
Abstract
Introduction
The inequality of healthcare between urban and rural areas is the primary cause of disparities in health delivery and utilization in China. In particular, there is a shortage of experts in rural areas. 1 Delayed diagnoses and inappropriate medical management are common in these areas, often resulting in public dissatisfaction. The development of the Internet has improved digital technologies in medical care. In recent decades, telemedicine has developed rapidly in many countries, which enabled easy access to specialists in large hospitals, thereby enhancing the delivery of clinical care and improving the practice level of small hospital doctors in rural areas. There is reliable evidence that telemedicine is a solution to several deficiencies in the country's health sector.
Telemedicine reduces costs and avoids risky road transfers. 2 –4 The specialists in the hub have more specialized knowledge and the ability to collect additional information by viewing patients and their families and clinical data, including laboratory results. 5 It has been applied in neurology, dermatology, radiology, and cardiology. 3,6 –8 Like many other developing countries, such as India 9,10 and Brazil, 11 the Chinese government began to use this technology as a strategic tool for improving China's medical and healthcare delivery system. A large number of telemedicine programs have been established since the mid-1980s. 12 Recently, the Chinese government decided to use telemedicine for promoting medical reform. Several locations have attempted to include telemedicine in gerontology in basic medical and new-style rural insurance. 13 In the last decade, China has accumulated telemedicine experiments in diagnosis accuracy, treatment improvement, and cost saving in rural areas.
To the best of our knowledge, there are few reliable published data regarding the utilization and cost-effectiveness of the program, despite recent major developments in nationwide telemedicine programs in China. 14 –17 We conducted a point-in-time study based on a visual (or video) telephone medical care management system established for western regions in China. We evaluated the regional distributions, types of diseases, diagnosis and treatment changes, and estimated cost saving of the telemedicine program.
Materials and Methods
Study Design and Setting
This is a 12-year cross-sectional analysis of a telemedicine program in western regions of China. As one of the essential Web sites of the Chinese project, the Telemedicine Center at the West China Hospital (TCWCH) was established at the end of 2001. TCWCH comprises hub and spoke interactions, whereby the WCH serves as the telemedicine hub and the spoke refers to the patient's location. With the support of the government, the telemedicine networks extended to more areas after the May 12, 2008, Wenchuan earthquake. The WCH provided long-distance medical education and consultation for the difficult cases.
The Public Affairs Development Department of the hospital is responsible for the organization and management of telemedicine services. The telemedicine system consists of a digital network with high-speed data transmission up to 2 Mbps. The TCWCH has seven sets of two-way video equipment and image transfer that can be used in simultaneously conducting long-distance education or consultation.
Ethics Statement
The study design was approved by the ethics committee of the West China Hospital of Sichuan University (SCU). All of the patients or their families provided written informed consent to participate in the study and the whole study was conducted in accordance with the principles expressed in the Declaration of Helsinki.
Participating Centers and Doctors
The TCWCH has more than 1,200 experts and healthcare professionals, who are beyond the attending doctor level and who come from first-class medical institutions in western China, including the West China Hospital, SCU, West China Women's and Children's Hospital, West China Hospital of Stomatology, SCU, West China School of Public Health, SCU, and School of Public Administration, SCU. Their specialties cover internal medicine, surgery, obstetrics and gynecology, pediatrics, stomatology, radiology, and laboratory medicine. The specialists in the hub take turns being on duty to maintain contact with the TCWCH. The local doctors from the spoke hospitals are medical practitioners who graduated from legitimate medical colleges with a bachelor's degree in clinical medicine and hold a medical practitioner's license. The local doctors initiated the telemedicine consultations. The TCWCH staff provided all of the medical practitioners with standard training for the administration of telemedicine services.
