
Abstract
Introduction
With the aging population, joint replacements such as total knee arthroplasty (TKA) are surgical procedures that are increasingly in demand worldwide. 1 Rehabilitation provided through home visits is part of the continuum of care after discharge from hospital following TKA. As demands for rehabilitation at home are growing and becoming more difficult to meet, evidences supporting the use of telerehabilitation as an alternate or complementary service delivery method are emerging. 2,3
Telerehabilitation, defined as “the use of Information and Communication Technologies (ICT) to provide rehabilitation services to people remotely in their homes or other environments,” 4 can be provided as a store-and-forward or real-time interactive service and varies from teleconsultations between professionals to remote evaluations and teletreatments of patients. 5
ICT needed to support telerehabilitation vary with the context of care provided (teleconsultation vs. teletreatment), the intervention (physical therapy, occupational therapy, speech and language therapy), and the synchronicity of the intervention (store-and-forward, real time). Teletreatments are often based on interactive synchronous audio/video (A/V)-mediated communication between patients and clinicians using videoconferencing over telecommunication networks and the Internet. 6 They may be delivered between two healthcare centers or between a healthcare center and the patient's home (in-home teletreatment). Videoconferencing for teletreatments encompasses a two-way use of video (cameras) and audio (microphone) capture equipment, compression and decompression of digitally captured streams of audio and video in real time using a coder–decoder (CODEC), and transmission of the compressed video and audio signal over a network. 7 Technological advances in videoconferencing, increases in bandwidth (BW) of telecommunication networks and reduced costs of ownership, have provided opportunities for the development and application of in-home rehabilitation teletreatments for different patient populations. 8
Although interactive synchronous A/V-mediated communications using videoconferencing is now a well-accepted form of communication for different domains of applications, its reliability and quality under real-world conditions of rehabilitation teletreatments have not been studied. In the context of A/V-mediated communication during in-home rehabilitation teletreatments, there are marked changes in the technical and interpersonal contexts within which communication takes place that can affect the usability of providing in-home teletreatments with videoconferencing. Usability as defined by the International Organization of Standardization (ISO) standard 9241-11 is “the extent to which a product can be used by specified users to achieve specified goals with effectiveness, efficiency and satisfaction in a specified context of use.” 9 The quality of the videoconferencing experience is at the forefront of the usability of A/V-mediated communication 10 –12 and can be modeled as a multidimensional construct with specific attributes. Lerouge et al. proposed a taxonomy of these attributes and described them extensively. 13,14
Building on the work of Lerouge et al., 13 the quality of the videoconferencing experience ( Fig. 1 ) can be seen as a combination of five factors: (1) the telecommunication network supporting the videoconference, (2) the videoconferencing technology used, (3) the usability of the technologies used, (4) the physical environment where the videoconferencing occurs, and (5) the human elements that can facilitate the videoconferencing experience. Reliability and performance of the telecommunication network and the videoconferencing technology are key metrics in the quality of the videoconference experience. For interactive A/V-mediated communication between patients and clinicians, a lack of reliability or performance in the telecommunication network and videoconferencing technology can not only impact the specific encounter in which it occurs but it also leaves a long-lasting impression on users (clinician and patients), which can negatively affect the perceived usefulness and ease of use of providing in-home teletreatments and ultimately impact acceptance of this mode of service.
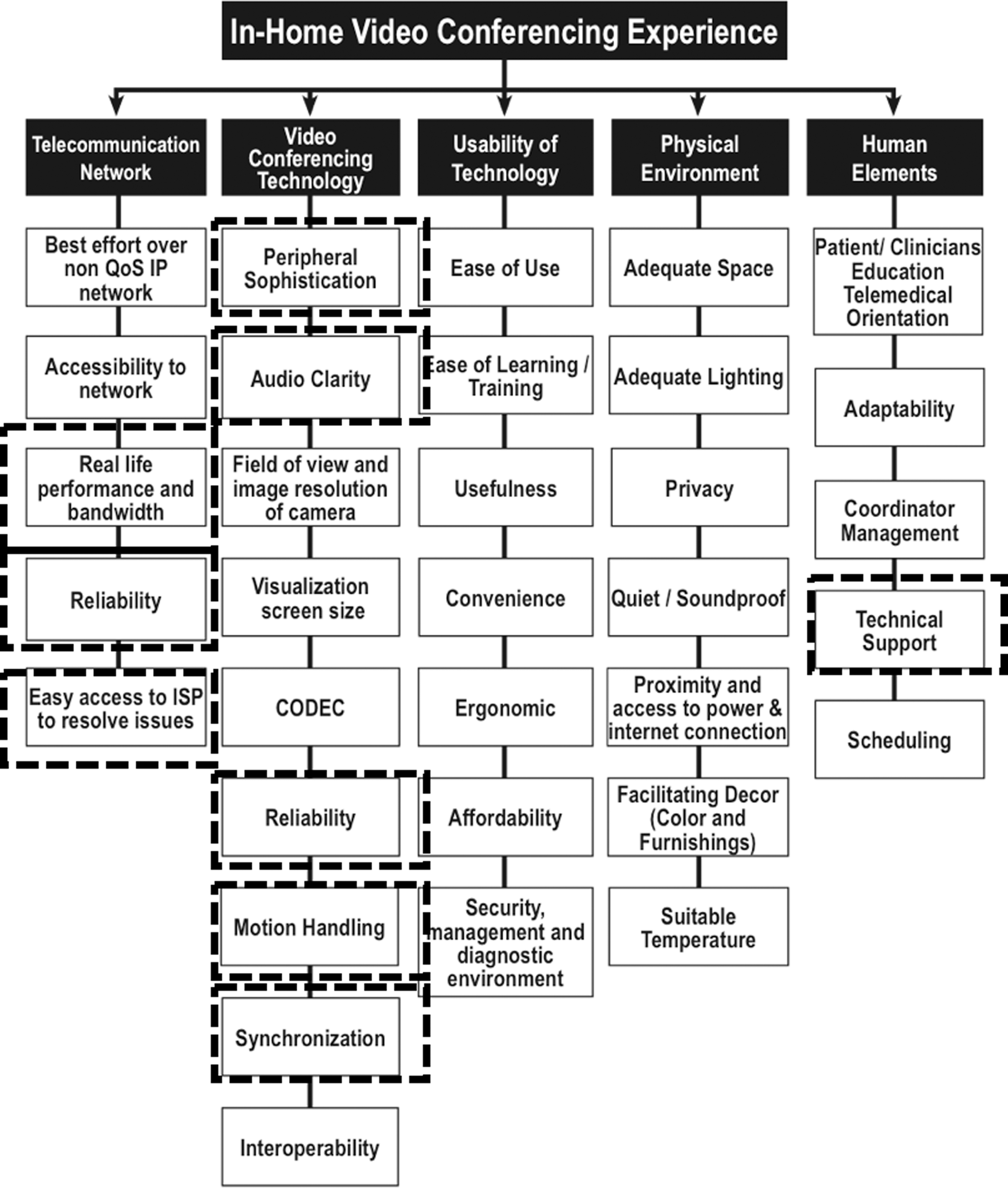
Quality attributes for in-home videoconferencing. Adapted from LeRouge et al. 13 with some additions.
The conditions of use, reliability, performance, and usability of interactive video-mediated communication during teletreatments have not been studied extensively and not specifically in the context of in-home telerehabilitation. The objectives of this study were to (1) document the conditions of use, performance, and reliability of interactive videoconferencing-based communication between patients and providers in the context of in-home teletreatments (TELE) following TKA and (2) assess from the perspective of the providers, the quality attributes of the technology used and its impact on clinical objectives.
