
Abstract
Introduction
It is estimated that by 2030 more than 500 million people will be diagnosed with diabetes worldwide, making the disease a major long-term health challenge. 1,2 Being diagnosed with type 2 diabetes (T2D) means a twofold increased mortality rate compared to the general population and a significant risk of developing diabetes-related complications. 3,4
Today, physical activity (PA) is the first-choice treatment for T2D, 5 and optimized blood glucose management reduces long-term complications. 6 Increased diabetes-related knowledge on how to manage the disease appears to improve health- related quality of life and clinical results for patients with T2D. 7 Patients are often left alone with the responsibility of handling daily self-management of the disease. Many patients experience this as a burdensome task and lack the required knowledge or motivation, and/or skills to manage their disease over time, which is necessary for successful sustainable lifestyle changes and prevention of long-term complications. 8 Failure to meet required and subscribed rehabilitation and guidelines may result in serious complications, increased healthcare costs, and premature death. 9
An increased concentration of plasma glucose and insulin resistance leads to macro- and microvascular complications, for example, myocardial infarction, stroke, gangrene, nephropathy, and retinopathy. 3,4,10 High concentration of plasma glycated hemoglobin (HbA1c) can be used as a surrogate measure to determine how well managed the disease is. By controlling HbA1C with PA or medicine, the patient can manage and control the disease in everyday life. 11 Insufficiently controlled glycemic hemoglobin levels leads to high concentration of HbA1c in diabetics.
PA is central in treatment of patients with diabetes, and due to the chronic nature of the disease, a lifelong lifestyle approach is required. Consequently, obtaining knowledge on the maintenance of newly acquired PA habits over a longer period becomes crucial. Effective long-term physical interventions have used supervised exercise, 12,13 but this approach is expensive (although superior to no intervention for quality-adjusted life years), 14 and implementation for larger populations is limited. As a result, the development of new rehabilitation approaches is required.
Telehealth modalities have been suggested to aid in the self-management of diabetes, and emerging evidence suggests that telehealth solutions could be effective and feasible in improving clinical outcomes in diabetes care. 15,16 Telehealth solutions are currently used as follows:(1) to monitor the efficiency of the treatment by transmitting blood glucose values to healthcare providers for review and (2) to provide feedback to patients by, for example, phone or videoconference. 17 In the present study, game-based interventions are defined as containing a gaming element that involves virtual reality, serious gaming, or exergaming in combination with a diabetes treatment aspect. Because game-based interventions are entertaining, they are being explored as a potential platform for health promotion 17,18 and offer a motivating aid for adhering to sustained, healthy behavioral changes. 19 Game-based interventions showed a promising effect in the rehabilitation of stroke patients 20,21 and the elderly. 18,22 The core concept of game-based interventions is the use of games to provide rehabilitation interventions to improve patient adherence to PA, or to improve disease-related knowledge, thus leading to a better self-management of blood glucose. Game-based interventions showed a positive effect on mental health (e.g., working memory, depression), physical health (e.g., balance, mobility), and social health (e.g., social interaction, social support) among adult diabetics older than 65 years of age. 9 When played with peers, games can be effective and also motivate participants to increase their PA, for example, in the case of patients with diabetes. 9,23
Game-based interventions could potentially be effective as an educator, motivator, and in maintaining positive health-related behavior in diabetics, but little is known about the effect of game-based interventions in diabetes rehabilitation. The primary objective of this study was to systematically review the literature for the effect of game-based interventions on HbA1c in the rehabilitation of patients with diabetes. In addition, the effect of game-based interventions on self-care, diabetes-related knowledge, and physical outcomes was also reviewed.
Methods
This review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA). 24
Literature Search
We conducted a systematic literature search in MEDLINE, EMBASE, PEDro, Scopus, Cochrane Central Register of Controlled Trials, CINAHL, and PsycINFO. A search matrix was devised with a combination of relevant diagnostic keywords for diabetes and keywords relevant to game-based interventions ( Appendix Table A1 ). The literature search was conducted in October 2014 using the same keywords and synonyms in all databases and only modified for specifically indexed terms related to the databases (subheadings, thesaurus, or medical subject heading [MeSH] terms). To include all relevant studies, we also screened the reference lists of the identified studies for relevant literature.
