
Abstract
Introduction
Echography is one of the most frequent forms of medical imaging requested by medical doctors after initial clinical examinations. However, even in developed countries with highly sophisticated healthcare systems, there are still wide areas where patients are required to travel more than 50 km for an ultrasound examination. Even in small cities (<10,000 people) where there are medical centers with various healthcare professionals, trained sonographers are not always present, requiring patients to travel to centers in a larger city for diagnostic examinations.
In most remote locations, medical professionals (paramedics, general practitioners) have no experience with clinical ultrasounds. In the minority of locations where professionals are minimally trained in the use of clinical ultrasound, they may possess the ability to visualize organs of interest but are generally unable to obtain the correct view for diagnosis without assistance from an expert sonographer. In addition, the reliability of the diagnosis from an echography examination is highly dependent on the level of training of the operator. Therefore, in small-city medical centers without access to trained sonographers, the need exists for a teleoperated echography system to facilitate examinations.
Tele-echography has been used for primary patient diagnoses in trauma or emergency situations 1 –3 in isolated areas such as Antarctica, 4 and in isolated rural areas. 5 Several different methods of tele-echography have been investigated using different technologies such as audio–video transmission, 6 three-dimensional (3D) echography, 7,8 and teleoperated echographic probes 9 with various degrees of success and ease of use. Regardless, the results from all of these studies confirmed the positive impact of remote echography on patient management and health outcome. 10
In 2002, a first-generation robotic arm to which an ultrasound probe could be attached for teleoperation through an Internet connection was developed by our group. 11 The system was validated in two isolated medical centers with remote abdominal, pelvic, and fetal examinations being performed successfully in 85% of the more than 110 cases. 12,13 The latest version of the robotic arm had dimensions of 40 × 40 × 35 cm and weighed approximately 3.5 kg. 14 Thus a mechanical support was necessary as the operator could not easily move the robotic arm or keep it stationary on the patient. 14 Even using the mechanical support, the nonsonographer operator was still required to locate the probe over the appropriate acoustic window with a degree of accuracy. However, this was difficult due to the size and weight of the robot and support structure, which emphasized the need for a smaller, more maneuverable teleoperated echography system.
The objective of the current project was to develop and validate in real clinical settings a smaller, more manageable teleoperated echograph and probe system. The system would involve modifying a commercially available echograph to allow the teleoperation of the functions and settings. Also, specialized motorized probes would be developed that contain internal motors to change the orientation of the ultrasound transducer. In addition to being more manageable in clinical settings, the smaller teleoperated probe unit would be more appropriate for use in medical centers and also in other settings where there are environmental restrictions such as areas devastated after natural disasters, in hazardous environments, or on the International Space Station.
Materials and Methods
Teleoperated Echograph and Probe Unit
A commercially available echograph (Orcheo Lite; Sonoscanner, Paris, France) was modified to allow for teleoperation through an Internet connection (TeamViewer GmbH, Göppingen, Germany) (Figs. 1 and 2). At the expert site, the trained sonographer adjusted the settings (gain, depth, etc.) and functions (Doppler, color, 3D, etc.) of the echograph using a standard keyboard (Fig. 3B). Each setting or function of the echograph was identified by letters on the keyboard; for example, Figures 6 and 7 increased and decreased gain, respectively, whereas Figure 4 activated the pulsed-wave Doppler mode. The design and weight (6 kg) of the echograph were not altered; however, additional functions were added to the operation, including elastography, 3D reconstruction, and radiofrequency display and process.
