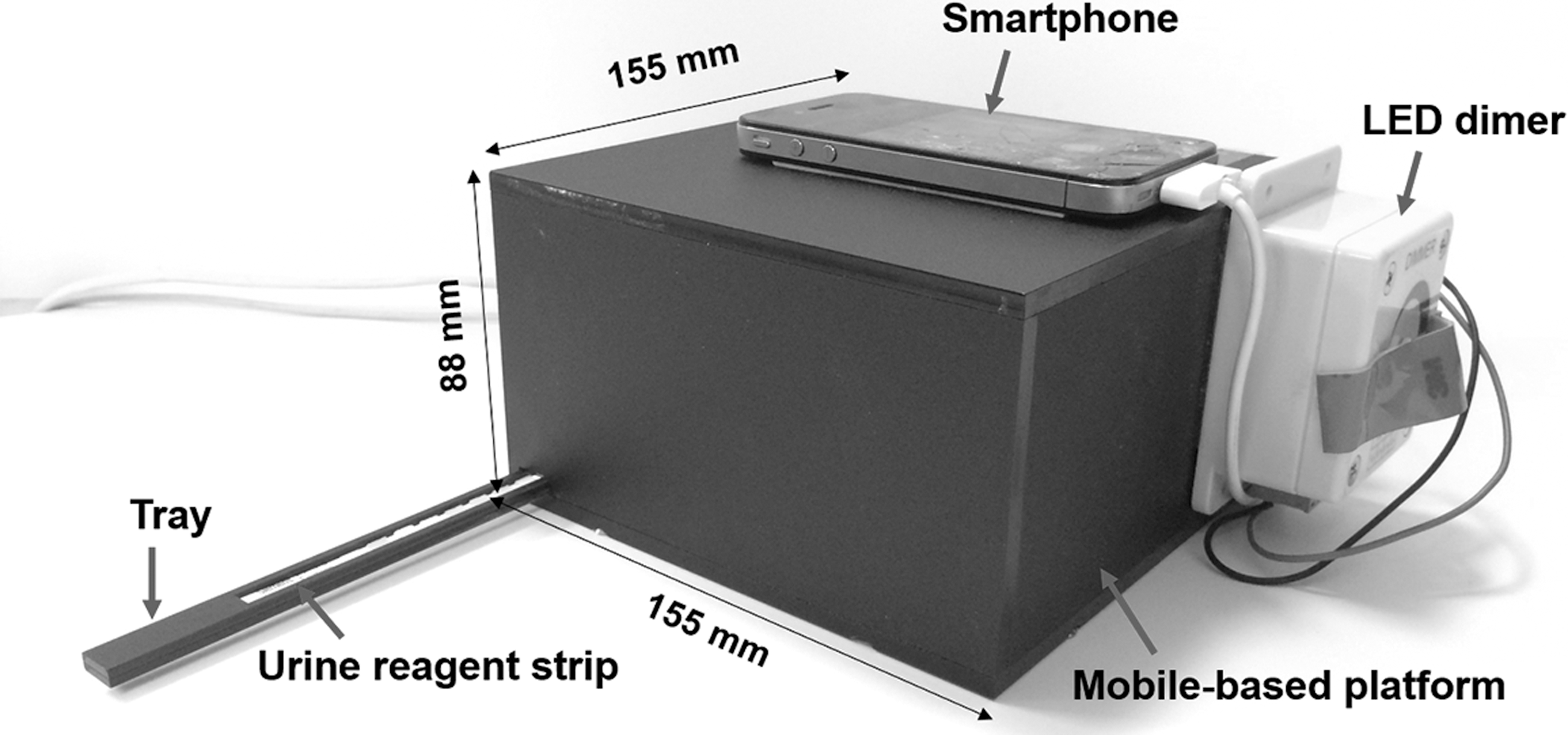
Developed smartphone-based reader and mobile-based platform. LED, light-emitting diode.