Interaction availability 24 h a day ensured access to an application for telemedical visits at any time. In accordance with the practical demand of spoke hospitals, all of the visits were classified as one of the following two teleconsultations, (1) ordinary consultation and (2) emergency consultation, which was performed either on the day of requirement or within 24 h. The flowchart is shown in Supplementary Figure S1 (Supplementary data are available online at
Data Collection
Patients and their family members in spoke hospitals were informed about the consultant and were asked to attend the telemedicine visit with their doctor together. They could decide whether or not to have the teleconsultation (The most possible reason is economic difficulty). A flowchart depicting how the final study population was selected is displayed in Figure 1.

Flowchart of teleconsultation patients through recruitment and selection.
For each consultation, the patients’ demographic data, such as age, gender, medical history, physical examination, and laboratory and imaging results, were transmitted to the TCWCH before the scheduled session. During the teleconsultations, which were all conducted on video, the consulting specialist questioned the patient or the family members if the patient cannot be present (for instance, intubated in the intensive care unit [ICU]), directed the local doctor to perform a physical examination, and discussed in real time the diagnosis and treatment with the spoke practitioner. Additional materials, such as further investigations, were requested if needed. Suggestions regarding diagnosis and management in written form were provided to the local doctors, who chose to accept or reject these recommendations.
We measured the impact of teleconsultation according to how clinical care was changed by calling the local doctors 90 days after the telemedicine sessions. The final diagnoses were determined, all of which were classified according to the ICD-10 system. 18 Three doctors from our department (C.H., X.M.-Z., and J.C.-R.) compared the original diagnoses with the final ones and assessed whether or not they were changed after teleconsultation.
We further divided diagnosis changes into minor diagnosis change and major diagnosis change types in the postconsultation survey to reflect the level of discordance between the diagnosis rendered by the local doctors at the time of original submission and the final diagnosis in each case. Minor diagnosis change is defined as follows: the final diagnosis is modified, but can still be grouped in the same subclassification of the ICD-10 system as that of the original, and the patient treatment is not affected. Major diagnosis change is defined as follows: (1) the final diagnosis is completely changed and, in contrast to the original classification, is grouped into a different subclassification of the ICD-10 system and (2) a minor diagnosis change with an impact on patient treatment. Treatment change was divided into two types: (1) treatment change linked with diagnosis indicates that the treatment after teleconsultation changes due to the change in the diagnosis and (2) treatment change not linked with diagnosis is used when the treatment changes, although the diagnosis remains the same.
In addition to improvement in clinical-related outcomes, we theoretically compared the actual costs of providing telemedicine with the potential costs of in-person visits from a societal perspective, which included two conditions: patients traveling to the hub and specialists traveling to the spoke hospitals.
The direct medical costs included consultation fees and registration fees obtained from West China Hospital. We regarded maintenance and staff costs of telemedicine as running costs. 19,20 Maintenance costs included the operating and repair costs of the telehealth equipment. Staff costs consisted of the annual salaries and overheads of the telemedicine administrative personnel. The primary costs associated with face-to-face consultations were due to travel and accommodation, which represented savings in the telemedicine model. Transportation expenses were calculated by the two-way average travel cost for two persons (the patient and one accompanying family member) or one specialist by the number of consultations that occurred at each site according to the annual statistics almanac of Sichuan. 21 Under the usual care model, at least one overnight accommodation for patients and accompanying family members in Chengdu during the appointment was required. If the specialists were in the hub, the outpatient costs were calculated by multiplying the mean time of travel to the spoke hospitals (in hours) by the specialists’ hourly salary.
To further analyze cost–savings related with treatment change in specific diseases after teleconsultation, we used cerebrovascular diseases (CVDs) as an example. A total of 100 cases of all the CVD patients were chosen randomly using Microsoft Excel (version 2010) to generate random numbers, and the costs per day before and after teleconsultation were directly compared.
The initial valuation of cost items was determined in Chinese currency, renminbi (RMB,  ). All cost savings were subsequently converted to U.S. dollars ($) based on the exchange rate in each year.
21
). All cost savings were subsequently converted to U.S. dollars ($) based on the exchange rate in each year.