Images of the

Image of the teleoperated equipment at the patient site including
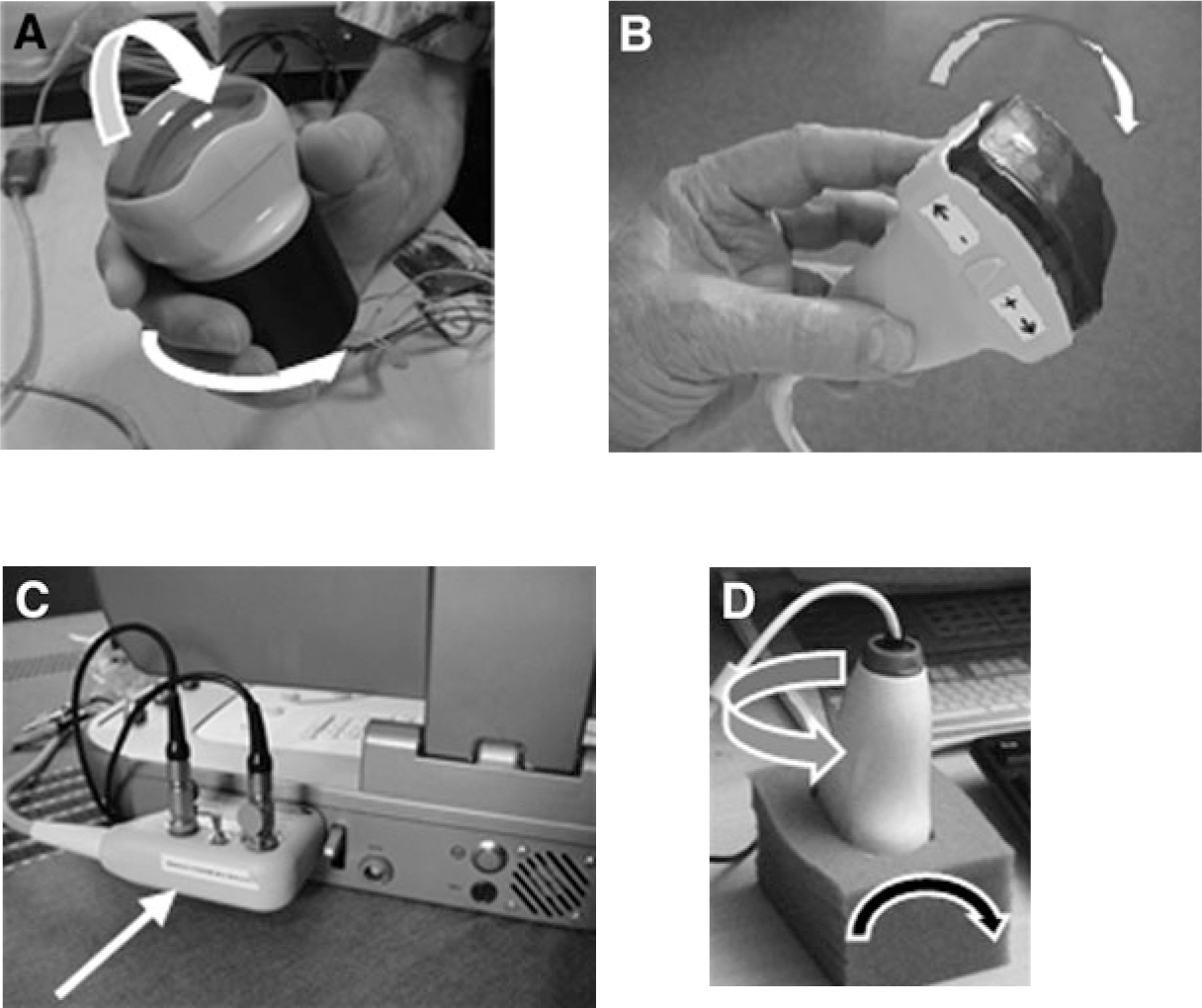
Two specialized teleoperated probes were developed (Vermon, Tours, France) for this system that were similar to commercial 3D probes, but slightly larger and heavier (400 cm3 and 430 g). The first motorized probe contained a convex array transducer (3.5–7 MHz) providing a wide image used for the assessment of deep organs (Fig. 1A). This probe was teleoperated using one motor to tilt the transducer (+55° to −55°) and a second to rotate the transducer around the central axis (±180°). The second probe contained a linear array transducer (5–15 MHz) used for the assessment of superficial organs (Fig. 1B). In contrast to the convex probe, the linear transducer was only teleoperated using one motor for the tilt movement (+55° to −55°) as it was believed that the nonsonographer operator would be able to identify the long and short axes of the superficial organs of interest (blood vessels, muscles). The probes were connected to the echograph using the standard probe connector, and the motors were connected to an electronic module (engine pilot) external to the echograph and connected to the Internet for teleoperation (Fig. 1C). Using custom software (Optimalog, St. Cyr-sur-Loire, France), movements of a dummy probe (Fig. 1D) located at the expert site were mimicked by the transducer of the motorized probe at the patient site.
