
Abstract
Introduction
Chronic medical conditions affect over 140 million Americans, account for 85% of healthcare expenditures, 1 and are now the leading causes of disability and death globally. 2,3 Access to care for individuals affected by chronic conditions is limited by distance, disability, the distribution of doctors, and other socioeconomic factors. Telemedicine has the potential to reach these individuals directly in their homes. Virtual house calls using simple, secure videoconferencing could represent the next-generation house call.
Although many studies have evaluated telemedicine for chronic conditions, few have examined videoconferencing, and even fewer have examined videoconferencing into the home. A 2012 review by Wootton 4 found 141 randomized controlled trials of telemedicine interventions for chronic conditions. However, most studies evaluated remote, generally asynchronous (e.g., text messages) monitoring or telephone support. Ten evaluated videoconferencing, but most were conducted in clinics. A subsequent literature search 5 found only six randomized controlled studies evaluating video visits directly into the home. With the exception of one multicenter spinal cord injury study, 6 most studies have been single center, short, and small. Despite this limited evidence base, interest in virtual house calls is rising rapidly for many conditions. 7 –10
Parkinson's disease is a prototypical chronic condition. Its incidence increases with age, 11 and its burden will double over the next generation. 12 Individuals have Parkinson's disease for approximately 14–16 years after diagnosis, 13,14 and it leads to progressive disability, cognitive impairment, limited mobility, 15 and impaired driving ability. 16 Parkinson's disease also burdens caregivers, 17 frequently requires institutional care, 18 –20 generates high healthcare costs, 21,22 and benefits from specialty care. 23 –26 However, over 40% of Medicare beneficiaries with Parkinson's disease do not receive care from a neurologist within the first 4 years after diagnosis, 26 and those who do not have worse health outcomes, including a 22% increased risk of death within 6 years. 26
Because many motor features (e.g., tremor, bradykinesia, gait changes) are assessed visually 27 and many nonmotor aspects (e.g., depression) are assessed by history, Parkinson's disease is well suited to remote assessment. Initial telemedicine applications began over 20 years ago 28 and have increased since then. 29 A 6-month randomized pilot study of 20 individuals demonstrated that video visits into the home were feasible, could produce comparable outcomes to traditional in-person care, and saved patients and their caregivers 3 hours of time and 100 miles of travel per visit. 24 However, national, large-scale studies of virtual house calls are lacking for Parkinson's disease and other chronic conditions. To that end, we are conducting such a multicenter study and here report baseline data, as well as interest, feasibility, and barriers to enrollment.
Materials and Methods
Trial Design
We are conducting a 12-month, multicenter national randomized comparative effectiveness study (Connect.Parkinson) comparing usual care in the community to usual care augmented by four virtual house calls from a remote Parkinson's disease specialist into participants' homes. The protocol details have been previously published. 5 The study was designed to enroll 200 individuals with Parkinson's disease and their care partners and has four specific aims: (1) to demonstrate the feasibility of using virtual house calls to deliver specialty care into the homes of individuals with Parkinson's disease who have limited access to care; (2) to show that such an approach can improve participants' quality of life; (3) to establish that telemedicine can enhance the quality of care received by participants; and (4) to demonstrate that this remote approach to care can save time, reduce travel, and decrease caregiver burden. The study was approved by the institutional review boards of the University of Rochester (coordinating center) and of the participating sites.
Participants
Eligible study participants are individuals with clinically diagnosed Parkinson's disease who have access to a nonpublic, Internet-enabled device with the capacity for videoconferencing and who are physically located in a state where a participating site investigator is licensed to practice medicine. Care partners, whose participation is optional, are family members or friends who provide regular, unpaid assistance with daily activities.
Recruitment and Enrollment
Recruitment for the study began in February 2014 and included efforts directed at patients and physicians. Based on previous research, 26 we identified counties in states where we had licensed specialists and where a majority of Medicare beneficiaries with Parkinson's disease do not currently see a neurologist. We targeted those counties using Google AdWords keyed to searches related to Parkinson's disease and through phone, mail, e-mail, and personal contacts to support groups and primary care providers. We also reached out to the Parkinson's community more broadly, announcing the study through electronic communications from the National Parkinson Foundation, a patient social networking site (PatientsLikeMe), and a posting in Fox Trial Finder (Michael J. Fox Foundation).