21
Statistical Analysis
The predefined standards for data collection were applied from May 2002 to December 2013. IBM SPSS 20.0 (IBM SPSS, Inc., Chicago, IL) was used for performing the statistical analysis. Descriptive statistics were used to describe the details of teleconsultations, the demographic features, and clinical outcomes. The continuous data are shown as the means and standard deviations. The proportions of cases, disease distributions, and patients who were suggested to receive further examination were analyzed using Pearson χ 2 tests. 22 Two-tailed tests were used, and p < 0.05 was considered to be statistically significant.
The mean values and ranges of cost data are provided. We perform a Mann–Whitney U test to compare the differences between the groups. One-way sensitivity analysis for the estimation of cost was performed to test the robustness of the results in net savings 20 and address potential sources of bias. This analysis was based on a number of assumptions regarding contributing variables. The robustness and extent to which the findings could be generalized were explored by changing the values of the variables in the analysis. The missing data were omitted.
Results
General Characteristics
From 2002 to 2013, a total of 11,987 teleconsultations were conducted. Among them, 1,463 were repeated. The 249 spoke hospitals consisted of 53 tertiary hospitals, 151 secondary hospitals, and 45 primary hospitals from 112 cities in 13 provinces, municipalities, and autonomous regions, including Sichuan (89.0%), Xinjiang (2.3%), Tibet (2.1%), and so on (Supplementary Fig. S2). There were 235 (94.4%) general hospitals, 7 psychiatric hospitals, 2 orthopedic hospitals, 2 tumor hospitals, 1 geriatric hospital, 1 maternity and child care hospital, and 1 anorectal hospital.
Thirty-two hospitals (12.9%) sent more than 100 consults each during the 12 years, while 134 hospitals (53.8%) sent less than 10 consults, and 83 hospitals (33.3%) sent 10–100 consults in the meantime. We further analyzed the distribution of teleconsultation cases from the 32 hospitals, which sent most of the consults from 2002 to 2013 (Supplementary Table S1); 87.5% of them came from Sichuan and 53.1% were from secondary hospitals.
The mean age of the patients was 49.6 ± 19.3 years (range, 1 day–95 years). The patients who were aged 15–64 years constituted 70.9% of all of the patients; 63.6% were males and 5.3% of the participants were ethnic minorities, including the Tibetan, Yi, Uyghur, Naxi, Kazak, Mongolia, Hui, and Qiang people. The general characteristics are shown in Table 1. After the 2008 Wenchuan earthquake, the total number of spoke hospitals, teleconsultations, and patients increased to 249, 9,152, and 8,110, respectively. The average chain growth rate in the number of spoke hospitals was 35.2% from 2002 to 2013. The average chain growth rate in the number of teleconsultations was 28.7% during the same period. They all have been increasing steadily in recent years (Supplementary Fig. S3).
General Characteristics of Patients Using Telemedicine in the Telemedicine Center at West China Hospital
SD, standard deviation.
Values are expressed as a number (percentage) unless otherwise indicated.
The numbers of telemedicine consultations from ordinary wards, emergency rooms, and ICUs were 8,682 (72.4%), 1,801 (15.0%), and 1,504 (12.5%), respectively. The mean response time was 1.6 ± 1.7 days (0–14 days). The numbers of emergency and ordinary consultation cases and changing trend of response time are shown in Supplementary Figure S4. The range is 1.1 days for emergency consultation and 1.6 days for ordinary consultation. Consultation requests for diagnostic support and treatment suggestion were 55.5% and 44.5%, respectively.
Distribution of Diseases
The diagnoses were confirmed in 10,995 cases (91.7%), while others still remained undetermined in a postsession evaluation. The final diagnoses covered every classification of the ICD-10 system (Table 2). Neoplasms (19.4%), injuries (13.9%), and circulatory diseases (10.3%) were the three most common diagnoses, followed by diseases of the digestive system (8.0%) and the respiratory system (7.6%). Supplementary Figure 5 shows the distribution of the final diagnoses and changes of the five most common diagnoses in the 12-year period.