At the patient site, a portable basic computer was used to connect the motorized probes to the Internet (Fig. 2) and display the control panel for the motorized probe engines and the ambient video and sound from the expert center. An Internet protocol (IP) camera (AXIS, Paris) allowed the expert sonographer to communicate with the nonsonographer operator at the patient site. A switch was used to control simultaneously the Internet connection for the portable computer, the echograph, and the IP camera.
At the expert site (Fig. 3A), a basic portable computer, connected to the Internet, was used to teleoperate the echograph and motorized probe and for the videoconference (IP camera; AXIS) between the two sites. The dummy probe was connected to this computer via a USB plug. A summary schematic of the teleoperated system is presented in Figure 4.

Images of the equipment used by the expert sonographer including

Schematic summarizing the teleoperated system. Solid black arrows show the transfer of information from the expert site to the patient site to control the motorized probe transducers (Optimalog) and the echograph (TeamViewer). Dashed arrows show the return of the ultrasound video back to the expert site (TeamViewer). Dotted arrows show the connection for the videoconference between the two sites (TeamViewer), which was accomplished using the personal computers (PCs) at both sites and Internet protocol (IP) cameras.
Tele-Echography Procedure
The teleoperated system was used for the examination of 100 patients from two medical centers, Richelieu and Ligueil, located 50 km and 60 km, respectively, away from the University Hospital in Tours and linked by ground Internet. After the initial clinical examination, the physician at the isolated medical center contacted the University Hospital to schedule the ultrasound examination within the following 24 h. In some cases the examination was scheduled within 30 min of the physician contacting the University Hospital. Patients were recruited in the order that they arrived at the medical centers. Each patient was informed of the procedures and signed a consent form with the physician at the medical center. At the expert center, patients were identified solely by number to maintain patient confidentiality. Patient names were only introduced by the attending physician into the anonymous medical reports received from the expert center. All protocols and procedures were approved by the University Hospital Ethics Committee (Tours).
To perform the teleoperated echography, the nonsonographer operator (physician or paramedic) at the patient site was required to hold and maintain the motorized probe motionless on the patient in the location indicated by the expert sonographer through the videoconference connection (Fig. 5). The expert sonographer then optimized the ultrasound image by teleoperating the echograph and the motorized probe transducer. Once the appropriate view was obtained (frozen image or cineloop reviewed by the expert), video and images were saved on the computer at the expert site for inclusion in the final medical report. Video and image were also saved on the patient echograph for later review and reprocessing (measures) by the expert if need. The diagnosis was delivered to the physician verbally over videoconference during the teleoperated examination with a follow-up report, identified only by patient number, being sent via e-mail within 30 min after the examination.

Image of the patient at one of the isolated sites with the motorized probe being held motionless by the nonsonographer operator.
Additional long distance validation tests to determine the ease of use of the system were conducted with the teleoperated echograph and motorized probed unit being temporarily located in the Hospital of Ceuta (southern limit of Europe, in Spain, by ground Internet) and at the Apatou dispensary in the Amazonian rain forest (French Guiana, by satellite Internet) located 1,800 km and 7,000 km, respectively, away from the University Hospital in Tours. In both of these locations similar teleoperated echography procedures were followed, but with only a limited number of cases (10 pregnancies and 5 cases, respectively). The physicians in each of the medical centers had previously used the robotic arm for teleoperated echography; therefore they were asked also to evaluate the ergonomics and performance of the teleoperated echograph and motorized probes compared with the robotic arm.
