
Abstract
Introduction
Brazil, like many countries in the world, faces a challenging epidemiological context in which mother/child diseases, malnutrition, and parasitic infections coexist with ageing populations, an epidemic of chronic diseases, and increasing rates of road traffic injuries and violence. Life expectancy, now at 73 years, is expected to reach 82 years in Brazil in 2030, with the number of elderly surpassing that of children and adolescents. 1,2
To face these challenges, Brazil began more than 25 years ago to build a universal public healthcare system—the Unified Health System (SUS)—structured around the principle of primary care. 3 However, despite many achievements, the SUS faces systemic problems, such as the fragmentation of its service network, with important gaps between primary and specialized healthcare. 4 Large hospitals providing high-quality technology-intensive services are available, but they are not capable of meeting the growing demand for care. Added to that, the quality of care provided by specialty clinics and primary care services is heterogeneous, technological resources are limited, and coordination mechanisms are lacking.
In this scenario, telemedicine/telehealth initiatives can play a major role in bridging the gap between levels of care. As defined by the Institute of Medicine, telemedicine is “ … the use of electronic information and communication technologies to provide and support healthcare when distance separates the participants.” 5 With the ability to overcome physical access barriers, support effective interventions regulated by mechanisms that promote equity, and prevent overmedicalization (quaternary prevention), telemedicine technologies can be implemented at a reasonable cost and scale plays a strategic role in the consolidation of healthcare networks. 6 –10
In 2007, the Brazilian Ministry of Health, through its Department of Health Education Management, supported the creation of nine telehealth working groups in the country. These telehealth groups were linked to public universities, among which the Federal University of Rio Grande do Sul (UFRGS). In 2010, the UFRGS pilot project was expanded to become a full-fledged government program [Programa Telessaúde Brasil Redes: TelessaúdeRS/UFRGS]. 11
Currently, TelessaúdeRS/UFRGS (
Materials and Methods
This descriptive article outlines the main telemedicine initiatives developed by TelessaúdeRS/UFRGS in focal areas: professional teleconsultation (clinical problem solving and medical regulation), telediagnosis, tele-education, development of telemedicine solutions and technologies, and support for implementation of IT solutions.
To carry out these actions, Telessaúde/UFRGS relies on a system that combines hardware, software, database, and networking components. For all services, data are moved along a fiber optic network backbone established by the Ministry of Health and Technology, running across the country and interconnecting federal universities. Teleconsultation and telediagnosis inquiries are recorded and responses are posted on the National Telehealth Platform (Plataforma Nacional de Telessaúde), a Web-based information system developed using the Python programming language and stored in a PostgreSQL database. Any changes in the work process requiring improvement or remodeling of platform features are tested before implementation in a prototype environment developed in Microsoft Sharepoint 2010. A Solidus Contact Center is used to manage the 0800 hotline. Tele-education initiatives are hosted in the open-source Moodle platform. The open source Mconf system (
Professional Teleconsultations
Attending physicians can discuss cases with a teleconsulting physician through an electronic platform or toll-free call. Web-based consultations have been available since 2007 in synchronous (real-time videoconference) or asynchronous (texting) modes. The consultation starts when a registered system user fills a short electronic form requesting an answer to a clinical question. This query is evaluated and classified by a medical regulator. The main goal of the medical regulator at this stage is quaternary prevention (preventing referral to a wrong specialist, overdiagnosis, and overtreatment). After regulation, a teleconsultant provides a brief response based on the best available clinical evidence (Fig. 1).

Flow of request, regulation, response, and evaluation of teleconsultations, TelessaúdeRS, Brazil, 2015.
A toll-free number (0800 hotline) is available for consultations over the phone. The hotline was established in March of 2013. Physicians from across Brazil and nurses from the state of Rio Grande do Sul have access to the hotline, Mondays through Fridays, from 8:00 a.m. to 5:30 p.m. General practitioners answer the calls and act as medical regulators to judge the need to involve specialists. Questions are answered in real time, based on the best available evidence and considering the local conditions and resources available to the caller.