Study Selection
The study selection was performed based on the study selection process suggested in the Cochrane Handbook. 25 Two reviewers (authors J.C. and R.J.) independently screened for eligible studies by title and abstract. Next, the eligible studies were then compared and disagreements solved by discussion. Study selection was done systematically based on a priori defined inclusion criteria: patients with diabetes (type 1 or T2D), game-based intervention (virtual reality, serious gaming, or exergaming), and randomized controlled trials (RCTs). Studies were excluded if the intervention did not include an interactive game or an application with gaming elements. No language or publication date restrictions were imposed. The two reviewers then independently performed the process again on the eligible articles in full, with the same inclusion criteria for title and abstract, disagreements again resolved by discussion.
Data Collection
The two reviewers extracted data from eligible studies independently. A standardized form based on the checklist provided in the Cochrane Handbook was used for the data extraction. 26 In the selection, risk of bias assessment, and grading process, all data and figures were crosschecked to identify any disagreements. Any disagreements were solved by discussion and a third reviewer (author L.S.V.) was consulted when disagreements persisted. When no between-group analyses were reported, the authors of the present meta-analysis calculated them based on the reported effects and variations in the within-group estimates of effect.
Risk of Bias
The two reviewers independently assessed the methodological quality of the included studies using the Cochrane risk of bias tool 27 for the following: sequence generation (selection bias); allocation sequence concealment (selection bias); blinding of participants and persona (performance bias); blinding of outcome assessment (detection bias); incomplete outcome data (attrition bias); selective outcome reporting (reporting bias); and other potential sources of bias.
Quality of Evidence