This study was embedded in the TelAge randomized controlled trial (RCT) on the effectiveness of delivering in-home telerehabilitation following TKA. Details about the results of the TelAge RCT on the clinical efficacy and cost of providing in-home telerehabilitation can be found elsewhere. 15,16 Briefly, clinical results from 205 patients with TKA randomized to receive in-home telerehabilitation or face-to-face visit showed that after a 2-month rehabilitation program at the last follow-up, the mean differences between the groups with respect to the primary outcome (WOMAC gains adjusted for baseline values) were close to zero and slightly in favor of the TELE group, proving the noninferiority of the in-home telerehabilitation intervention. 15 Results from an economic analysis based on a health sector perspective (costs relevant to the patient not considered) showed a cost differential in favor of the TELE group when the distance of the home was 30 km or more. 16 This article presents results specific to the conditions of use, quality, performance, and reliability of the technology used to deliver the in-home telerehabilitation intervention in the experimental arm of the TelAge RCT.
Materials and Methods
Design and Participants
The TelAge RCT ran from 2008 to 2012 and involved three research centers and eight hospitals located in Sherbrooke, Quebec City, and Montreal in the province of Quebec, Canada. Ethics committees of each hospital approved the TelAge RCT and the participants' written consent was obtained before their inclusion. Patients scheduled for TKA were recruited before surgery and eligibility was verified using the following criteria: (1) waiting for a primary TKA after a diagnosis of osteoarthritis; (2) returning back to their home after hospital discharge following TKA; (3) access to a wired high-speed Internet connection at home (min 512 kilobits per second [Kbps] in upload); and (4) living less than 1-h driving distance from the primary care hospital. Patients were excluded if they (1) had health conditions that could interfere with tests or the rehabilitation program; (2) were planning a second lower limb surgery within 4 months; (3) had cognitive or collaboration problems; (4) had major postoperative complications; or (5) had weight-bearing restrictions for a period longer than 2 weeks postsurgical intervention. Patients meeting these criteria were recruited and then randomized to physical therapy provided face-to-face at home (VISIT) or in-home telerehabilitation provided remotely (TELE).
Telerehabilitation Intervention
The experimental arm (TELE) of the TelAge RCT consisted of providing remotely through a telerehabilitation platform two 45–60-min physical therapy sessions per week for 8 weeks (16 sessions total). The components of the TELE intervention were as follows: a pre- and postexercise assessment (structured interview and observation), supervised exercises during a period of about 30 min (mobility, strengthening, function, and balance), prescription of home exercises to perform on days without supervised sessions, and advice concerning pain control, walking aids, and the return to activities. The telerehabilitation platform used for the provision of care included various components to provide a user-friendly videoconferencing experience for both the clinician and the patient at home ( Fig. 2 ). The core of the platform was a videoconferencing system (Tandberg 550 MXP), which uses a H.264/AVC CODEC and incorporates a pan-tilt-zoom wide-angle camera and omnidirectional microphone. In the patient's home, the system was mounted over a 20-inch LCD screen, which displays the video received from the clinician. Audio was played using external speakers placed on both sides of the screen. On the clinician side, a computer with dedicated software (TeRA) is added to the videoconference link to enable user-friendly control using a computer mouse of videoconferencing sessions, near and far end camera controls (pan, tilt, zoom), picture in picture and local and remote display of camera sources, built-in clinical tests, and photo and video recordings. Video and audio data were encrypted (AES 128-bit encryption) and transmitted over a high-speed Internet connection. The clinician telerehabilitation platform was installed at one location (closed office in a dedicated room at each research center) per geographical site. Physical therapists (PTs) providing the services booked directly their appointment with the patients and reserved the room for the time period of the treatment.