Teleconsultations can also occur in the opposite direction, which is initiated by teleconsultants who propose case discussions with attending physicians regarding referral of patients to specialty clinics. This initiative, called RegulaSUS, was established in 2013. RegulaSUS relies on two strategies to organize the access of patients to specialty clinics: referral protocols and clinical case discussions of waitlisted patients. The protocols focus on the most frequent reasons for referral in each medical specialty. Specific protocols define clinical situations that require face-to-face medical assessment in a specialized medical service. Medical regulators apply these guidelines to waitlisted patients, with deflection of patients deemed adequate for diagnosis and/or treatment at primary care units. The consulting physician in the 0800 hotline discusses the patient with the attending physician to define the need for referral, optimize clinical conducts, and guide follow-up at the primary care level. This process is currently being implemented for a number of specialties: endocrinology, nephrology, pulmonary medicine, oral medicine, urology, neurology, neurosurgery, rheumatology, thoracic surgery, gynecology, and infectious diseases.
Telediagnosis
TelessaúdeRS/UFRGS has provided this service since 2013, specifically focused on pulmonary function tests (spirometry). State-based primary care physicians may request a spirometry through the Telehealth Platform. The request is regulated and, if accepted, a team member contacts the patient to schedule the test. 12,13 For this test, patients must travel to one of eight cities, located in major geographic areas to reduce travel time as much as possible. Test results are forwarded to the TelessaúdeRS/UFRGS headquarters for interpretation by pulmonary medicine specialists. A report is then produced and forwarded to the requesting physician through the Telehealth Platform.
Tele-Education
Tele-education initiatives target the different professions involved in primary care, taking into consideration specific needs for continued professional education and learning preferences. Thus, multiple programs are developed for each topic. The following topics are covered: second opinion; teleconsulting responses for relevant replicable topics; distance learning; collaborative care in mental health and prenatal care (discussion of cases); and Web Balint groups and Web problem-based interview with a focus on physician-patient clinical communication. All these activities are available on YouTube® (
Telemedicine Solutions and Technologies
Telehealth services are developed on demand. Service data recording, monitoring, and evaluation systems are developed by the TelessaúdeRS/UFRGS team in partnership with private companies. Systems are always tested before implementation. These pilot projects generate information to support the development of flexible collaborative platforms that can be swiftly updated and refined. Following the pilot stage, processes and documentation are analyzed (access profiles, variables, validation conditions, etc.) using business process management. This information will support the development of the final IT solution by a private partner with supervision from the TelessaúdeRS/UFRGS team. Following development of the system, the final version is cleared by the TelessaúdeRS/UFRGS team and made available for user training and full implementation.
Support for it Systems
Since 2014, TelessaúdeRS/UFRGS has worked with primary care facilities in the state of Rio Grande do Sul to implement e-SUS AB, an electronic health record (EHR) system created by the Ministry of Health. Support may be provided through face-to-face training at the facility, distance training through Web conferencing or Web talks, or teleconsulting using the Telehealth Platform. All these actions cover both technology-related or usage issues. The most important tool for EHR implementation is an 8-h face-to-face module at primary care facilities preceded by a preparatory videoconference with the primary care team.
Results
Professional Teleconsultations
Between December 2007 and September 2015, 15,536 healthcare professionals from 1,241 primary care services in the 497 municipalities of the state or Rio Grande do Sul registered to use the system. This translated into benefits for 11,000,000 state residents. During this period, 31% of the registered users, 86% of the primary care units, and 88% of the municipalities submitted at least one request, for a total of 15,441 queries. Of the total queries, 85% were asynchronous and 15% were synchronous (VoIP). The highest number of requests came from nurses (36%), community health agents (25%), and physicians (15%). Users were satisfied or extremely satisfied with the service provided in 95% of the cases, with full resolution of the query in 85% of them. Unnecessary referral to higher levels of care was avoided in 66% of the teleconsultations.
