
Abstract
Background
Telehealth is defined by the U.S. Department of Health and Human Services as the use of electronic information and telecommunications technologies to support long-distance clinical healthcare, patient and professional health-related education, public health, and health administration. 1 The American Telemedicine Association defines telehealth as the use of medical information exchanged from one site to another through electronic communications to improve a patient's clinical health status. 2 It connects patients with physicians or other healthcare providers outside of the traditional office visit. 3 These technologies include videoconferencing, store-and-forward imaging, streaming media, and terrestrial and wireless communications. 1 The Medicare Telehealth Parity Act of 2015 Bill was introduced in the U.S. Congress last July; the bill opens the possibility of telehealth evaluation and follow-up in patients with chronic kidney disease (CKD) and with a kidney transplant. 4
CKD is defined by the presence of kidney damage or decreased kidney function for three or more months. 5 This is a worldwide public health problem; in the United States the prevalence is increasing because of the added incidence of diabetes mellitus, hypertension, and obesity. The 2014 U.S. Renal Data System (USRDS) Annual Data Report states that CKD is more common than diabetes mellitus and estimates that 13.6% of all adults have CKD and 12.3% of adults have diabetes mellitus. 6
As the incidence of renal conditions in the U.S. population continues to rise with a nephrologist shortage expected in the coming years, geographic barriers hindering patients from obtaining access to specialist care become more apparent. Telemedicine or telehealth has been identified as an essential instrument to assist in the care of patients with chronic conditions who reside in remote communities. 7,8 Telehealth permits specialized medical care in areas where specialists are otherwise not physically available. 2,3,9 There is experience in the use of telehealth (e-consults, provider–provider videoconference) in nephrology and other specialties with good outcomes. 7 –10 This is the first tele-nephrology study and analysis using patient–provider videoconferencing.
The Miami VA Healthcare System serves veterans in three South Florida counties: Miami-Dade, Broward, and Monroe, with an estimated veteran population of 175,000. We have one main tertiary hospital with multiple community-based outpatient clinics in a radius of 500 miles. To cover the three counties, in 2013 the Division of Nephrology implemented tele-nephrology to evaluate initial consults and follow up renal patients with multiple conditions, which include CKD, glomerulonephritis, and end-stage renal disease with pre- and post-transplant evaluation. The primary objective of this article is to evaluate the different types, uses, and benefits of the tele-nephrology clinic in our veteran community.
Materials and Methods
A retrospective, comparative, and descriptive study design was used to evaluate the effect of the tele-nephrology clinic intervention. Multiple clinical indicators were included in the analysis: blood pressure (BP) control (defined as less than 140/90), stabilization of the renal function (measured through glomerular filtration changes over time), and electrolyte/metabolic control. One hundred one patients who were evaluated in the tele-nephrology clinic between 2013 and 2015 were included. The repeated variable measurements were collected retrospectively over a follow-up period of 12–24 months, patients were seen two to five times during that time range with a mean number of clinic visits of 3.5. Patients were deemed suitable for tele-nephrology if they lived more than 40 miles from the nephrology clinic at the Miami VAMC. Patients traveled to four tele-nephrology clinic locations, and each visit was ∼20–30 minutes long. After patient arrival at the tele-nephrology clinic, vital signs were obtained by the telehealth nurse (BP, heart rate, respiratory rate, and temperature). The interaction between the patient and the physician occurred in real time using a secured videoconference system. Evaluation, discussion of the clinical findings, and a plan of care for the patient's renal condition were done using the videoconference system.
The statistical analysis was performed using SPSS version 22® and Minitab version 17®. Patient demographics and frequency of the variables were obtained.
Results
One hundred one patients were included in the analysis (Table 1), 95% of who were male (n = 96) and 5% of whom were female. (n = 5). The mean age was 65.5 years. The majority of the patients included were assigned to the Broward Clinic (79.2%, n = 80). Almost half of the patients were classified as CKD stage III (49.5%, n = 50), followed by CKD stage IV (13%, n = 14), and CKD stage II (7.9%, n = 8). The most common comorbidities were hypertension (present in 63.4% [n = 64] of the patients), type 2 diabetes (present in 26.7% of patients, n = 27), and HIV (5.9%, n = 6).
Patient Demographics
CKD, chronic kidney disease; ESRD, end-stage renal disease.
A one-way analysis of variance (ANOVA) between subjects was conducted to compare the effect of the tele-nephrology clinic on repeated BP and laboratory measurements at baseline, during treatment and post-treatment (Table 2). During the first visit to the tele-nephrology clinic, the mean systolic BP was 137.19 ± 22.27 mm Hg and the mean diastolic BP was 75.3 ± 13.07 mm Hg; changes to medications were made during the tele-nephrology clinic appointments, and in the last documented visit to the clinic the mean systolic BP was 125.14 ± 14.65 mm Hg and the mean diastolic BP was 69.7 ± 11.15 mm Hg. This was consistent with a decrease of 12.05 mm Hg in the systolic BP and 5.58 mm Hg in the diastolic BP. ANOVA showed that the effect of the tele-nephrology clinic intervention on reducing BP was statistically significant (for systolic BP, DF: 2, F value: 12.17 and p value <0.0001 (Fig. 1); for diastolic BP, DF: 2, F value: 5.57 and p value: 0.0042). The post hoc analyses using the Tukey method with a 95% confidence interval (CI) indicated that the mean systolic and diastolic BP at baseline and after treatment were both significantly different with an adjusted p value of <0.0001 and 0.0027, respectively (Table 3: summary of ANOVA for laboratory repeated measurements).