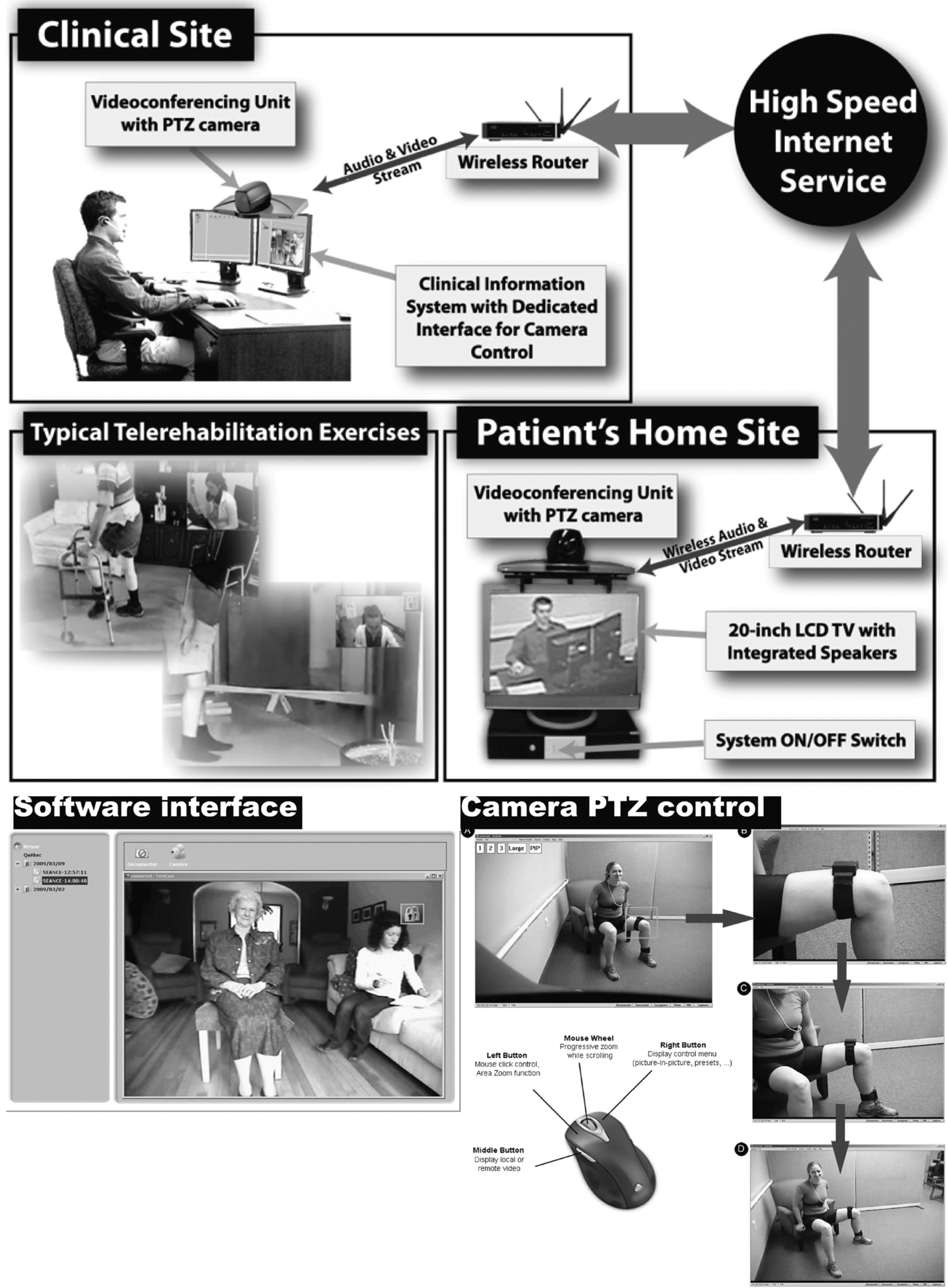
Overview of telerehabilitation platform and component used during the TelAge RCT. PTZ, pan-tilt-zoom; RCT, randomized controlled trial.
PTs providing services and patients receiving the telerehabilitation services were trained on the use of the platform (training time for therapist was 90 min, training for patient at home was 10 min). Before discharge from the hospital, depending on the presence or absence of an Internet connection at the home of the patients and on the BW available, arrangements were made through a telecommunication broker with links to multiple Internet service providers (ISPs) to schedule installation/activation or upgrade of services for the duration of the project. Based on previous experiences in another RCT on in-home teletreatments, 17 cable network installations or upgrade were privileged over Digital Subscriber Line (DSL) network by the research team. After installation or upgrade to the Internet service, a technician from the research team drove to the patient's home and proceeded to (1) analyze the placement of the equipment in the home; (2) create or expand a secured wireless network connecting the telerehabilitation system to the existing Internet connection; (3) install and configure the different components of the system in the home; (4) test the connection between the remote clinical site system and the patient's home system; (5) assess the BW and reliability of the Internet connection between the remote clinical site system and the patient's home system during a connection scenario (15-min tests); and (6) train the patient on the sequence of operation of the system (on/off). At the time of the TelAge RCT, ISPs in Quebec offered high-speed Internet connections through DSL or cable with varying download BW (1–8 Mbps) but they were limited theoretically in upload BW to 800 Kbps with real-life upload BW closer to 600 Kbps. Since the CODECs used in the TelAge trial (H.264/AVC) did not have scalable capabilities, connections were thus capped at 512 Kbps with 64 Kbps allocated for audio and a maximum of 448 Kbps allocated to video.