At the University Hospital in Tours, two experts who were using tele-echography in practice were asked to evaluate the time response of the motorized probe to the expert's hand movements, the quality of the image reaching the expert center, and the use of the keyboard for adjusting echograph settings and functions. The performance of the new system was compared with that of the previous robotic arm system already medically validated. 12 –14
Results
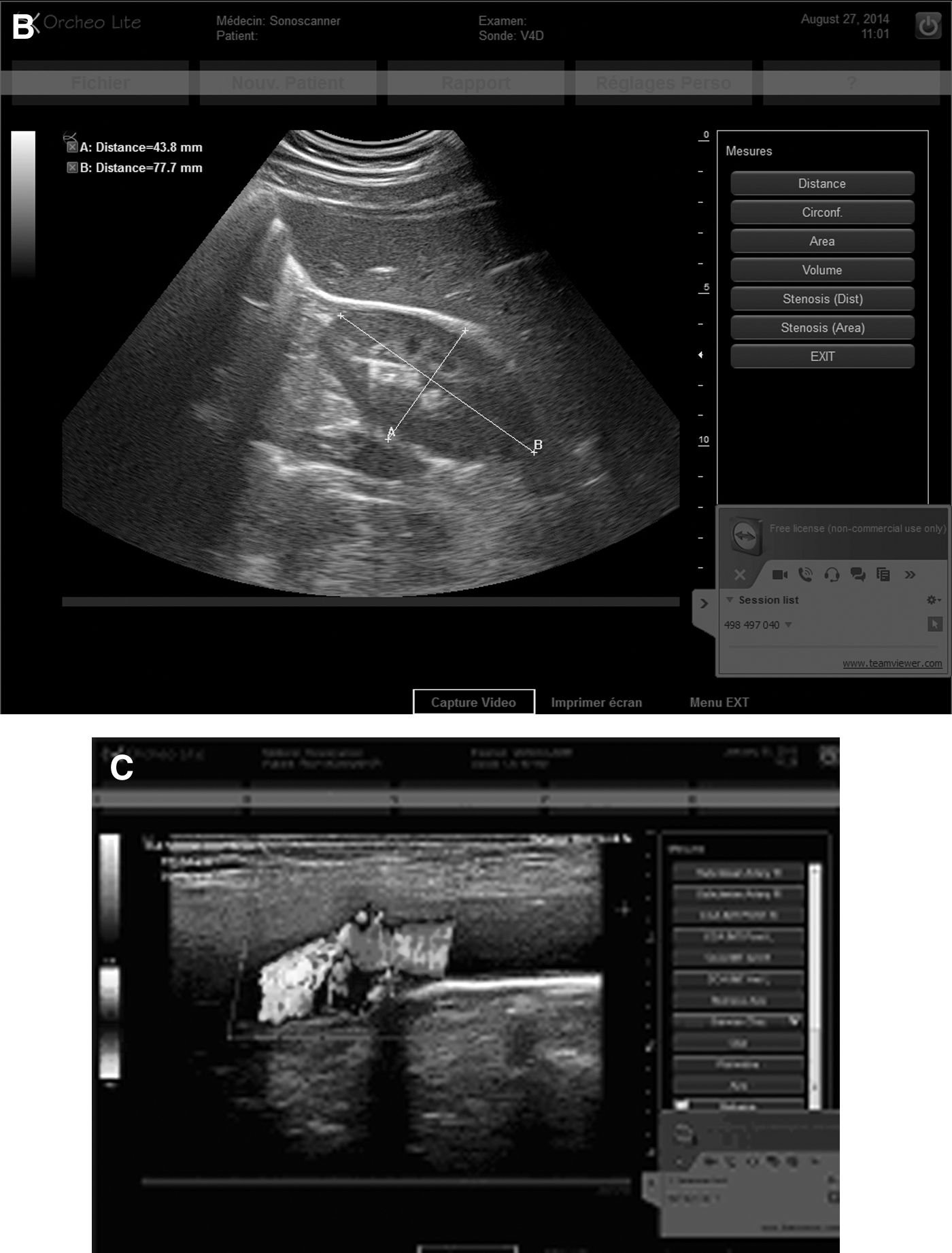
Over a 5-month period, 100 teleoperated ultrasound examinations were conducted in the two small medical centers 50–60 km away from the Tours University Hospital, on the abdomen and pelvis (36%), vascular structures (42%), and other small parts including the thyroid and various skin muscles disease (22%). All examinations were standardized to include imaging and measurements of similar organs and structures. The abdominal examination included B-mode visualization of the pancreas, liver, biliary tract, gallbladder, and the right and left kidneys (Fig. 6A and B). Pelvic examinations involved the visualization of the bladder, uterus and ovaries, or prostate. Vascular imaging included assessments of the carotid arteries or the veins of the lower limbs. The common carotid artery was imaged in B-mode for the measurement of the intima-media thickness, and the bifurcation was imaged in B-mode, color, and pulsed-wave Doppler modes for the calculations of the resistance index and the quantification of stenosis (Fig. 6C). The veins of the lower leg (femoral, popliteal, posterior tibial, and gastrocnemius veins) were imaged in B-mode and color Doppler with compression being applied to the leg distal from the Doppler recording point. Thyroid investigations included transverse and longitudinal views in B-mode, color, pulsed-wave Doppler modes, elastography, and muscle examinations included the visualization of the muscle and vascular structures with both B-mode and color.