Subjects and Procedure of Study
Between August 2014 and March 2015, urine samples were collected from patients presenting at the ED of Seoul National University Hospital. Patients were included who presented to the ED in the period of study who had urinalysis ordered by the attending emergency physician regardless of symptoms and who consented to participate in the study. Patients were excluded if they did not agree to participate. Written informed consent was obtained from all the participants before any study-related procedures were performed.
A preliminary study of 12 subjects was performed in order to establish the criteria for the image processing. For the final evaluation of the smartphone-based urine reagent strip test, we aimed to have at least 84 subjects. We arrived at this number based on the results of a recent published study (n = 69) 12 plus a 20% expected failure rate. Of our samples, 3 were excluded due to an unstable Wi-Fi network, and we were left with a total of 81 urine samples to include in the study. The main demographic characteristics are described in Table 1.
Characteristics of Enrolled Subjects
SD, standard devation; UTI Hx, personal history of urinary tract infection.
Figure 2 illustrates the schematic procedure of our study. As shown in Figure 2, a portion of a given urine sample was used to evaluate the proposed reader, and the other portion was sent to the urine laboratory of the Department of Laboratory Medicine at Seoul National University Hospital for analysis. In the laboratory all urine samples were analyzed by automated semiquantitative urinalysis (model US-3100R Plus®; Eiken Chemical, Ltd., Tokyo, Japan), the results of which are then used as a reference in this study.

Schematic process for analysis of the urine reagent strip test using the smartphone-based reader in the emergency department (ED) and the photometric analyzer (model US-3100 Plus) in the central laboratory.
Urine Reagent Strip Test Using the Smartphone-Based Reader
Preparation of urine samples
Urine samples collected from the patients were extracted in a sterile syringe by a researcher. Then the urine sample in the sterile syringe was applied to the assigned positions for LE and NIT on the Multistix 10 SG urine reagent strip.
Capture of image sequence using the smartphone-based reader
A researcher captured the image of regions of interest with the same conditions for distance and luminance as for the calibration points and maintained a set protocol for all the samples. Figure 3 illustrates the overall procedure of urine reagent strip test analysis using the smartphone-based reader. The steps for the operator of the device included the following: (1) execution of a self-timer camera application (GorillaCam; Joby®, San Francisco, CA); (2) inserting the prepared urine reagent strip into the platform; (3) capturing the urine reagent strip as well as the reference chart during a 2-min period per 30 s; and (4) execution of the storage service application Dropbox (Dropbox, San Francisco). Through Steps 1–4, in total, five images were acquired by the reader. Acquired image sequences were saved in the smartphone as well as automatically uploaded into a predesignated folder. The subsequent image analysis for detecting presence of LE and NIT was automatically performed using MATLAB® software (The Mathworks, Natick, MA) on a personal computer (see Supplementary Data; available online at

Schematic procedure of analysis of the urine reagent strip test using the smartphone-based reader:
Evaluation of the Reliability of the Smartphone-Based Reader
Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) were estimated to validate the performance of the smartphone-based reader according to the following equations:
where TP is true positive, which denotes the number of positive for NIT or LE measurements from the photometric analyzer correctly identified as that of NIT or LE from the smartphone-based reader; FN is false negative, which denotes the number of positive for NIT or LE measurements from the photometric analyzer incorrectly identified as negative; TN is true negative, which denotes the number of negative NIT or LE measurements correctly identified as negative for NIT or LE; and FP is false positive, which denotes the number of negative NIT or LE measurements incorrectly identified as positive for NIT or LE.
Statistical analysis was performed using SPSS version 20.0 software (SPSS, Chicago, IL). Kappa (κ) analysis was performed to assess the agreement of detection performance between the two devices: a κ value of 0.40 was considered poor-to-fair agreement, that of 0.41–0.60 was considered moderate agreement, that of 0.61–0.80 was considered substantial agreement, and that of 0.81–1.00 was considered excellent agreement. 15 The Wilcoxon signed ranks test was used to establish differences in TATs. A value of p < 0.05 was considered statistically significant.