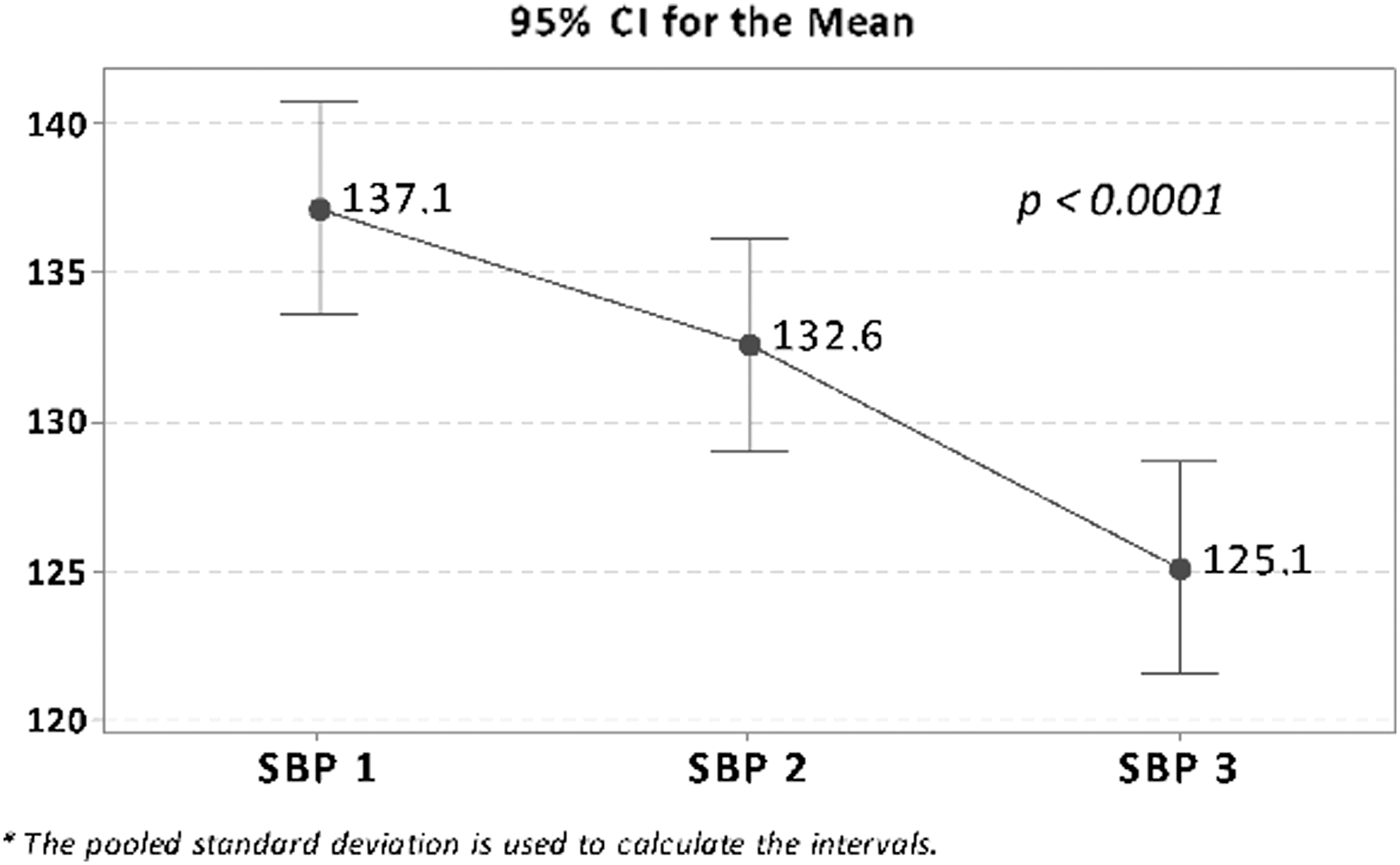
Interval plot of systolic blood pressure. SPB: Mean systolic blood pressure values obtained during the tele-nephrology visits.
Laboratory and Blood Pressure Measurements By Time
CI, confidence interval; SD, standard deviation.
Summary of ANOVA for Laboratory Repeated Measurements
p Value statistically significant if less than 0.05.
ANOVA, analysis of variance.