Example ultrasound images collected during the teleoperated examination:
Organs were adequately visualized, the color and pulsed-wave Doppler modes were correctly displayed, and the diagnosis was given for 97% of the examinations. In 2 obese patients the pancreas and gallbladder could not be visualized due to poor echogenicity. In an additional patient, edema and fat tissue prevented the proper imaging of the leg deep veins. In each of these cases the patient underwent a conventional echography examination at a radiology center.
Setup of the connections for teleoperation and the videoconference required less than 3 min. Each examination took an average of 17 ± 4 min to complete. Using the Internet connection for teleoperation (1 megabits/s [Mbps]; 10 frames/s [fps]), there was about a 2-s lag for commands to be transmitted to the echograph and motorized probe and for the resulting modifications in the ultrasound video to be transmitted back to the expert site. The sonographer was able to accommodate for this lag after about 1 h of training with the system. Additionally, the quality of the ultrasound image at the expert site was slightly lower than that on the actual echograph at the patient site; however, the images were still of good quality for medical diagnoses. On two occasions the teleoperated examination could not be performed due to a weak Internet connection greatly degrading the quality of the transmitted video. Therefore these exams were rescheduled for the following day without issue.
The teleoperated examinations performed with 15 pregnant patients in long distance sites (the hospital in Ceuta, n = 10; the hospital in French Guyana, n = 5) reported similar quality of ultrasound images allowing for medical diagnoses. There was no difference in the teleoperation lag with the hospital in Ceuta using ground Internet, but the delay was increased to 3 s for examinations conducted in French Guyana (7,000 km from the expert sonographer) using satellite Internet. Limited testing was also conducted with the expert sonographer located away from the Tours University Hospital (20 out of the 100 cases) using home, mobile phone, airport, or hotel Internet connections with no detriments to the teleoperation of the echograph and probe system nor on the image quality.
Discussion
The current study successfully demonstrated the clinical use of the teleoperated integrated echograph and probe system for performing clinical ultrasound examinations in areas isolated from trained sonographers. This system improved on previously used methods of remote ultrasound examinations to provide a system that is smaller and easier to use for the nonsonographer operator, does not require substantial training of the nonsonographer operator, allows for the teleoperation of the echograph by the expert sonographer, and uses a standard Internet connection. The results of this study demonstrate that this teleoperated echograph and probe system may be used in clinical settings where a trained sonographer is not readily available.
Other Systems for Tele-Echography
Previous versions of teleoperated ultrasound examinations have been used in different settings with each presenting several limitations. For the simplest version, remote guidance consists of a trained sonographer directing a partially trained operator at the side of the patient through the ultrasound examination using a videoconference link. Using this system, only a videoconference link was required for communication between the sonographer and the patient site operator; however, this system also required minimal training of the patient-site operator to become proficient in visualizing the organs of interest for the examination. 15 –17 Therefore, remote guidance is only effective if the operator in the isolated site has received training in ultrasound imaging. Moreover, this system has not been validated in routine practice on real patients.
To avoid the need for training operators in the isolated medical sites, a volume capture method was developed and tested in clinical settings and on the International Space Station. 7 –9 Using this method, the operator located the probe over the organ of interest and then tilted the probe to scan the area containing the organ. The video from this tilt maneuver was used to reconstruct a virtual 3D image that a trained sonographer then used to find the appropriate view of the organ and to perform the required measurements. This method was found to be useful for visualizing morphological issues but does not allow for Doppler or time–motion assessments. In addition, this is a postprocessing method requiring substantial time after the initial investigation to generate a report and to deliver a diagnosis.