Measures
Technical support need and service delivery reliability
As the TelAge RCT included analysis of costs of delivering the in-home telerehabilitation intervention, 16 a standardized log of events per participant was maintained by the PTs and technological support personnel throughout the delivery of the interventions for each TELE session. Variables accounted for in the log were (1) if a new Internet connection was installed (yes-no); (2) the type of Internet connection provided (cable-modem); (3) the total time (including travel time from the hospital to the home and back) spent by technicians for the installation, test of the equipment, training of the patient on the equipment, and its removal at the end of the intervention; (4) the proportion of planned TELE sessions completed (number of sessions provided in TELE/number of TELE sessions in the rehabilitation program; (5) the planned TELE sessions with technological problems requiring technical support; (6) the average time spent for technical support interventions during planned TELE sessions. Results were computed for all planned and/or delivered telerehabilitation sessions provided for all participants and per geographical region (Sherbrooke-SHER, Quebec-QC, and Montreal-MTL).
Performance and use of network connection
Network use for each telerehabilitation session provided during the TelAge RCT was extracted from upstream and downstream statistics, and logs provided by the videoconference CODECS and the routers connected to Internet at both sites (patient's home and clinical site). Data were stored and aggregated per session. For each TELE session, real-time connection (time when both videoconferencing systems were connected), dead time not connected (time when the clinician videoconferencing system was active and trying to connect to the patient's videoconference system during a planned TELE session), and number of connection interruptions during the session were computed and averaged for all planned and/or delivered telerehabilitation sessions provided. Dead time included time spent to solve technical problems occurring during a planned session until the session was given or had to be rescheduled. Average upload BW during each TELE session extracted from the patient's home CODEC and used as an indicator of BW expressed as % of the BW allocated. Results for performance and use of network connection were computed for all participants and per geographical region (SHER, QC, and MTL).
Technological impacts on video-mediated communications and clinical objectives
The quality of A/V-mediated communications and the impacts on clinical objectives was assessed after each session by asking the treating clinicians after each TELE session a series of questions on specific variables (Appendix 1). PTs were asked to subjectively rate their appreciation of the technical quality of A/V-mediated communications during the session, using a four-point Likert scale on five key aspects: (1) quality of the overall technical environment; (2) quality of the image/voice synchronization; (3) quality of the image frame refresh rate; (4) quality of the sound; and (5) quality of the operability of the peripherals during the session. The variables chosen were taken from existing questionnaires previously used to assess the quality of videoconferencing. 11,14 Scoring for each variable was based on a gradation of quality (low, insufficient, acceptable, good). Likert levels were associated with the presence and frequency of occurrences of events detrimental to the quality of the measured variable and if these events had or not an impact on the treatment quality. PTs were also asked after each session to subjectively rate on a scale of 0–10; (1) their satisfaction with the communication with the patient; (2) their appreciation of the relationship with the patient; and (3) the attainment of clinical objectives. An electronic form containing the questions was automatically generated after discontinuation of the TELE session and answers for a given session were stored on a database with a timestamp. The results are reported as % of session for each scaling item on the five aspects of the technical quality of A/V-mediated communications and as a % of the session in the scaling categories of the clinical workflow aspects for all participants and per geographical region (SHER, QC, and MTL).
Statistical Analyses
Descriptive statistics (%, frequency, mean, standard deviation [SD]) were computed for all participants included in the per protocol analyses of the TelAge RCT and for subgroups in the three geographical regions (SHER, QC, MTL). Kruskal–Wallis tests with pairwise comparisons between geographical regions were computed on the % scores for the appreciation of the technical quality of A/V-mediated communications and on the perception of the technological impacts on the clinical objectives after each session. A p-value of 0.05 was considered in these analyses. All analyses were performed using IBM SPSS v21.
Results
A total of 258 patients discharged from the hospital following TKA were recruited in the TelAge RCT. Postsurgery, 53 patients were excluded and those who remained (n = 205) were block-randomized to the TELE group (n = 104) or VISIT group (n = 101). Seven of the TELE group participants were excluded for lost at follow-up evaluations, and thus, the final sample for TELE group was n = 97. The sociodemographic characteristics of the patients who received the TELE intervention (n = 97) and the PTs (n = 14) who provided the teletreatment are presented in Table 1 .
Description of Conditions for Provision of In-Home Telerehabilitation and Sociodemographic Characteristics of Participants and Clinicians Who Delivered the Telerehabilitation Interventions
MTL, Montreal; QC, Quebec; SD, standard deviation; SHER, Sherbrooke.