The 0800 hotline handled 21,281 inquiries between March 2013 and September 2015. The service was used mainly by physicians from the South (51.6%), Southeast (20.7%), and Northeast (15.3%) regions of Brazil. Among users who answered the satisfaction survey, 99% were satisfied or extremely satisfied with the service. Among requesters who intended to refer a patient to higher levels of care, 74% changed their decision following the consultation. In the first semester of 2015, the 0800 hotline handled 2,898 calls; 50% of these calls were made by 10% of the total number of physicians using the service in this period. The main topics of these calls according to ICPC-2 were administrative procedures (A62), noninsulin-dependent diabetes (T90), uncomplicated hypertension (K86), pregnancy (W78), hypothyroidism (T86), insulin-dependent diabetes (T89), Hansen's disease and other infectious diseases (A78), urinary tract infection (U71), other skin disorders (S99), syphilis (X70), tuberculosis (A70), dermatophytosis (S74), hyperthyroidism (T85), and chronic skin ulcer (S97).
The RegulaSUS project discussed 13,774 clinical cases through telephone consultations. Specialty referrals were canceled by attending physicians in 57% of cases, which were then treated at the primary care facility. Only 16% of the cases were in fact referred for specialized attention. For the remaining 27%, municipal services were requested to provide additional information, either because the patient records were not found or the attending physicians did not agree to discuss the case (3%). Of the nephrology teleconsultations, 44.8% resulted in cancellation of referral to specialized care, versus 33% in which referral was maintained. In pulmonary medicine, 53% of the referrals were cancelled and 16% were maintained; and in urology, 56.8% were cancelled and 7.1% were maintained.
Telediagnosis/Spirometry
Until this moment, 4,700 spirometry tests have been performed. Of these, 2,914 were performed between January and August 2015, when implementation of the Telespirometry Centers was completed (Fig. 2). The mean time between test request and delivery of the report to the requesting physician was 20 days.