A robotic arm to which a standard ultrasound probe could be attached was the first generation of teleoperated ultrasound developed by our research group that was capable of real-time echographic and Doppler examinations. 11 –13 Using the robotic arm did not require the patient-site operator to have any training in ultrasound imaging, but this operator was still required to operate the settings and functions on the echograph under the guidance of the expert sonographer through videoconferencing. This system has been successfully used for examinations of several hundred patients over the past 10 years with successful diagnoses in 85% of cases. 11 –13 Currently, the most recent version of this system is still in routine clinical use and delivering successful diagnoses in 97% of cases. 14 Due to the volume (40 × 40 × 35 cm) and weight (3.5 kg) of the robotic arm, a heavy mechanical support structure was required. The nonsonographer operator was required to move the support structure into position so that the ultrasound probe was correctly located over the appropriate acoustic window, which was not easy or accurate with this support structure. Therefore, the present teleoperated integrated echograph and probe unit, called “Tele-Operated UltRasound System” (“TOURS”), aimed to address the size and weight issue of the robotic arm and to reduce the responsibilities of the nonsonographer operator by allowing for the teleoperation of the echograph settings and functions.
Ergonomics of the Current System
The motorized probes designed for the teleoperated ultrasound system were similar in size and weight to commercially available 3D ultrasound probes. The small size and light weight of both the deep organ and superficial organ probes made it easy for the nonsonographer operator to correctly position the probe on the patient and to hold it still throughout the ultrasound examination. Each probe contained motors that allowed the expert sonographer to remotely change the orientation of the transducer to optimize the image for diagnoses without requiring the assistance of the nonsonographer operator. In addition to the probe being easy to place and hold, its small size also made it possible to locate the probe on the lateral side of the patient for visualization of the kidney or to push hard on the probe (increase hold down pressure) if requested by the expert for patients who were obese or unable to hold a breath. These motions were not possible with the robotic arm attached to a mechanical cart.
The echograph connection ends of the motorized probes were modified to allow electrical input for teleoperation. As the modifications were made on the probe connectors (Fig. 1), the motorized probes could be operated either in teleoperation mode or as a standard echograph probe. In addition to using the dummy probe to teleoperate the motorized probes, the expert sonographer could activate a program in which the motorized probe performed a 90° tilt scan (2–4 s) for a video volume capture of the area under the probe. This video could then be processed to produce a 3D reconstruction of the volume scanned for later analysis at the expert center. In the case of poor Internet transfer rates, this tilt movement could be initiated by the nonsonographer operator at the patient site and the saved video later transferred to the expert site for analysis. 9
Remote Control of the Echograph Settings and Functions
The second major issue that was addressed by this teleoperated echograph and probe unit was the ability of the expert sonographer to directly control the echograph settings and functions. Software was designed that allowed the expert sonographer to control the echograph using a standard keyboard without requiring actions from the nonsonographer operator at the patient site. In addition to controlling the settings such as gain and depth, the expert was able to freeze the image or Doppler trace and to access the cine loop to determine the best available image and to save frozen images and video clips to the echograph and the computer at the expert site. Lastly, the expert was able to recall saved images and videos directly from the patient-site echograph for additional measurements after the patient had left. The ability of the expert to control all of the echograph functions and settings greatly reduced the time required to perform the teleoperated ultrasound examination as changes and measures could be made without having to verbally direct the nonsonographer operator to make the required adjustments. This also helped to reduce the required training of the nonsonographer operator, who was then only required to properly locate the ultrasound probe over the desired acoustic window, which was achieved using visible landmarks (for example, xiphoid, costal border, mammary line) and direction via videoconference with the expert sonographer.
Tele-Echography in Practice
Teleoperation of the echograph and probe unit involved a lag time of approximately 2 s for the majority of locations tested with ground Internet. The expert sonographer was required to accommodate for this delay when moving the dummy probe and changing the echograph settings and functions. The expert was therefore required to move the dummy probe much slower to avoid overshooting the organ of interest or scanning through the organ too quickly. It was found that expert sonographers were able to adjust to this delay after only 1 h of training with the teleoperated system.