Patients (n = 97 with 58% male and a mean of 65 years of age) received from 14 physiotherapists (mean age 33 years, 50% male) a total of 1,431 telerehabilitation sessions (about 15 sessions per participant) on the three sites (363 sessions in Quebec city, 830 sessions in Sherbrooke, 238 sessions in Montreal). Installation of a high-speed Internet connection was necessary for 75% of the participants and 84% of all the connections were on a cable network. An overview of the conditions of service delivery, reliability, and technical support need during the provision of telerehabilitation services is presented in Table 2 . The mean total installation/removal time of the telerehabilitation platform by technical personnel for all participants, including return travel time to the participant's home for the installation and removal, the configuration of the equipment on the network, on-site test of the quality of the connection, and the removal of the equipment was 308 min, with an SD of 123 min. Planned telerehabilitation sessions were successfully delivered for 96.5% of the rehabilitation program scheduled (n = 16 sessions) and lasted on average 45 min (SD: 11 min), with an average of 5 min of dead time (SD: 29 min). Dead time included the waiting period on the PTs side to connect to the patient at the allocated time and the connection interruptions in the session, which included the time needed to get access to technical support and the time spent by the technical support personnel to try to resolve the issues. When the technical support interventions did not succeed in establishing the conditions to provide the service, the TELE session was rescheduled later in the day or the next day. If the problem persisted beyond this, the planned TELE session was replaced by a VISIT session and considered as cancelled. Connection interruption per session occurred at least once in 21% of the telerehabilitation sessions delivered. Technical support was required in 43% of the sessions (before, during, or after), but the time of these interventions was about 3 min (2.8 ± 6.1 min). The use of telecommunication network during the provision of in-home telerehabilitation shows that the average total BW used per session of telerehabilitation (expressed as a percentage of the 512 Kbps connection speed set by the CODEC) was 77%.
Technician Time for Installation and Uninstallation of Platform, Reliability Technical Support, and Network Bandwidth Needs in the Provision of In-Home Telerehabilitation (N = 1,431 Sessions)
BW, bandwidth; Kbps, kilobits per second.
Subjective appreciation by treating PTs on the technical quality of A/V-mediated communications during telerehabilitation sessions (1,309 completed questionnaires out of 1,431 sessions) is presented in Figure 3 . Results are reported as % of session for each scaling item on five aspects for all participants and per geographical site. The details of the scales used are presented in Appendix 1. Over all the sessions performed, the appreciation of the quality of the overall technical environment was good (no dropped service and/or technical instabilities) in 80% of the TELE sessions evaluated and judged insufficient (significant presence of dropped service and/or technical instabilities, leading to important impact on treatment quality) in 3% of the rest of the sessions. The appreciation of the quality of the image/voice synchronization was good (the image/voice synchronization adequately supported communications with the patient and met the required needs during the session) in 84% of the TELE sessions evaluated and insufficient (the image/voice synchronization rendered communication with the patient difficult several times during the session and had an impact on treatment quality during the session) in 2% of the rest of the sessions. The appreciation of the quality of the image frame refresh rate was also good (punctual presence of short delays in refresh rate, with no impact on treatment quality or noticeable delay in refresh rate) in 84% of the telerehabilitation sessions evaluated and insufficient (presence of short delays in refresh rate repeated during the entirety of the session, with an impact on treatment quality) for 3% of the rest of the sessions. The appreciation of sound quality was good (the intelligibility of sounds transmitted supported adequately communication with the patient met the required needs during the session) for 85% of the TELE sessions evaluated and insufficient (the intelligibility of sounds transmitted and/or the existence of echo throughout the entirety of the session rendered communication with the patient impossible and had effects on treatment quality) for 2% of the rest of the sessions. The appreciation of the quality of the operability of peripherals during the session was good (no difficulties in the operation and control of peripherals) in 89% of the telerehabilitation sessions evaluated and insufficient (punctual difficulties in the operation and control of peripherals during treatment, leading to important impacts on treatment quality) in 1% of the rest of the sessions. Small but statistically significant differences (values in red on the graphs for Fig. 3) on the subjective appreciation of the technical quality of A/V-mediated communications during in-home telerehabilitation between geographical sites were found on four of the five variables (Kruskal–Wallis test with pairwise comparisons between sites p < 0.005). The appreciation of the quality of the overall technical environment was judged better (% good and % acceptable higher) at the QC site then the other two sites (SHER, MTL). The appreciation of the quality of the image/voice synchronization and the appreciation of sound quality during the sessions were judged slightly lower at the SHER site than the other two sites (% good and % acceptable lower). The appreciation of the quality of the image frame refresh rate was judged better (% good higher) at the MTL site than the other two sites (SHER, QC).