Interested participants were directed to a 1-page Web site (
Intervention
All participants received an e-mail link to secure, Health Insurance Portability and Accountability Act–compliant virtual visit software from SBR Health (Cambridge, MA) that embeds videoconferencing software from Vidyo (Hackensack, NJ) and is hosted by ID Solutions (Indianapolis, IN). Participants who did not have a Web camera received one (Creative Labs Live! Cam Chat HD camera; Creative Technology Ltd., Singapore) by mail. A study coordinator performed a test connection with participants prior to study visits and provided technical support by phone. No in-person support was provided.
All participants receive a baseline and end of study virtual visit with an independent rater. Those in the intervention arm are scheduled to receive four virtual visits over 1 year from a Parkinson's disease specialist. The exact content of each visit is determined by the clinician and patient but generally consists of a history, Parkinson's disease–focused examination, 23 addressing the patient's questions or concerns, and providing recommendations. Previous studies have demonstrated the reliability of remote clinical evaluation for Parkinson's disease in comparison with that of personal care. 23,30 Due to state law differences on prescribing medications remotely, 31 these recommendations, including medication changes (if indicated), are then mailed to the patient and the patient's local providers, who were notified at the study's outset of their patient's study participation, for implementation. Those randomized to their usual care in the community receive one video visit with a Parkinson's disease specialist after the 12-month visit with the independent rater.
Outcomes
The primary outcomes are feasibility, defined as the percentage of telemedicine participants who complete at least one telemedicine visit and the overall percentage of completed telemedicine visits, and efficacy, as measured by the change in the Parkinson's Disease Questionnaire 39, a widely used Parkinson's disease–specific quality of life measure. 32 Secondary outcomes include quality of care as measured by the change in the Patient Assessment of Chronic Illness Care, 33 time and travel savings, and change in caregiver burden as measured by the Multidimensional Caregiver Strain Index. 34
Sample Size
The sample size of 200 participants was selected to ensure adequate power of at least 80% to detect a moderate effect size on the quality of life measure, allowing for a 20% dropout rate.
Results
Enrollment
From February 1, 2014 to August 25, 2015, 11,734 individuals from 50 states and 80 countries visited the 1-page study Web site. Of these, 1,704 (15%) clicked through to the study interest form, and 927 (8%) completed it (Fig. 1). Most forms (79%) came from individuals in eligible states. Because initial interest was high, individuals who were not seeing a Parkinson's disease specialist were prioritized to the exclusion of others (n = 77), and 44 were excluded because enrollment was complete in their state's site. Ultimately, 272 individuals were referred to 18 research sites for consent, 210 enrolled in the study, and 195 were randomized. As shown in Table 1, most participants learned about the study from the National Parkinson Foundation Web site (n = 339), PatientsLikeMe (n = 204), and Fox Trial Finder (n = 132).