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) was used to rate the overall quality of evidence 28,29 based on five factors: design, indirectness, inconsistency, imprecision, and probability of publication bias. Evidence was rated to be of a high, moderate, low, or very low quality.
Results
The database search identified 1,101 articles, 258 of which were duplicates (Fig. 1). Screening for eligibility by title of the 843 unique articles resulted in 64 potentially eligible and after reviewing the abstracts, nine studies were eligible for full-text reading. Five studies were excluded due to no gaming intervention (n = 4) and nondiabetics (n = 1; Fig. 1), resulting in four eligible studies (Table 1). 30 –33 Two studies examined exergames 27,30 and the two others looked at serious gaming using a personal digital assistant (PDA) or a game console. 31,32
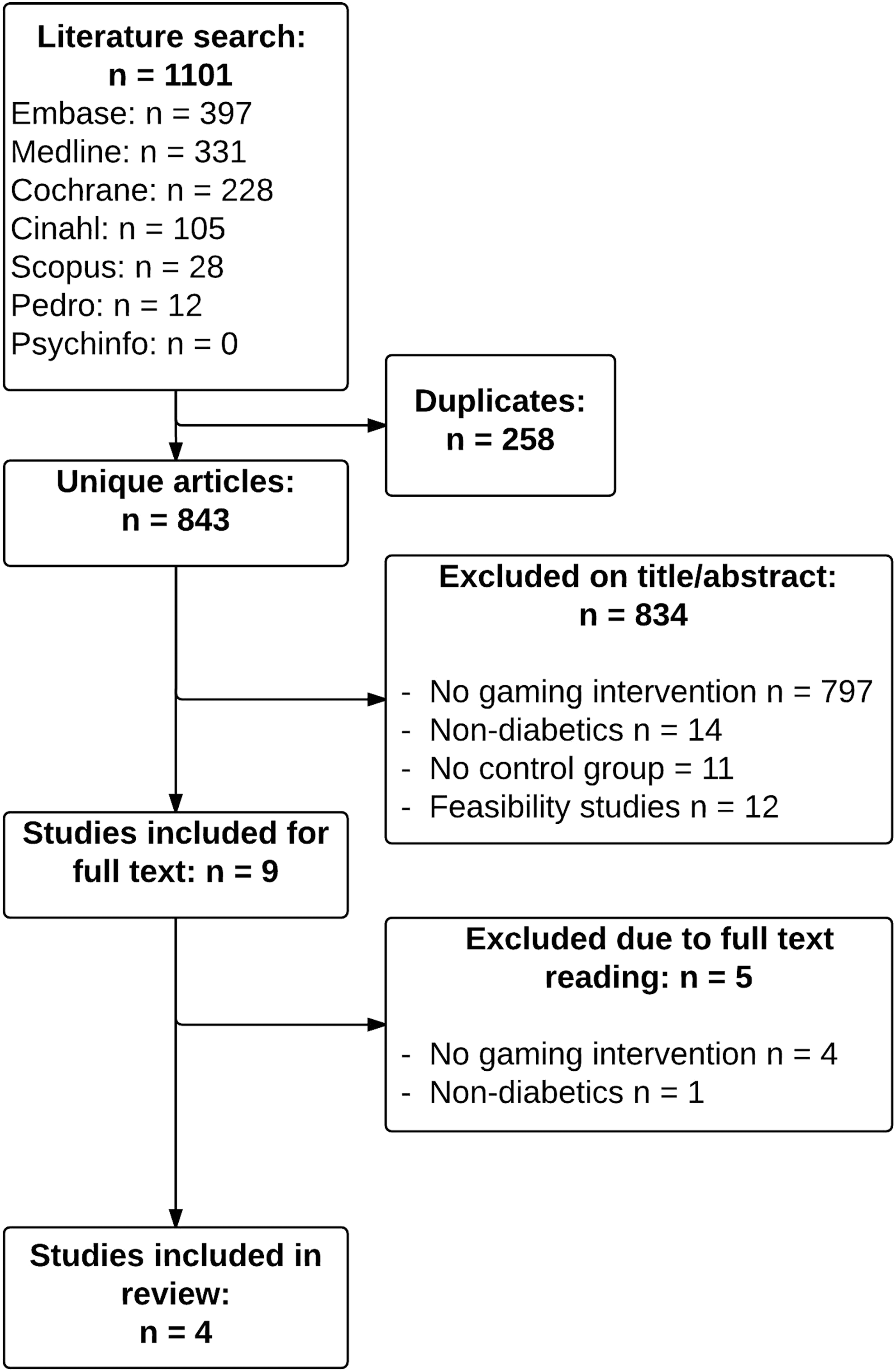
Flowchart showing systematic literature search, screening of studies, full-text reading, and studies included in review with number and reasons of study exclusion at each stage.
Characteristics of Included Studies
BMI, body mass index; DMP, Hemoglobin A1c; HbA1c, Hemoglobin A1c; PDA, personal digital assistant; RCT, randomized controlled trial; T1D, Type 1 Diabetes; T2D, Type 2 Diabetes.
Study Characteristics
Effect of interventions
A random-effects model for the effect of game-based interventions on the primary outcome HbA1c was conducted as the interventions and the sample inclusion criteria varied among the included studies.
Three studies reported HbA1c (Fig. 2). Patients allocated to the game-based intervention had an average standard mean difference (SMD) and 95% confidence interval (CI) = −0.10 [−0.33, 0.14], p = 0.468. Thus, no evidence was found indicating a significant treatment effect between the game-based intervention and the nongaming interventions. The test for heterogeneity: chi-squared = 1.76 (df = 2), I2 = 0.0%, shows that there is, to a great extent, overlap between CI in the included studies and that the observed variance could be spurious. A sensitivity analysis of age (older than/younger than 18 years) showed no effect of game-based interventions in the younger group SMD (CI); 0.10 (−0.30, 0.49) nor in the elderly group SMD (CI); 0.10 (0.33, −0.14). The sensitivity analysis is presented in Figure 3.