Evaluation of the Efficiency of the Smartphone-Based Reader
To evaluate efficiency of the smartphone-based reader, TAT was calculated for each device. TAT of the reader was denoted as the duration from the start of the test to the final report of the result. Because analysis by the smartphone-based reader was performed in the ED, additional time was not required, which in turn meant that the TAT of analysis was as the same as that of the entire study procedure. In contrast, analysis by the photometric analyzer was performed in the urine laboratory of the Department of Laboratory Medicine at the same hospital, which required additional time for delivering the samples. Thus, TATs of the photometric analyzer were separately calculated for analysis and for the entire study procedure: TAT for analysis was denoted as duration from receipt of a urine sample at the urine laboratory of the Department of Laboratory Medicine to the final report of the result, whereas TAT for the entire study procedure was denoted that from the start of the test to the final report of result (i.e., TAT for analysis in addition to time required for delivering urine samples).
Results
In total, 81 urine samples were analyzed by the smartphone-based reader and the photometric analyzer. According to the analysis result using the photometric analyzer, LE is more prevalent than NIT in the urine samples: the prevalence of LE was 21.0% (95% confidence interval [CI], 13.0–31.6%), and that of NIT was 8.6% (95% CI, 3.8–17.2%).
Evaluation of the Accuracy of the Smartphone-Based Reader
Table 2 summarizes the results on the detection performance for LE and NIT in the smartphone-based reader compared with those in the photometric analyzer. As shown in Table 2, the proposed reader reveals accuracies (i.e., percentage of correct detection for both positive and negative of the reagent) of 85.2% (95% CI, 75.2–92.0%) for LE and of 97.5% (95% CI, 90.5–100.0%) for NIT. In addition, the reader exhibited excellent agreements with the photometric analyzer (κ coefficient of LE = 0.903 [95% CI, 0.781–1.000]; κ coefficient of NIT = 1.000 [95% CI, 1.000–1.000]) (Table 2).
Results of Urine Reagent Strip Tests Using a Smartphone-Based Reader Versus the Photometric Analyzer (Model US-3100 Plus)
Positive, negative, and total values are numbers of strips.
NPV, negative predictive value; PPV, positive predictive value.
Evaluation of the Efficiency of the Smartphone-Based Reader
To evaluate the efficiency of the smartphone-based reader, TATs of the reader were calculated and compared with those of the photometric analyzer (Fig. 4). As depicted in Figure 4, median TAT for analysis in the reader was 3.0 min (interquartile range [IQR], 3.0–4.0 min). In contrast, a higher median TAT of 33.0 min (IQR, 26.5–42.0 min) for analysis was observed for the photometric analyzer. Thus the smartphone-based reader's median TAT was 11-fold faster than that for the photometric analyzer (p < 0.001) (Fig. 4). TAT of the entire study procedure for the reader was about 20-fold less than that of the median time for the photometric analyzer (3.0 min [IQR, 3.0–4.0 min] versus 62.0 min [IQR, 49.5–75.0 min]; p < 0.001) (Fig. 4).