The mean renal function of this sample of patients improved over time, with stabilization of the glomerular filtration rate and even a mild improvement in some patients (Fig. 2). The mean creatinine among patients at their initial evaluation in the tele-nephrology clinic was 2.23 ± 1.5 9 mg/dL, and the mean creatinine at the final visit was 1.97 ± 1.49 mg/dL. The creatinine changes over time were not statistically significant (DF: 2, F value: 0.74 and p value: 0.47). Potassium showed a significant improvement in this sample (DF: 2, F value: 4.96 and p value: 0.0076). Post hoc analyses using the Tukey method and 95% CI indicated that the mean potassium measurements at baseline and after treatment were both significantly different with an adjusted p value of 0.0050. Phosphorous and bicarbonate did not show a statistically significant improvement (p value 0.79 and 0.91, respectively).
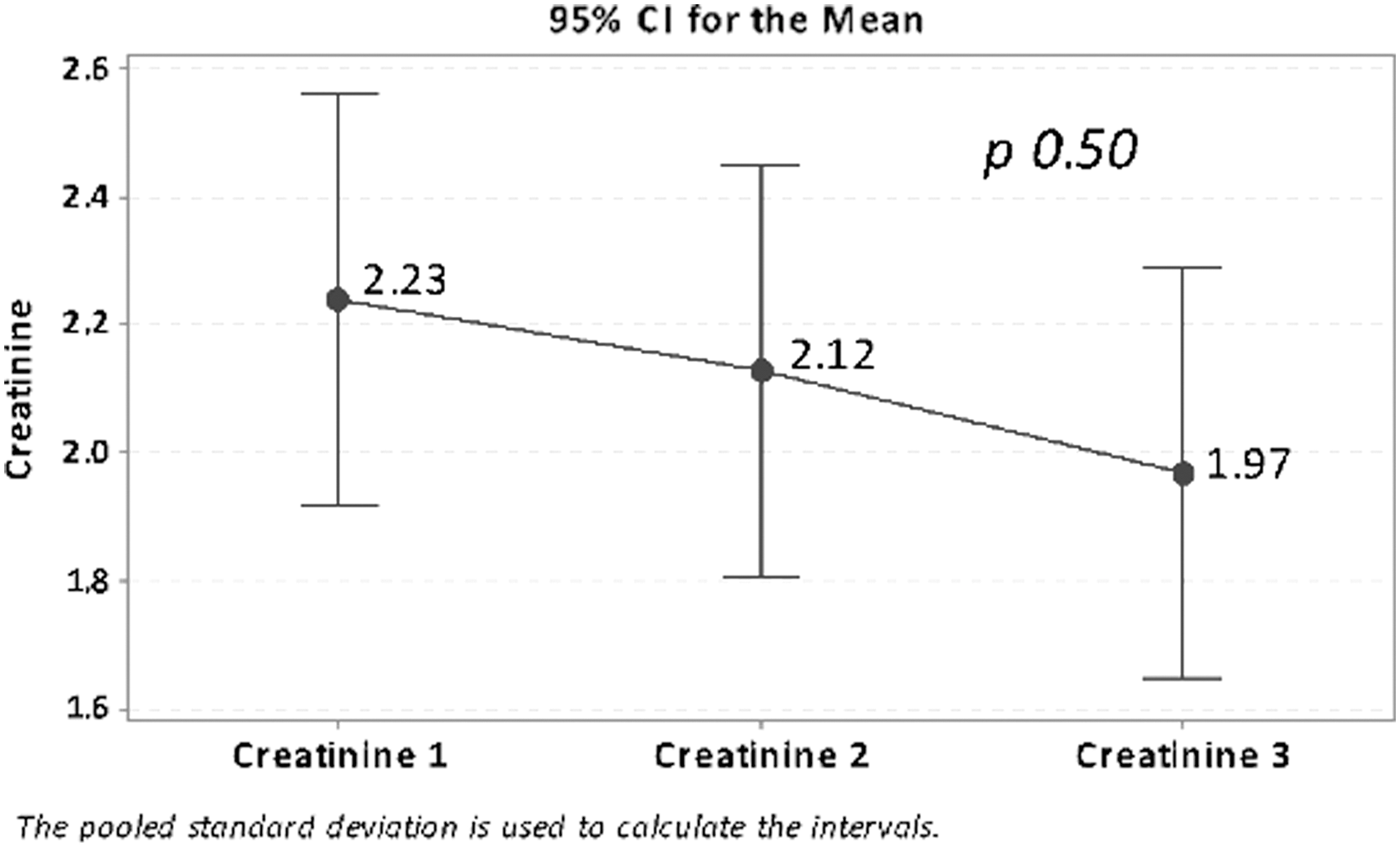
Interval plot of creatinine. Mean creatinine values obtained during the tele-nephrology visits.
Conclusions
This is the first study that evaluates face-to-face tele-nephrology applications. The goal of tele-nephrology is to optimize the delivery of renal care in underserved areas. In this pilot study, we showed that with the tele-nephrology clinic intervention, we were able to effectively improve BP control in patients with kidney disease who reside in underserved areas. In addition, stabilization of the glomerular filtration rate was achieved along with control of the electrolytes. For patients who reside in remote areas, tele-nephrology allows access to a renal specialist. This innovative patient-centered tool allows nephrologists to improve the patient experience of care and healthcare outcomes and may afford potential opportunities to reduce the cost of healthcare in patients with multiple renal conditions.
Footnotes
Disclosure Statement
No competing financial interests exist.