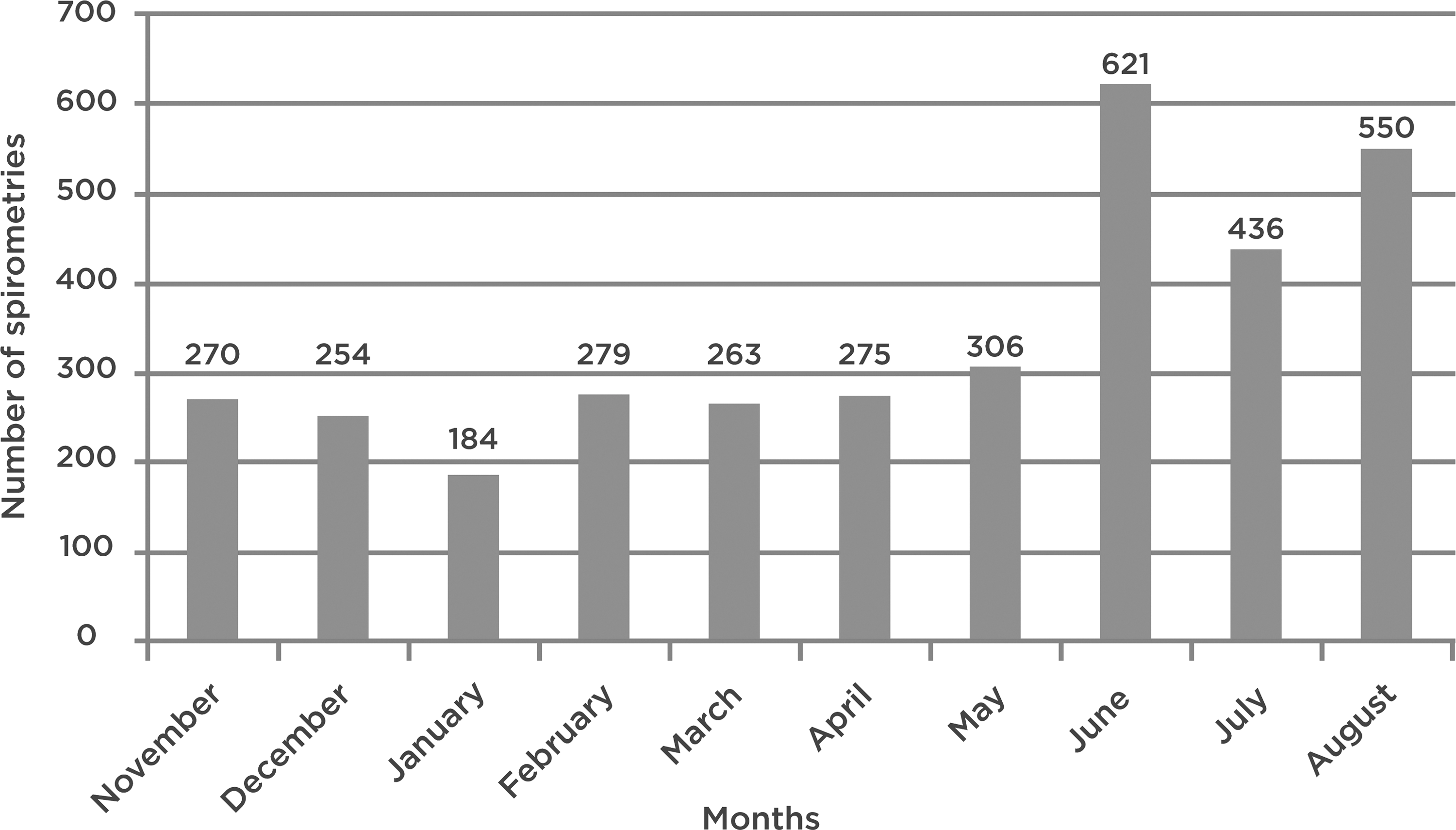
Monthly spirometry requests from November 2014 to August 2015, TelessaúdeRS/UFRGS, Rio Grande do Sul, Brazil, 2015.
Tele-Education
Between January 2009 and June 2015, TelessaúdeRS/UFRGS published 688 second-opinion protocols, equivalent to 87% of the protocols published in the Virtual Health Library. It also produced 28 editions of distance learning modules for 1,778 participants; 24 meetings focusing on collaborative care in mental health and prenatal care for primary care physicians and nurses; and 170 Web talks with participation of more than 7,500 professionals. Videos posted in the Internet were viewed by more than 300,000 professionals.
Telemedicine Solutions and Technologies
Telehealth services are currently provided through an online platform accessible to SUS primary healthcare professionals: the National Telehealth Platform. Registered users number 44,800 healthcare professionals, with 2,500 monthly requests for teleconsultations and telediagnosis support. The platform is used by 25 Telehealth Groups across Brazil and staffed by 540 teleconsultants. Five apps have also been developed to support decision-making (dietary assessment, glomerular filtration, cardiovascular risk, gestational age, and alcohol abuse), with more than 10,000 downloads. Another five apps are being released and 12 are being developed, for a total of 22 apps for mobile devices.
It Solutions
TelessaúdeRS/UFRGS supported implementation of e-SUS in 1,192 primary care units, with training of 14,400 healthcare professionals. Over 2,068 primary care services (87% of all primary care services in the state of Rio Grande do Sul) had their IT structure mapped. In addition, 462 face-to-face trainings for the implementation of e-SUS AB EHR system were provided, along with 813 web conferences and 4,942 teleconsultations about EHR. According to the Ministry of Health, 1,164 primary care services in Brazil have implemented the e-SUS AB EHR. Of these, 431 primary care units (37.02%) are located in the state of Rio Grande do Sul.