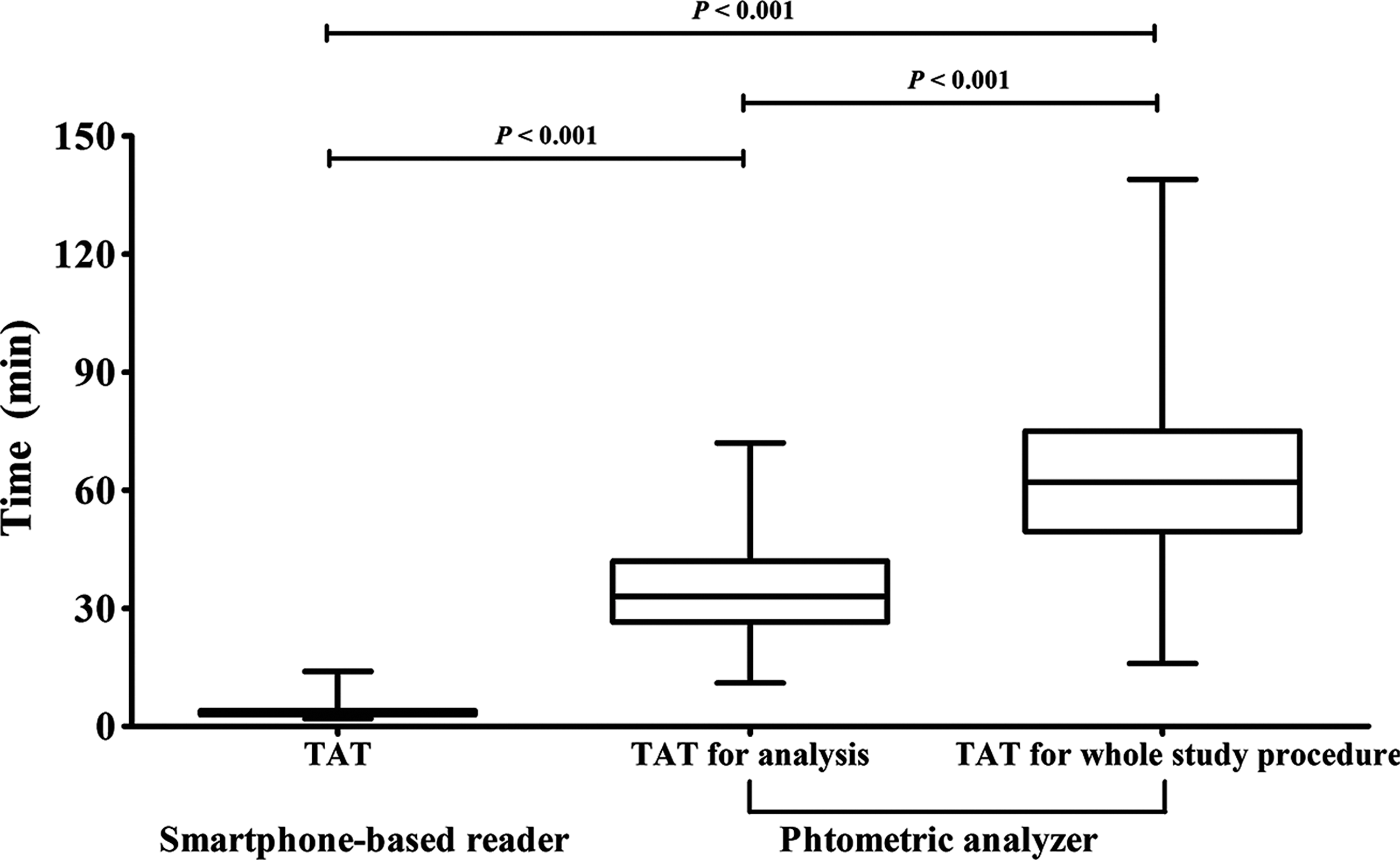
Comparison of turnaround times (TATs) for analysis and the entire study procedure between the smartphone-based reader and the photometric analyzer (model US-3100 Plus).
Discussion
In this study we developed a smartphone-based urine reagent strip reader that can detect the presence of LE and NIT, which are important indicators for UTI. Notably, we also collected clinical urine samples and evaluated our reader with these samples. This is the first published study to evaluate a smartphone-based reader with clinical urine samples. Compared with a conventional photometric analyzer, our device demonstrated that it gives reliable results (Table 2).
A mobile platform with a smartphone was developed that allows maintaining a constant capturing conditions and hence reduced measurement variability such as camera focus, camera angle, and lighting conditions. 11 In addition, freely accessible, simple, and widely used tools (i.e., GorillaCam and Dropbox) were used in this study. A Gorilla application was selected for a continuous shooting mode with an adjustable interval, and Dropbox was selected due to its simple file-synchronization function. 16 With the help of these applications, the study and analysis were easily carried out. As the procedure is not complicated, a minimally trained technician can perform the test with just a few clicks. In addition, data analysis can be fully and automatically executed so that highly trained personnel would not be required for the analysis. We believe that this reader offers a low-cost alternative for a priori screening in a clinical environment such as a busy ED of patients who are suspected of having UTI.