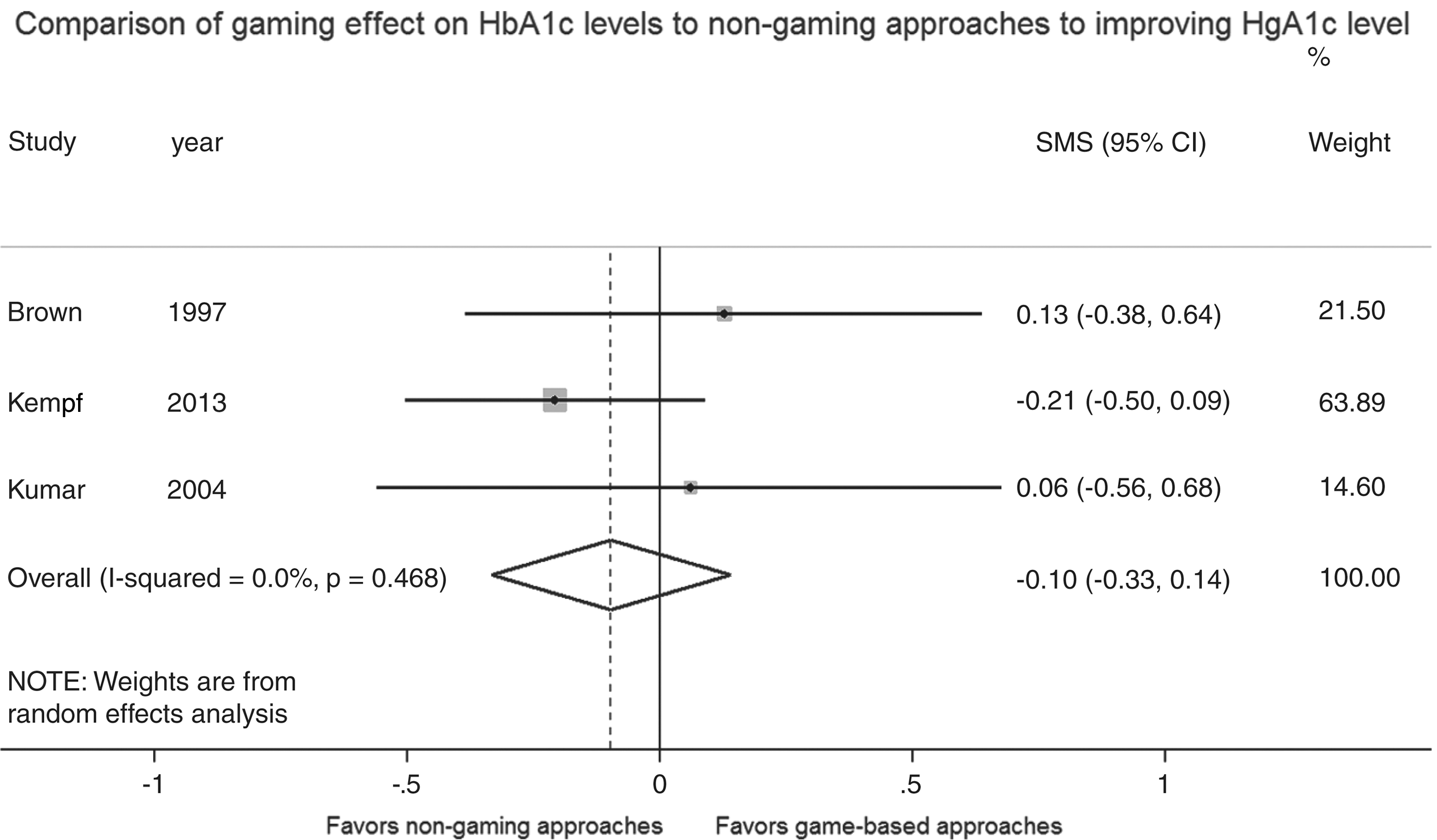
Comparison of gaming effect on HbA1c levels to nongaming approaches to improving HbA1c level.
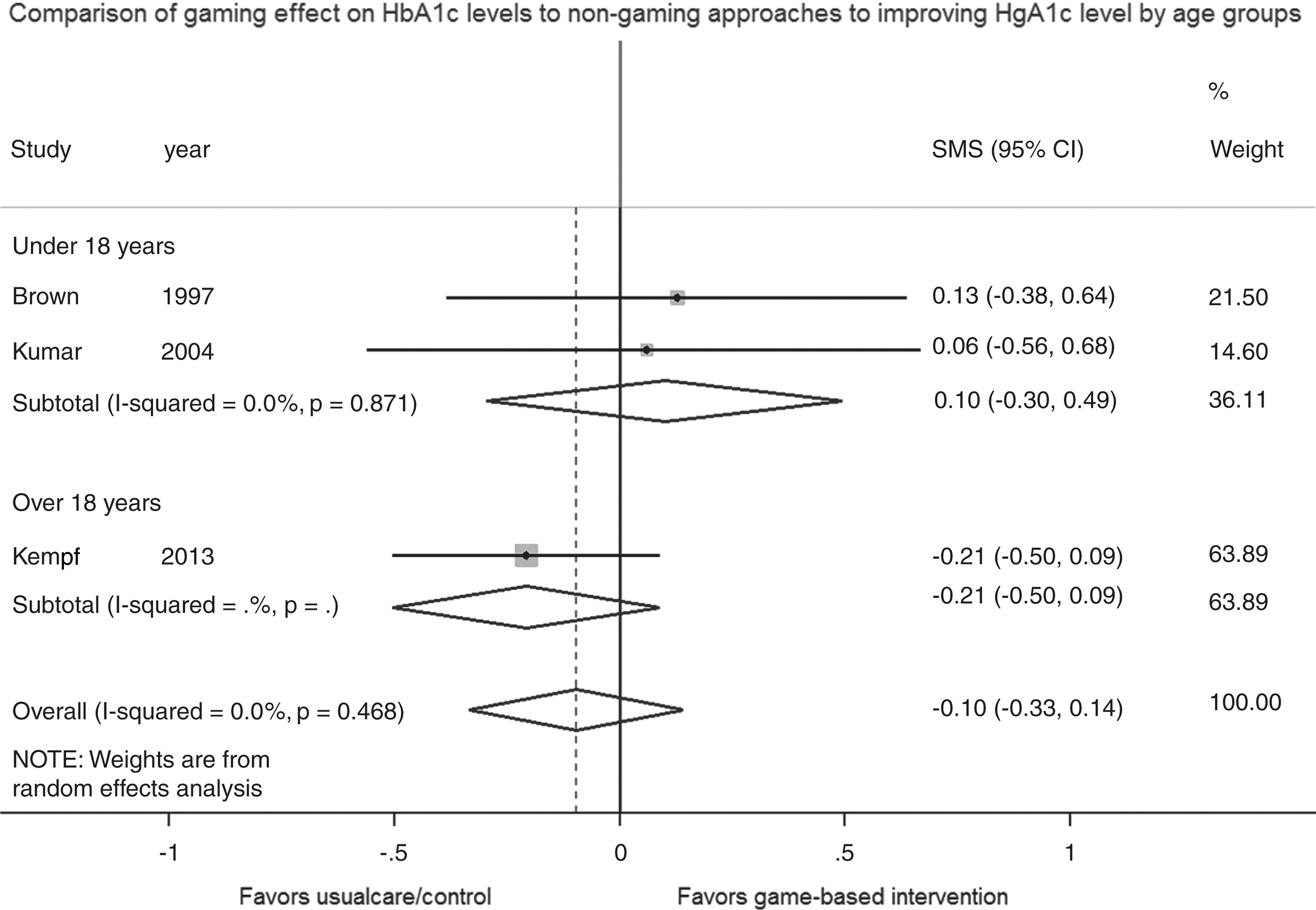
Sensitivity analysis of age on HbA1c levels in game-based approaches and nongaming approaches to improving HbA1c level.
Analysis of Secondary Outcomes
Health-related quality of life
In the study by Kempf and Martin, 33 health-related quality of life, measured by the Allgemeine Depressionsskala, which is the German version of the Center for Epidemiological Studies Depression Scale, increased significantly by 2.4% ± 6.58 (p = 0.03) in the game group compared to the controls who participated after a 12-week period. 33
Diabetes-related knowledge
In the study by Brown et al., 32 patients' diabetes-related knowledge was tested with interviews, and participants were given points based on how many questions they answered correctly. No difference was observed between the game-based intervention group and the control group (p = 0.64).
Balance
Lee and Shin 30 used three balance tests in their study. The one-leg-standing (OLS) test is used to assess postural stability. 34 The Berg Balance Scale (BBS) evaluates the functional balance of 14 activities of daily living and is scored by a healthcare professional. 