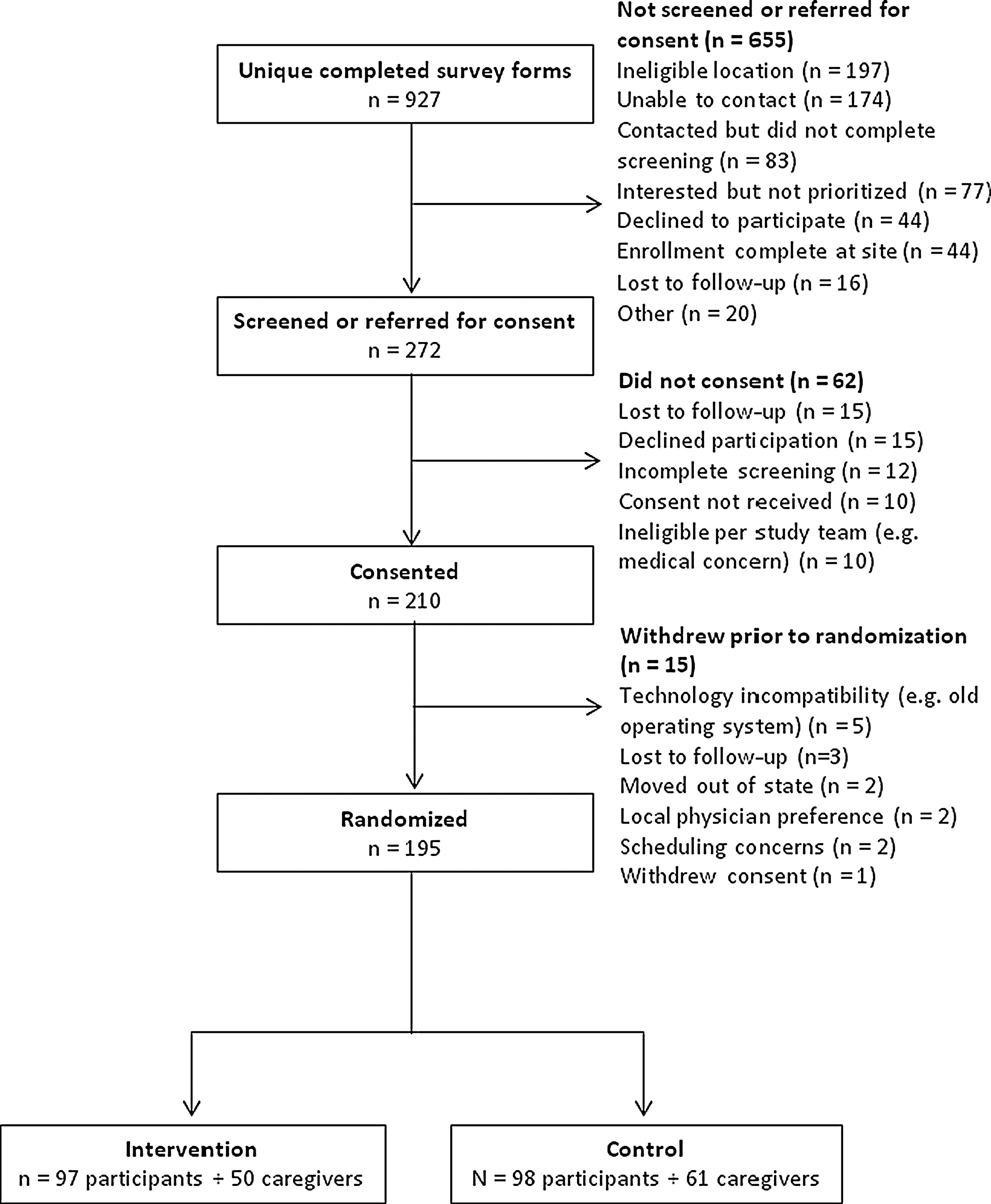
Flowchart of study participants.
Referral Sources of Interested Participants
The 927 participants provided 1,058 referral sources. Because participants could indicate multiple referral sources, percentages add up to more than 100%.
Study Population
Table 2 summarizes the baseline characteristics of the study population that underwent randomization. Fifteen individuals withdrew prior to randomization, which occurred after a baseline visit with an independent rater. The most common reasons for withdrawal were technological incompatibility (e.g., old operating system) and losses to follow-up (Fig. 1). The characteristics of those who withdrew (data not shown) were similar to those who were randomized. Most study participants are white (96%) and college educated (73%), with a mean age of 66 years and average Parkinson's disease duration of 8 years. At baseline, their mean Parkinson's disease–specific quality of life scores are relatively low, indicating mild perceived impairment. Participants' mean scores on the Patient Assessment of Chronic Illness Care are comparable to what has been observed in other chronic disease populations. Of our participants, 96% use the Internet or e-mail at home, and 54% have used their computer to participate in a video call. In the 12 months prior to enrollment, only 3% had not seen either a general neurologist or a Parkinson's disease specialist. However, 55% of participants come from a U.S. county in which fewer than 55% of Medicare beneficiaries with Parkinson's disease receive neurological care. Participants travel on average 52 miles each way to receive Parkinson's disease care.