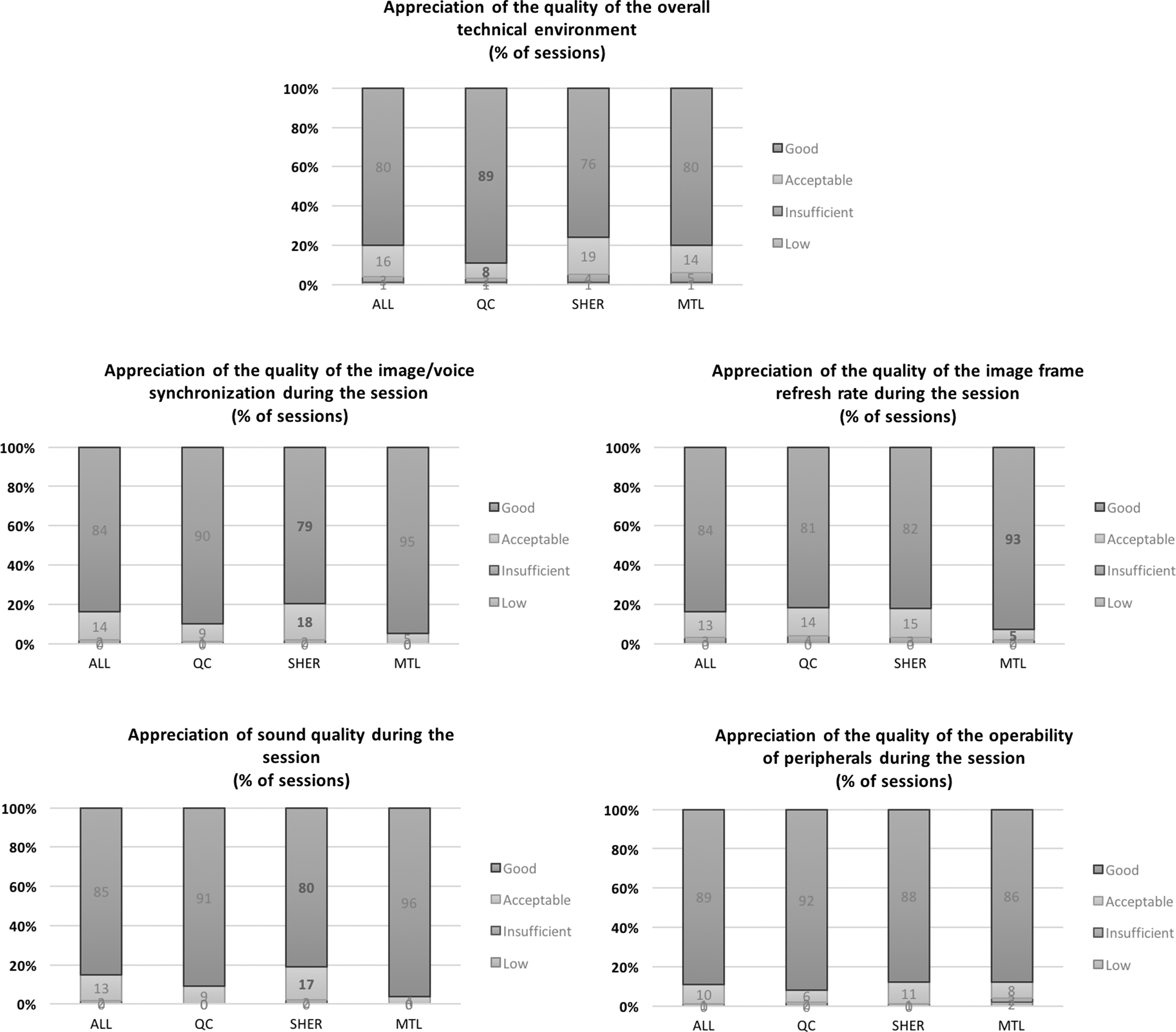
Subjective appreciation by treating PTs on the technical quality of A/V-mediated communications during telerehabilitation sessions. Results are presented as % of sessions performed in total and per geographical site. A/V, audio/video; PTs, physical therapists.
Subjective appreciation by treating PTs on the technical impacts of A/V-mediated communications on the clinical workflow during telerehabilitation sessions is presented in Figure 4 . Clinicians were very satisfied with the flow of communication with 92% of the sessions scoring >8/10. Their evaluation of the clinician–patient relationship under the conditions of in-home telerehabilitation was also very positive with 97% of the session scoring >8/10. In 99% of the sessions under the conditions of in-home telerehabilitation, clinicians judged that they were able to reach their clinical objectives completely or almost completely (scores >8/10).
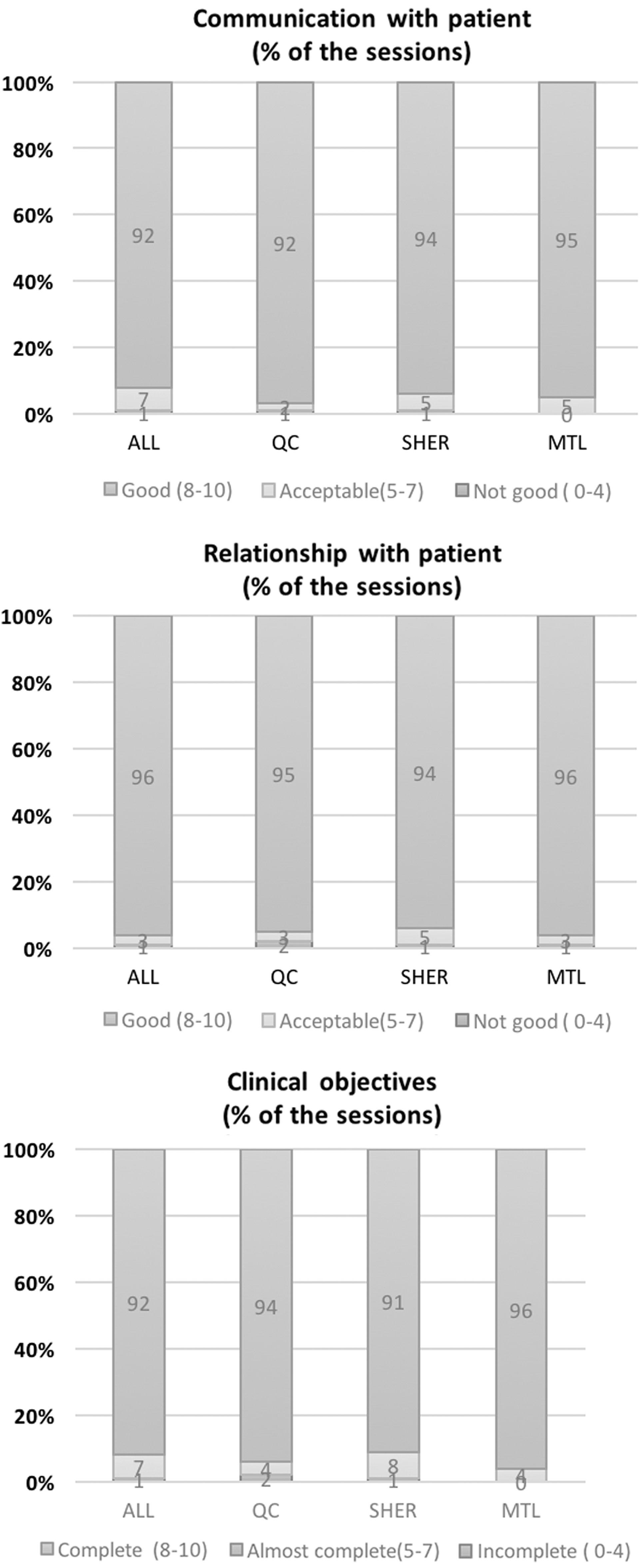
Subjective appreciation by treating PTs on the technical impacts of A/V-mediated communications on the clinical workflow during telerehabilitation sessions. Results are presented as % of sessions performed in total and per geographical site.