35 The functional reach test (FRT) measures dynamic balance in a functional reach task. 36 A statistically significant difference in OLS between the game group and the control group was observed. The game group could stand on one leg 4.91 s [4.32–5.50] (p = 0.001) longer than the control group. On BBS, the game group was 1.89 points [0.74–3.03] (p = 0.001) better compared to the control group. On FRT, the game group was 3.68 cm [3.38–3.98] (p = 0.001) better than the control group. In summary, game-based interventions have a significantly positive effect on balance.
Strength
Lee et al. used sit-to-stand (five times) to evaluate lower limb strength. 37 The game-based group improved its lower limb strength and was 2.86 s [2.37–3.35] (p = 0.001) faster compared to the control group. 30
Methodological Quality
The quality of the four included studies was assessed using the Cochrane risk of bias tool. 27 All four studies suffered serious bias in several areas ( Figs. 3 and 4 ). Blinding can be difficult in rehabilitation interventions, but none of the studies made an effort to blind either patients or personnel. All studies showed problems with selective outcome reporting as no protocol was published for any of them, and the studies by Kempf and Martin 33 and Lee and Shin 30 reported no between-group analysis (calculated by the authors of the present meta-analysis). In three of the included studies, the allocation concealment was unclear ( Figs. 4 and 5 ).