Clinical Characteristics and Outcomes of Teleconsultations by Categories of Diseases
p-Value using a χ 2 test for categorical variables comparing the differences between any of the four study groups.
Note: Values are expressed as a number (percentage) unless otherwise indicated.
Among the neoplastic diseases, the most common diagnoses were malignant neoplasms of digestive organs (34.4%), followed by malignant neoplasms of respiratory and intrathoracic organs (17.3%), and malignant neoplasms that were stated or presumed to be primarily of lymphoid, hematopoietic, and related tissue (10.4%). Of the injuries, the most common diagnoses were injuries to the head (28.8%), followed by injuries to the abdomen, lower back, lumbar spine, and pelvis (16.4%), and injuries to the hip and thigh (12.1%). Among the circulatory diseases, the most common diagnoses were CVDs (40.3%), followed by other types of heart disease (18.7%) and ischemic heart diseases (IHDs) (12.7%).
Clinical Outcome Evaluation
The characteristics of teleconsultation in the patients with different diseases and from different wards are displayed in Tables 2 and 3.
Estimated Annual Costs (US $) and Cost Savings of the Telemedicine Model for All Patients
p-Value using a Mann–Whitney U test for continuous variables comparing the differences between the three study groups.
P1: Patients traveled to the hub versus teleconsultation; P2: Specialists traveled to the spoke hospitals versus teleconsultation; P3: Patients traveled to the hub versus specialists traveled to the spoke hospitals.
Note: Values are expressed as mean (range) unless otherwise indicated.
Bold values signify p < 0.05.
Approximately 61.5% of the cases from the emergency room required emergency consultations, whereas for the ICU and ordinary wards, the percentages were 21.2% and 1.4%, respectively (overall p < 0.0001). The majority of emergency consultations were received for patients with injuries (20.2%), followed by circulatory diseases (18.8%), other diseases (12.3%), and neoplasms (6.6%) (overall p < 0.0001).
Of the total consultations, telemedicine resulted in a change of diagnosis in 4,772 (39.8%) patients and varied by disease classification (overall p < 0.0001). The diagnosis change, for the most part, occurred in patients with other diseases (43.0%), followed by circulatory diseases (40.8%), neoplasms (37.5%), and injuries (29.3%). Of the 4,772 cases, 3,707 (77.7%) underwent major changes in diagnosis. Of the definitive diagnoses after teleconsultation, 51.0% (n = 1,891) completely changed into a different subclassification of the ICD-10 system. The remaining 1,816 cases (49.0%) can be grouped in the same ICD-10 system subclassification as the original one; however, their treatment also changed as previously described. The patients suffering from neoplasms, other diseases, injuries, and circulatory diseases each had a percentage of 79.3%, 78.8%, 77.5%, and 68.7%, respectively, in major diagnosis change (overall p < 0.0001) (Fig. 2A). The three most common major diagnosis changes were found in mental disorders (84.6%), diseases of the musculoskeletal system and connective tissue (81.3%), and neoplasms (79.3%) (among diseases with case number over 100). More detailed diagnosis distributions and types of diagnosis changes of mental disorders and the musculoskeletal system and connective tissue diseases are summarized in Table 4.

Diagnosis change, further investigations, and treatment change in the three most common diseases and others.
Estimated Daily Costs (RMB) and Cost Savings of the Telemedicine Model for 100 Patients with Cerebrovascular Diseases
Laboratory investigation includes hematologic test, biochemical test, and immunological tests, etc.
Imaging investigation includes ultrasound, computed tomography, magnetic resonance imaging, and digital subtraction angiography, etc.
Other investigation includes electrophysiological test and vestibular function test, etc.
Western medications primarily include the following: aspirin, clopidogrel, warfarin, and heparin, etc.
TCM medications primarily include the following: San Qi Tong Shu (Chinese patent medicines), Dan Shen, and Deng Zhan Hua Su, etc.
Other costs represent expenses for rehabilitation therapy.
TCM, traditional Chinese medicine.