Discussion
This study surveyed the reliability and performance of using interactive A/V-mediated communication based on H.264/AVC videoconferencing over residential high-speed Internet connections during the provision of in-home teletreatments in the context of an RCT on post-TKA rehabilitation. Data extracted from automated logs and questionnaires during the delivery of 1,431 sessions over 97 patients located in three different geographical, mostly urban, areas in Quebec, Canada showed the conditions of operation and underlying reliability and performance that can be expected under real-world conditions of in-home telerehabilitation services.
In terms of access to telecommunication networks to support videoconferencing, the majority (75%) of patients who participated in the TelAge RCT required the installation of a high-speed Internet connection and the provision of a new contract service by an ISP. This was not expected, as data from a Canadian Internet Use Survey by Statistics Canada 18 showed that 73% of households in Quebec had home Internet access in 2010. While the TelAge RCT ran from 2008 to 2012 and since then Internet accessibility and use have improved, this is not necessarily the case for older adults. The sociodemographic characteristics of the participants may have been a factor explaining this as Internet access and use in older adults typically lag, which is observed in the overall population. 19 In the United States, recent statistics from the Pew Internet research project 20 shows that in 2013, 41% of adults older than 65 years do not use the Internet at all and 53% do not have broadband access in their homes. Undeniably, the absence of an existing high-speed Internet connection complicated the logistics of scheduling, installing, and testing the equipment needed for the provision of in-home teletreatments after discharge from the hospital in a timely manner and affected the reliability of the service delivery. Upgrading or using existing Internet connections had fewer uncertainties, although it sometimes required more work in configuring and maintaining existing home wired and wireless networks.
Although the recruitment process in the TelAge RCT for the participants included verification of their eligibility with an ISP broker (i.e., access to a high-speed Internet connection capable of supporting reliably videoconferencing at the participant's home address) or the presence of an existing high-speed Internet connection, teletreatments had to be started within 7 days of their discharge from the hospital. In the context of a new Internet connection, this meant that an ISP had to be selected and an appointment scheduled to install a functional high-speed Internet service before the installation and configuration of the telerehabilitation platform by our technician in the participant's home. Installation, configuration, equipment tests in the home environment also required the physical and virtual presence of technicians. The typical installation, including training of the patient on the use of the platform, was between 30 and 45 min. Accounting for the return travel between the home location and the hospital at both the installation and removal visits, the average technician time was about 5 h plus transportation expenses ($0.41/km [CAN]). This was acceptable under the conditions and scale of an RCT, but could certainly constitute a logistical and financial barrier to the delivery of a cost-effective intervention in a large-scale program. Indeed, cost analyses of the TelAge RCT 16 showed that the cost of a TELE session was $80.99 (CAN) with 41% of that attributed to technological costs (technical equipment amortization, installation/uninstallation of technology, Internet costs, technical problem resolution time and travel time (technician), technical problems after sessions by the physiotherapist). Installation/removal of technology represented 22.4% of the technological costs. In the context of service delivery outside of an RCT, Internet access and the initial configuration and testing of the underlying technological platform used to provide in-home teletreatment could constitute major obstacles to the generalization of this service delivery approach.
In this study, we recorded a high amount of planned sessions delivered (96.5%), with little effect on the overall service provided. It should be, however, noted that this percentage included planned sessions that were rescheduled to later in the day or the day after depending on the issues. When issues could not be resolved in a timely manner, they were cancelled; thus, cancelled sessions were a last resort. The effects of cancelled sessions on the clinical outcomes were mitigated and limited, seeing as the cancelled sessions were in turn provided in person. Cancelled planned sessions were explained mostly by contextual conditions outside of the control of the clinical team (i.e., telecommunication network performance and reliability). In this context, it is important to note that the installation of a new Internet connection affected the reliability of service, as the majority of cancelled planned sessions occurred in the first 2 weeks of teletreatments after the installation of the high-speed Internet connection. This was often due to performance issues with the network connection (mostly upload BW). Although some of these issues were related to wireless interference, and in some cases equipment failure, more often than not the root cause was at the physical and infrastructure level of the backend connection (connection of the house to the Internet, modem adjustments), requiring service calls to ISPs to solve the problems. This type of troubleshooting may be done before TKA surgery to optimize teletreatment delivery postsurgery. The reliability of providing in-home teletreatments through videoconferencing is thus not perfect. However, considering the unpredictability and relative lack of control over the technological environment and the dependence on external service providers, this success rate is surprisingly high. With the expanding availabilities and coverage of cellular telecommunication networks and their ever increasing BW, it would be plausible to consider bundling and preconfiguring the equipment required for the delivery of in-home telerehabilitation using cellular data plans. The use of a cellular modem as a gateway to support videoconferencing on the patient side could be an option, but the impacts of latency of cellular communication and reliability of connection outside urban areas (cellular coverage) have not been formally studied, and network access could also be problematic depending on the location. However, data plans over cellular networks also have much higher rates per BW usage than traditional wired ISPs, and since videoconferencing is BW-intensive, this could impact the cost of service and the scalability of this approach.