We also compared the TATs of the smartphone-based reader with those of a photometric analyzer. The reader reduced about 11-fold the median TAT for analysis as well as about 20-fold the median TAT for the entire study procedure compared with a photometric analyzer (Fig. 4). These differences in the TAT may be due to the following: The smartphone-based reader can analyze the urine samples on site. On the other hand, in a given ED environment, the urine samples are collected as a batch and then carried to the department of laboratory medicine at the same hospital for analysis, which requires time for delivery. Additional time can also be consumed in identifying the urine sample or feeding the urine samples to the photometric analyzer. It is also noted that even though the photometric analyzer performs the LE and NIT test almost instantly, the results of analysis for a digital medical record are reported only after microscopic urinalysis results are completed as well. Considering the busy ED environment, the delivery of urine samples is frequently delayed, and if there is a backlog in the department of laboratory medicine, more delay is to be expected. The proposed reader with this rapid detection time is expected to allow a timely analysis for UTI in patients and a timely reporting of results. This is valuable compared with other studies 8 –12 that reported and evaluated other smartphone-based urine reagent strip readers at the laboratory level.
There are some limitations to our study. Although our reader showed high sensitivity and accuracy, it is difficult to conclude that the reader is accurate for diagnosing UTI. This is because the analyzed results from our smartphone-based urine reagent strip reader were not directly compared with those from previous studies where urine cultures, the standard of diagnosing UTI, were used. However, the purpose of this study was not to validate the proposed reader in diagnosis of UTI but to compare the reliability and the efficiency of the proposed reader with those of a photometric analyzer, as a rapid screening tool for detecting urine LE and NIT. Therefore this limitation does not reduce the merits of the study.
In addition, sensitivity and PPV of LE showed relatively low values even though the overall results showed a relatively high accuracy (Table 2). These relatively low values may due to the difficulty in decision-making in the case of LE results showing “trace.” In previous studies 17,18 relating the urine reagent strip test to diagnosis of UTI, the “trace” value was usually taken as “positive,” which we believe that it could have contributed to the lower sensitivity and specificity because “trace” meant labeling the sample an ambiguous reading. If we obtain more color information regarding LE for the urine reagent strip through the reader and have more accurate criteria for determining LE levels, we believe that this limitation could be resolved. In addition, our results also showed high sensitivity and specificity for NIT. When a patient is suspected of having UTI with positive LE and NIT, a physician should prescribe antibiotics before the result from a urine culture is reported, and then the final diagnosis of UTI can be confirmed by the urine culture. Therefore we think that the relatively low sensitivity for LE of the proposed reader would not be a problem for the required clinical performance. Furthermore, three urine samples in the test set were excluded because analysis did not work normally due to an unstable Wi-Fi environment. An advanced reader undisturbed by network problems is required.
Conclusions
In spite of these limitations, our smartphone-based urine reagent strip reader showed good reliability for detection of both LE and NIT and demonstrated a noteworthy reduction of TATs, compared with the photometric reader. It is concluded that our results validate the clinical capability of the smartphone-based urine reagent strip test in the clinical environment, and this reader is expected to enable a more rapid and reliable colorimetric test for screening of LE and NIT in the clinical setting and at the point of care, without the risk of conversion of the urine samples. Our device was also economical for cost saving in terms of materials used and the efficiency gains in detection compared with expensive photometric analyzers.
Footnotes
Acknowledgments
This study was supported by the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (grants HI13C1468 and HI14C0559) and by the BK21 Plus Program through the National Research Foundation of Korea funded by the Ministry of Education (grant 22A20130011025).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.