Discussion
The size and national reach of TelessaúdeRS/UFRGS are a testimony to the progress of telemedicine in Brazil. Together with the number of professionals served, the scope and variety of initiatives show the potential of telemedicine to guide the process of decision-making within the context of primary healthcare. As stated by Oxman et al., 14 “There are no ‘magic bullets’ for improving the quality of healthcare, but there are a wide range of interventions available that, if used appropriately, could lead to important improvements in professional practice and patient outcomes.” To bridge the gap between primary and specialized healthcare, TelessaúdeRS/UFRGS develops multifaceted initiatives—ranging from the implementation of IT systems to software development, tele-education programs, support for clinical decision-making, and qualification of patient care. All these initiatives originate from a careful epidemiological diagnosis to focus on the major health needs of the population in the state of Rio Grande do Sul and Brazil. They also take into consideration the most common questions of primary care physicians to provide continued professional education for these professionals strengthening the problem-solving capacity of the Brazilian primary healthcare system. 15
The limitations for the expansion of telehealth in Brazil include infrastructure aspects, access barriers, legal constraints, and policies regulating information technology development and innovation. Primary care services lack equipment and Internet connectivity, which prevents further dissemination of telehealth services. A 2012 survey by the Ministry of Health, in which 38,812 primary healthcare services were evaluated in the five regions of Brazil, showed that only 51% (range: 26–72% across five regions) reported having a computer, 35% (13–60%) reported Internet access, and 12% (3–23%) reported participating in telehealth activities. In addition, the availability of health information in the SUS is fragmented, with data scattered over 30 different systems, leading fragmentation, failures in coverage, and low level of support for decision-making. 16
Another limitation of TelessaúdeRS/UFRGS is the relatively low utilization level considering the potential number of users—over 50,000. This, however, seems to be an international phenomenon. Alkmim et al. 17 mention the following determinants of teleconsultation service usage: no clear evidence of impact on health indicators, user perception of usefulness, benefits, and limitations, and no clear evidence of cost-effectiveness, deficient infrastructure, acceptance of technology, and ethical and legal aspects. 17 Therefore, teleconsulting service usage is low in both the national and international scenarios, with less than one teleconsultation inquiry per primary care service per month. 17 In our service, 10% of the active users made half the calls to the teleconsultation hotline in the first half of 2015, while many others never used the service. Another issue that is still relevant in Brazil is the high number of primary care professionals who are digitally illiterate (1/3 below a minimal/ideal level). 18 Conversely, many reviews have shown a positive effect of telehealth on the prevention of unnecessary referrals to higher levels of care, admissions, and emergency consultations. 8,19 Specific limitations of the Brazilian setting that hinder further expansion of telehealth include a resolution of the Brazilian Federal Medicine Council that prohibits teleservice (ICT-mediated) encounters between patients and physicians and a bureaucratic and restrictive policy for the development of information technologies and innovation. 20
To counterbalance that, a generous federal policy to support the development of telehealth centers has been in place since 2007. Along the same lines, some Brazilian states have provided robust financial support for some local initiatives, as is the case of our own Center. 21 –24
The variety of services and teleconsultations provided at the TelessaúdeRS/UFRGS Center is remarkable, but not unique in the national scenario. Also noteworthy are the telehealth initiatives in the states of Santa Catarina and Minas Gerais, both established in 2005, with over two million test reports in several specialties and 1,600,000 electrocardiograms, respectively. 25,26 Telespirometry has been the main contribution of TelessaúdeRS/UFRGS to telediagnosis until now, selected due to the high prevalence of asthma and chronic obstructive pulmonary disease in the state, with access to the test regulated by strong scientific evidence.
Implications for Public Policies
The case of TelessaúdeRS/UFRGS shows that even in the presence of social inequality and economic limitations, telemedicine is potentially useful to qualify the healthcare provided to the population. In future, the scope of telehealth initiatives is expected to increase to encompass health service planning, monitoring, evaluation, and interventions. 18 We hope that telemedicine will ultimately bring healthcare services closer to the population by consolidating a wide network interconnecting SUS services and bridging the gap between primary and specialized healthcare. Telemedicine will possibly strengthen the lines linking healthcare facilities and healthcare professionals, serving as a robust strategy to the effective implementation of healthcare networks with the ultimate goal of providing correct, humanized, and equitable care, at the right time and at the right place, at the right cost, with adequate quality.
Footnotes
Acknowledgments
Financial support for this project is provided by the National Research Council (CNPq), Ministry of Health (Education and Work Management Office/Department of Health/Department of Health Education Management and Office of Healthcare/Department of Primary Care), and Rio Grande do Sul Department of Health.
Disclosure Statement
No competing financial interests exist.