Baseline Characteristics of Randomized Study Participants
Data are mean (standard deviation) unless otherwise noted. The number of responses is 195 unless otherwise noted.
Higher scores indicate greater disability.
Excludes “rigidity” and “postural stability” fields.
Lower scores indicate greater disability/dissatisfaction.
Table 3 summarizes the baseline characteristics of the participating caregivers. Like the participants with Parkinson's disease, most are white (79%) and college educated (55%).
Baseline Characteristics of the Participating Care Partners of Randomized Participants
Data are mean (standard deviation) values unless otherwise noted.
Higher scores indicate higher amounts of strain for caregiver.
Remote Assessments
At baseline, 177 (91%) of the 195 randomized individuals completed all 39 questions of the Parkinson's Disease Questionnaire 39. Of those who did not, 11 failed to complete one question, 5 failed to complete two questions, and 1 failed to complete three questions. Similarly, 180 (92%) provided responses to all questions of the Patient Assessment of Chronic Illness Care. Among care partners, 111 were randomized with the participants, and 72% answered all questions of the Multidimensional Caregiver Strain Index.
Discussion
Interest and enrollment in this national randomized controlled trial of virtual house calls suggest that latent demand for this care model is high and that remote recruitment and enrollment may be feasible. However, although the study reached those in geographically underserved areas, it did not reach those who are not seeing a specialist.
Over 10,000 individuals from all over the world visited the 1-page study Web site, and almost 1,000 individuals with Parkinson's disease expressed interest in participating in this study. This large latent demand for virtual visits, which initially surpassed our capacity to respond in a timely manner, is consistent with the experience of Kaiser Permanente of Northern California 35 and the Department of Veterans Affairs, 36 which have experienced large and rapid adoption of their various virtual visit models.
The principal driver of this interest may be convenience, 25,37 as most study participants are currently seeing a neurologist. For older individuals who generally live in suburban and rural areas, have limited mobility, impaired driving ability, and overburdened caregivers, receiving convenient, patient-centered care may be critical.
Enrollment also demonstrated the feasibility of entirely remote participation in research studies, at least through the initial phase. Nationwide recruitment, consent, enrollment, and completion of assessments were all completed by individuals with Parkinson's disease and their care partners without the need or potential benefit of an in-person encounter. Other clinical studies that have used remote approaches to evaluate therapeutics have demonstrated the feasibility of such an approach. 38 –43 That said, contacting many individuals was difficult because of telephone blocking services, absence of a prior relationship, and incomplete information provided. The inclusion of data checks to identify any missing responses would likely have reduced inadvertent omissions in sometimes lengthy forms and surveys.
Recruitment and enrollment in this study demonstrated the ability to address geographic but not socioeconomic barriers to care. Over half of the study participants come from counties with limited access to neurological care. Importantly, despite efforts to reach those who are not receiving care from a neurologist, the vast majority of study participants are seeing a neurologist. The characteristics of those with Parkinson's disease with the least access to care—older, rural dwelling, women, for example 26 —are very similar to the characteristics seen in those with the least access to the Internet and broadband. 44,45 Although broadband access is increasing, 46,47 recruitment and enrollment in this study were likely affected by the Digital Divide 48 —the difference in information between those who have access to the Internet and those who do not. 49 Internet access among individuals with chronic conditions is less than that of those without chronic conditions (72% versus 89%). 50,51 Participants in this study demonstrate higher usage of the Internet (96%) than the general population of adults (87%) and much higher usage than adults 65 years of age or older (57%). 52 The impact of the well-connected nature of this study population remains to be determined. Beyond increasing access to the Internet, future efforts will have to develop alternative approaches that likely rely on in-person contact, 53 such as outreach to local support groups and community leaders, to reach the most underserved.