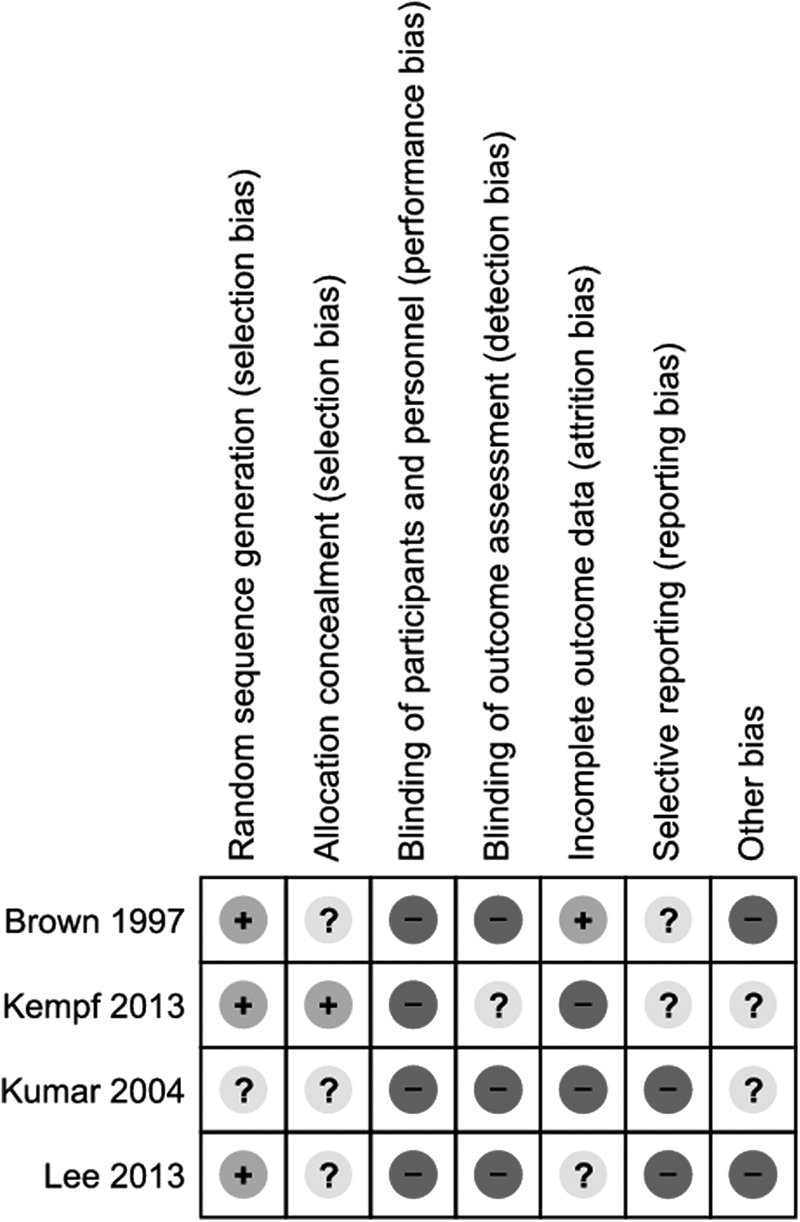
Risk of bias summary: review authors' judgments about each risk of bias item for each included study. +, Low risk of bias; -, High risk of bias; ?, Unknown risk of bias.