The equipment used by the expert sonographer also presented the advantage of being portable. The system consisted of a portable computer and the dummy probe, which was approximately 200 cm3 in volume, weighted 150 g, and connected to the computer via a USB connection. Therefore, the equipment for the expert sonographer (approximately 1 kg in weight) could be transported to different locations and used for the ultrasound examinations in any location where an Internet connection was available (medical center, home, hotel, etc.). This is a definite advantage in emergency situations as the expert sonographer would not be required to travel to specialized locations, thus decreasing the time required for ultrasound diagnoses.
Previous work has demonstrated medical interest in the use of teleoperated systems for examinations in isolated areas. 14 Typically, a patient in an isolated medical center would be required to travel to a center in a larger city for the examination and wait 3–7 days before getting an appointment at a radiology center and receiving the echographic report. With the teleoperated system, physicians and patients are able to get diagnoses faster, leading in many cases to earlier treatment and improved patient outcomes.
Limitations
The lag present in the teleoperated echograph system resulted in longer durations of the ultrasound examinations. When the expert made an adjustment to the dummy probe, the resulting image did not appear on the screen for 1–2 s. Consequently, the expert was required to make only single movements of the dummy probe at slow speeds. This is in contrast to conventional examinations, where the sonographer is able to rapidly move the probe over the patient's skin. The expert sonographers were able to adjust to this delay with approximately 1 h of training, but this still resulted in longer echography examinations.
Using TeamViewer made it easy to connect the teleoperated echograph to the expert center as it does not require a fixed IP address and can pass through several standard firewalls. Unfortunately, the bandwidth and the frame rate of the transmitted video fluctuate, likely in relation to the number of customers using the Internet service at the same time. Thus, the quality of the video reaching the expert was not constant. If the quality of the image was made a priority, then the delay increased from 2 s. Therefore, in some cases (not frequent) priority was set to reduce the lag initially while the sonographer found the appropriate view and then to image quality to obtain good-quality images for analysis. This also served to further increase the time required for the ultrasound examination. The current expert medical center has access to an Internet bandwidth of 1 Mbps, which was able to transmit good-quality images at a frame rate of 10 fps. In the past, a bandwidth of 512 kilobits/s was used, and the image quality was significantly reduced while still sufficient to evaluate the status of the organs if a frame rate above 8 fps was maintained. If the frame rate dropped below 8 fps the video was not transmitted correctly (image interruption, image missing, background noise, and pixels on the image), preventing the delivery of a medical diagnosis. In the current study the Internet flow rate during the tele-echography examinations was not directly measured; however, it was subjectively determined that a 1 Mbps bandwidth and a frame rate of 10 fps would consistently result in transmitted images of sufficient quality for accurate diagnoses.
The motorized probes designed for this system present a great improvement over the robotic arm and support structure. However, the motorized transducers in the probes only allow for the orientation to be adjusted in two directions. Thus, the degree of maneuverability of the motorized probe is restricted compared with a human hand. In some cases it was difficult to obtain the appropriate view for diagnoses with this restricted movement, resulting in longer examination time.
Conclusions
The current teleoperated echograph and probe system allowed for ultrasound examinations to be performed quickly (15–20 min), successfully (in 97% of the cases), and without the need of a trained operator at the patient site. This system serves to reduce the time required for patients to receive medical diagnoses, potentially resulting in faster initiation of treatment and improved patient outcomes. The teleoperated echograph and probe unit in the current study, “TOURS,” is a substantial improvement on the previous version requiring the use of a large, heavy robotic arm and support structure. The echograph and probe system are light (echograph, 6 kg; electrical module and computer, 1.3 kg), and the motorized probes (430 g and 300 g) do not require a large support structure, making it ideal for locations with environmental constraints (geographically isolated sites, centers with limited medical equipment, long distance airplanes, hazardous areas, spaceflight, etc.). Currently this system is scheduled to fly onboard the International Space Station at the end of 2016 under the project name TOURS (Tele-Operated UltRasound in Space).
Footnotes
Acknowledgments
The authors thank Mme. Maryannick Porcher for her active contribution to the tele-echography examinations. The present work was supported by CNES (the French Space Agency) (R & T grant TOURS-2:131512-2014).
Disclosure Statement
No competing financial interests exist.