Beyond the Digital Divide, the study encountered additional barriers that slowed enrollment. Despite great interest, enrollment in the study took 13 months, principally due to the need for review and approval of the protocol by each site's institutional review board. The limitations of local institutional review board review in multicenter studies, 54 –56 as well as the benefits of central institutional review boards, have been well documented. 57 –61 The other principal source of delay was the requirement for hand-signed consent forms, which could be addressed by adopting the electronic signatures that are increasingly used in clinical trials. 38
Beyond this study, virtual house calls face additional policy barriers, especially licensure and reimbursement. Because state medical licensing boards generally require that a physician be licensed in the state where the patient is physically located when services are rendered, we had to exclude nearly 200 individuals from participation simply because they lived in the “wrong” state. The Federation of State Medical Boards recently drafted a framework for an Interstate Medical Licensure Compact to enable expedited licensure in multiple states; 62 however, the speed at which such change will occur is questioned. 63 Last year, Congress reintroduced the TELE-MED Act, which would enable Medicare providers, like those in the Department of Veterans Affairs, who are licensed in one state to provide telemedicine services to Medicare beneficiaries in a different state. 64,65
The second major barrier is reimbursement. Fueled by state parity laws, 66,67 private insurers are increasingly reimbursing for telemedicine services, but Medicare is lagging. In 2012, Medicare spent approximately $5 million on telemedicine-related expenditures, 68 which was less than 0.001% of its total expenditures. 69 Moreover, Medicare provides no coverage of virtual house calls 70 and continues to incent institutional care over community-based care. 71 In organizations where licensure and reimbursement barriers have been addressed (e.g., Kaiser Permanente, the Department of Veterans Affairs), adoption of virtual visits has been rapid and welcomed.
In addition to difficulty enrolling a diverse population, this study has several limitations. The first is that it is almost exclusively focused on delivering care from a single specialist to an individual with a single chronic condition. Multidisciplinary care 72 delivered remotely could offer potentially greater benefits. For example, remote delivery of speech therapy 73 has already been found to be clinically valid and reliable in Parkinson's disease. Individuals with Parkinson's disease may suffer from multiple comorbidities that require personalized solutions, 74 some of which could be delivered remotely by other providers. In addition, almost all study participants had no preexisting relationship with the clinician whom they are seeing remotely. Combining in-person and virtual visits, especially after a diagnosis has been made, may provide additional benefits. Because of variation in state laws and policies, 31 the recommendations of the remote specialists in this study are communicated to the local clinician and participant for implementation. Although this may replicate some practices, more direct involvement of the remote specialist could enable more rapid and likely implementation of recommendations. Finally, although this study does not include a cost-effectiveness analysis, more frequent neurologist visits are associated with lower healthcare expenses due to a reduction in Parkinson's disease–related hospitalizations. 75
Overall, virtual house calls use technology to drive synchronous delivery of care directly to patients with lifelong conditions in their homes (Fig. 2). Such a model stands in contrast to the current institutional-based care that relies on colocation of a patient and clinician(s), generally in urban centers. Fueled by increasingly inexpensive and available technology, the next generation house call may deliver and increase access to patient-centered care for those with chronic conditions. Hopefully, this study will elucidate the benefits and limitations of this approach.