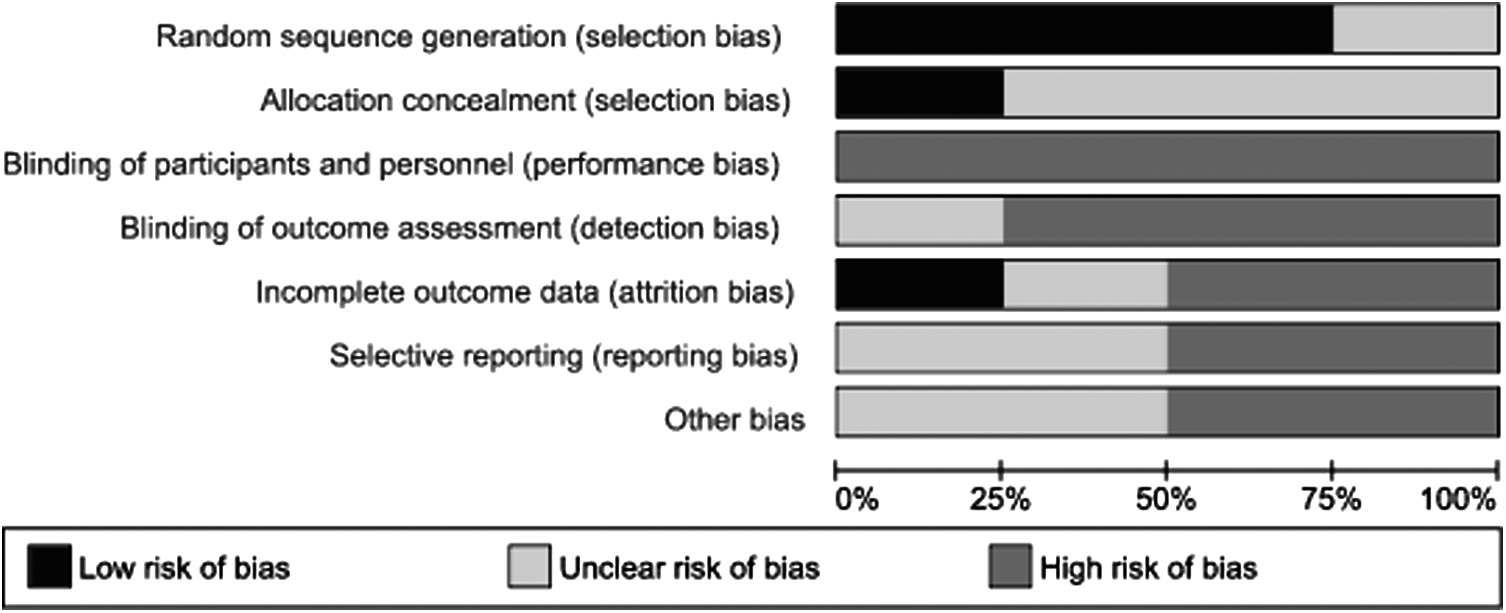
Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.
Grade
The quality of the body of evidence was evaluated using GRADE, 29 while HbA1c was used as the primary outcome in three studies and was the only outcome used in more than one of the studies included.
The quality of evidence was downgraded due to serious risk of bias and the degree of indirectness, but also because the interventions were not consistent and the magnitude of effect showed impression. Furthermore, the literature search identified conference articles not published in journals, which may be an indication of publication bias. The quality of evidence was thus graded very low. Table 2 presents a summary of grading for quality of evidence in HbA1c.
Grade Evidence Profile-Summary of Grading for Quality of Evidence in HbA1c
Discussion
Summary of Evidence
Four studies were found eligible for this systematic review and meta-analysis investigating the effect of game-based interventions on HbA1c and clinical outcomes. Game-based interventions showed no effect on HbA1c when compared to usual care or waiting lists, however, this is result is based on a limited body of evidence. Three studies 31 –33 with different game-based interventions (predict the upcoming HbA1c on a PDA 31 ; Super Nintendo® containing diabetes-related content 32 ; exergame with Wii Fit Plus 33 ) were included in the analysis, which is why indirectness among the studies exists. Inconsistency between study results was observed. The results of the present review differ from results in previous reviews on game-based interventions, for example, virtual reality, serious gaming, and exergaming. 38,39 One possible explanation for this is that only RCTs were eligible for inclusion in our review. Another potential explanation is that the studies focused on HbA1c as the main outcome and not on self-management or knowledge-related outcomes. The present review shows that there was serious risk of bias in the included studies, thus resulting in a very low GRADE rating for the quality of the body of evidence. The very low GRADE rating reflects that the likelihood that the effect will be substantially different (i.e., large enough difference to possibly affect decision-making) is high, however, this result is based on a limited body of evidence. 29
Secondary Clinical Outcomes
The present review examined health-related quality of life, diabetes-related knowledge, muscle strength, and balance as secondary clinical outcomes. Game-based interventions were superior to controls in improving health-related quality of life, muscle strength, and balance. 30 No difference was found between game-based interventions and controls in terms of diabetes-related knowledge. 32 Due to the low number of included studies, it was not possible to perform a meta-analysis examining the effect or to do a GRADE rating of the quality of the body of evidence for secondary outcomes.