This study also provided an overview of feasibility of a teletreatment during a session and the possibility of providing a smooth, uninterrupted treatment. For teletreatment sessions that were given, connection interruptions were present in 21% of the sessions. Connection interruptions during videoconference over nonquality of service (or so-called best effort) networks like those of ISPs are common and generally expected by users who have used videoconference services over the Internet. As special care was taken to streamline the software interface so that PTs could re-establish connection easily and efficiently as patients were not required to do anything to establish the connection (connection was automatically accepted on the patient side once the system was powered on), this did not seem to affect the perception of the quality and reliability of the service. Dead time per session in minutes, which corresponds to the time when the attending PTs at a scheduled time for a given session were not connected to the patient's station, represented on average 5 min, with about 50% of that time split between waiting for the patient to turn on the system at the scheduled time and the other 50% because of reconnection attempts after a dropped connection. With respect to the scheduling, appointments were confirmed before the session by the PTs in the previous session and instructions were given to the patient to power on the system 15 min before the established time so as to enable connection tests by technical personnel if needed and to ensure that the session would start on time. Coordination with the patients and educating them on respecting this directive could contribute to reduce this dead time, which is not a lot, but can add up and become costly with multiple patients per clinician across time.
Another factor to consider for treatment interruption is the requirement of significant “glitches” requiring technical support. Technical support calls during the TELE sessions to our help desk were frequent (43% of the 1,431 sessions), but of short duration (average of 3 min). The initial training for the PTs on the telerehabilitation platform and the checklist to solve technical issue were limited (about 1 h 30 min). One hypothesis for the frequency of the calls is that throughout the duration of the project, connection problems, coupled with the learning curve associated with using the telerehabilitation platform, required a remote intervention from our technicians to confirm to the PTs that they were following the right workflow in using the platform or solving technical issues than actually solving technical issues. User training and improved documentation could reduce this dependence on technical support.
Treatment sessions could also potentially be interrupted by “traffic” on the home Internet connection. BW use on the participant's home Internet connection in upload during telerehabilitation sessions was on an average 77% of the available capped BW (i.e., 512 Kbps), reflecting that upload BW limitations were not a contributing factor in the quality of the audio/video-mediated communications. Residential high-speed Internet BW in upload at the time of the TelAge RCT (512 Kbps) was thus sufficient. With the increased upload BW offered by current residential high-speed Internet services (between 700 and 1,000 Kbps), BW does not seem to be a determining factor, but network congestion might be. This could indeed be different during peak Internet use periods (9:00, 12:00, 17:00) where anecdotal evidences from the TelAge RCT and other ongoing clinical trials on in-home teletreatments suggest that a higher frequency of performance problems occur at those hours. Scheduling in-home teletreatments outside of these peak hours thus appears warranted.
The appreciation of the performance and quality of the A/V-mediated communications during in-home rehabilitation teletreatments by the PTs was positive throughout the duration of the RCT. For 96% of the sessions, the quality of the technical environment was considered good or acceptable. Similar trends were observed for appreciation of specific technical attributes during telerehabilitation sessions such as image/voice synchronization, image frame refresh rate, sound quality, and quality of the operability of peripherals (1–3% less than good or acceptable). Outside of the cancelled sessions, with <5% of the sessions delivered presenting acknowledgeable performance issues, A/V-mediated communications during in-home rehabilitation teletreatments appear to be more satisfactory. These results are similar to those presented by Demiris et al. 11 who showed through retrospective analyses of 114 captured hospice interdisciplinary team meetings using web-based videoconferencing clients that 95% of the session presented an overall technical quality that was judged good or acceptable. Average scores for perceived video and audio quality during the sessions in both studies are also similar (>80%). It should be noted that under the conditions of the RCT, the appreciation of the performance and quality of the A/V-mediated communications by the clinicians could have been subjectively overestimated because of a participation bias. Indeed, while they had no formal experiences with the technology and this type of service delivery, PTs who delivered the in-home teletreatments could have had a positive bias toward this mode of service delivery as they volunteered and accepted to provide teletreatments.
Conclusion
The reliability and quality of interactive video-mediated communication-based on H.264/AVC videoconferencing over residential high-speed Internet connections can be considered good to acceptable for the provision of in-home teletreatments. A technical support infrastructure is required to support the delivery of in-home teletreatments. Reliability and performance issues observed were caused mostly by telecommunication problems inherent with the initial installation of Internet access and the initial configuration and tests of the underlying technological platform used to provide in-home teletreatments. Most of the issues encountered could be mitigated with the presence of an existing high-speed Internet connection in the home, with which time will be the norm even for older adults. Once the connection is there, ease of use of the platform. At this time, optimization of the processes of connecting reliable patients to the Internet, getting the telerehabilitation platform in the patient's home, installing, configuring, and testing the existing platform will be needed to generalize this approach of service delivery.
Footnotes
Acknowledgments
We thank all participants, study personnel, and orthopedic surgeons for their contribution to this project. Funding from the Canadian Institutes of Health Research (CIHR) supported this research. P.B. was supported by a Fonds Recherche Québec–Santé (FRQ-S) research scholar award.
Disclosure Statement
No competing financial interests.