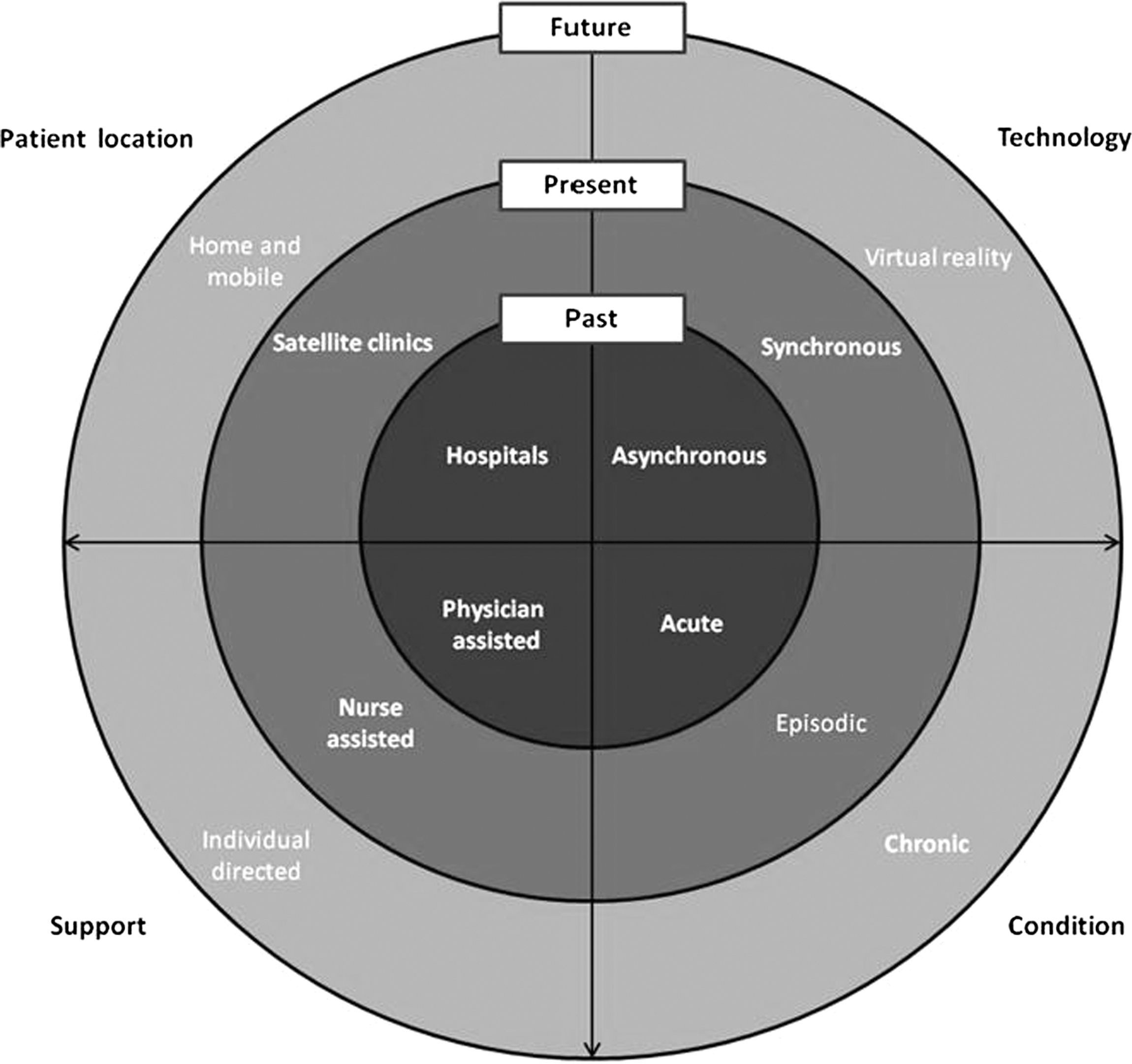
Expanding model of telemedicine care.
Footnotes
Acknowledgments
This research is supported by an award (AD-12-11-4701) from the Patient-Centered Outcomes Research Institute, and the National Parkinson Foundation is collaborating in the conduct of the study. Software used in the study is provided and supported by SBR Health (Cambridge, MA), Vidyo (Hackensack, NJ), and ID Solutions (Indianapolis, IN). The project described in this publication was supported by the University of Rochester CTSA award number UL1 TR000042 from the National Center for Advancing Translational Sciences of the National Institutes of Health. We would also like to thank Dr. David Brailer (Health Evolution Partners), Dr. Robert Kolodner (ViTel Net), Dr. Ruth Schneider (University of Rochester Medical Center), Ms. Kathryn Duderstadt (Struthers Parkinson's Center), Ms. Silvia Vargas-Parra (University of Miami), and Ms. Catherine Wielinski (Struthers Parkinson's Center) for their contributions to the study.
Disclosure Statement
E.R.D. has filed for a patent related to neurology and telemedicine, is an unpaid adviser to SBR Health and Vidyo, and serves on the Medical Advisory Board of and has stock options in Grand Rounds. K.M.B. has filed for a patent related to neurology and telemedicine. The remaining authors declare no conflicts of interest exist.