Previous studies on telemedicine in the care of patients with diabetes contain more positive conclusions compared to the present review. A systematic review by Marcolino et al. 40 explored the effect of telehealth solutions on HbA1c and found a significant absolute reduction of 44% [61–26%] when compared to usual care. This result is in contrast to the present review. Marcolino et al. 40 included only studies investigating patients older than 18 years of age and the intervention could be any telehealth approach that included personal feedback from a healthcare practitioner. Since our review only investigated game-based interventions and not the wider telehealth approach, different studies are included in the two reviews. Therefore, telehealth approaches in general can show a significant effect, as stated by Marcolino et al., 40 and the effect of game-based interventions does not seem to show the same effect as our results indicate.
Limitations
The included studies in this review had some limitations. For example, two of the three studies on HbA1c had no follow-up period, and one study only had a trail period of 4 weeks. Given the response times for HbA1c, this time frame may be insufficient. The gaming content inclusion criteria limited the amount of studies eligible for inclusion in the present systematic review. However, a broader definition such as telehealth would have resulted in more eligible studies, but at the same time this would have introduced indirectness of the findings in terms of the game-based aim of the present study. Because this field of research is still relatively new, many synonymies exist for games used for health purposes. The search strategy we chose was designed to include a wide variety of game types, but there was still the risk that research categorized under different keywords would remain unidentified.
The content of the games was as different as the platforms they were designed for, which was also the case for the outcomes they chose to measure. An important difference between exergames and serious games is the method used to improve the health of patients with diabetes. While the gaming element in the exergame and the virtual reality game directly influence players by making them move around, serious games take a different approach. By combining gameplay with education, essentially a “gamification” of traditional educational content relevant to diabetics, these types of games try to make learning fun. Both Packy & Marlon 32 and DiaBetNet 31 educate players on diet, basic knowledge about diabetes, and blood sugar monitoring, in addition to testing this knowledge as part of the game.
As mentioned, game-based interventions have been shown to have an effect on both stroke patients 20,21 and the elderly, 18,22 but only patients with diabetes were included in the present systematic review, which is why our results are solely based on findings for this population.
Conclusions
Game-based interventions showed no effect on HbA1c in patients with diabetes when compared to usual care/waiting lists, but they did show a significant effect on health-related quality of life, balance, and strength. However, these conclusions are based on a limited body of evidence and should be interpreted with care. No difference was found between game-based interventions and controls in terms of diabetes-related knowledge. The overall methodological quality of the included studies is low and the body of evidence graded very low. As the population with diabetes and rehabilitation expenditures grows, the authors see the potential of game-based rehabilitation for chronic diseases, such as diabetes, because of its motivating nature. Additional and better methodological studies are needed, however, to gain knowledge about the full potential of game-based rehabilitation.
Footnotes
Acknowledgment
The authors thank Rikke Daugaard for her contributions to the search matrix used in the present review. This project did not receive any specifically earmarked grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure Statement
No competing financial interests exist.
Appendix
Search Matrix
| FOCUS 1 | AND | FOCUS 2 |
|---|---|---|
| diabetes mellitus | game | |
| diabetes | games | |
| dm2 | gaming | |
| dm1 | exergame | |
| niddm | exergames | |
| noninsulin dependent | exergaming | |
| noninsulin dependent | virtual reality | |
| iddm | active video | |
| T2D | game-based | |
| type 2 diabet* | teleplay | |
| type ii diabet* | digital play | |
| T1D | serious gaming | |
| type 1 diabet* | ||
| type i diabet* | ||
| adult onset diabet* | ||
| late onset diabet* | ||
| “diabetes mellitus”[MeSH Terms] | ||
| “diabetes mellitus, type 2”[MeSH Terms] | ||
| “diabetes mellitus, type 1”[MeSH Terms] |
The search was conducted based on this matrix and additional indexed terms (e.g., subheadings, thesaurus, or MeSH terms). Here is the specific search matrix for MEDLINE presented. MeSH, medical subject heading.