A total of 3,856 (32.2%) respondents needed to perform one or more than one further investigations. They were requested the most by patients who were diagnosed with neoplasms (35.6%), closely followed by patients with other diseases, diseases of the circulatory system, and injuries, accounting for 35.1%, 29.6%, and 17.4%, respectively (overall p < 0.0001). In those who required further investigations, 2,132 consultants (55.3%) reported that there was a change in the patient's diagnosis, and 1,683 (78.9%) of the 2,132 cases were considered to have major diagnosis change. There was no significant difference in major diagnosis change among the four disease groups (overall p = 0.0614). We classified the types of investigations in major diagnosis change groups and found that 615 (36.5%) cases requested laboratory investigations, 381 (22.6%) patients required imaging examinations, and 277 (16.4%) cases demanded both laboratory and imaging examinations. Other investigation methods were indicated in 411 (24.4%) cases. The patients who were diagnosed with neoplasms (n = 195, 56.9%) required laboratory tests the most, 77.4% of which were pathology tests, whereas the patients with circulatory diseases (n = 81, 53.3%) and injuries (n = 78, 73.6%), for the most part, required imaging tests (Fig. 2B). A total of 8,131 (67.8%) patients were not required to perform further investigations. A total of 2,640 (32.5%) cases had diagnosis changes, and 2,024 of 2,640 cases (76.7%) had major diagnosis changes. The patients with neoplasms (78.3%) had the largest proportion of major diagnosis changes, followed by other diseases (77.8%), injuries (77.7%), and circulatory diseases (66.3%) (overall p = 0.0002).
In general, the treatment plan changed significantly in 6,591 (55.0%) patients as a result of the telemedicine session and varied by specialty (overall p < 0.0001). Injuries accounted for the highest proportion of treatment changes (61.4%) compared with neoplasms, circulatory diseases, and other diseases (57.6%, 48.9%, and 53.6%, respectively). A total of 3,677 (55.8%) treatment changes were not associated with diagnosis change. The patients with injuries (66.5%) had the largest percentage of treatment changes, which were not due to changes in diagnosis, followed by neoplasms (60.1%), circulatory diseases (54.7%), and others (51.4%) (overall p < 0.0001) (Fig. 2C).
With regard to the patients’ next treatment plan, 463 (3.9%) patients were transferred to the hub. More patients (5.0%) with circulatory diseases were transferred compared with those patients with neoplasms (3.9%), other diseases (3.9%), and injuries (2.8%) (p = 0.0314).
Cost Analysis of Telemedicine
The annual mean cost calculations and details of savings for all of the patients are summarized in Table 3. Our analysis showed that the total cost of the telemedicine project in the first year of operation was $16,941 compared with $21,207 when the patients traveled to the hub or $25,160 when the specialists traveled to the spoke hospitals for in-person consultations. In 2013, the telemedicine network cost was $176,243, whereas the cost of the face-to-face healthcare model totaled $803,847 when the patients traveled to the hub or $1,383, 148 when the specialists traveled to the spoke hospitals. On average, the annual telemedicine cost ($74,156) was less than the two types of traditional visit costs, $271,200 if patients traveled to the hub (p = 0.0433) and $387,407 if specialists traveled to the spoke hospitals (p = 0.0209), respectively. The leading expenditures of telemedicine were the running costs of equipment maintenance and staff (p < 0.0001). A mean cost saving of $197,044 or $313,251 was achieved.
Overall, the aggregate cost of the teleconsultation project in a 12-year period was $889,885, whereas the conventional consultation expense was $3,254,410 or $4,648,898, which represents a net saving of $2,364,525 or $3,759,014. Figure 3 shows the trend of the estimated cost savings for all of the patients in the study period. The cost savings in both conditions, which increased year by year, were observed to be stable before 2008. The breakeven point (the threshold at which the teleconsultation costs are equal to face-to-face consultation costs) varied relying on patient numbers, distance, and intricacies of cases. The threshold was reached at a workload of 2,323 or 1,588 consultations in each condition. For sensitivity analysis, see the Appendix in Supplementary Data.
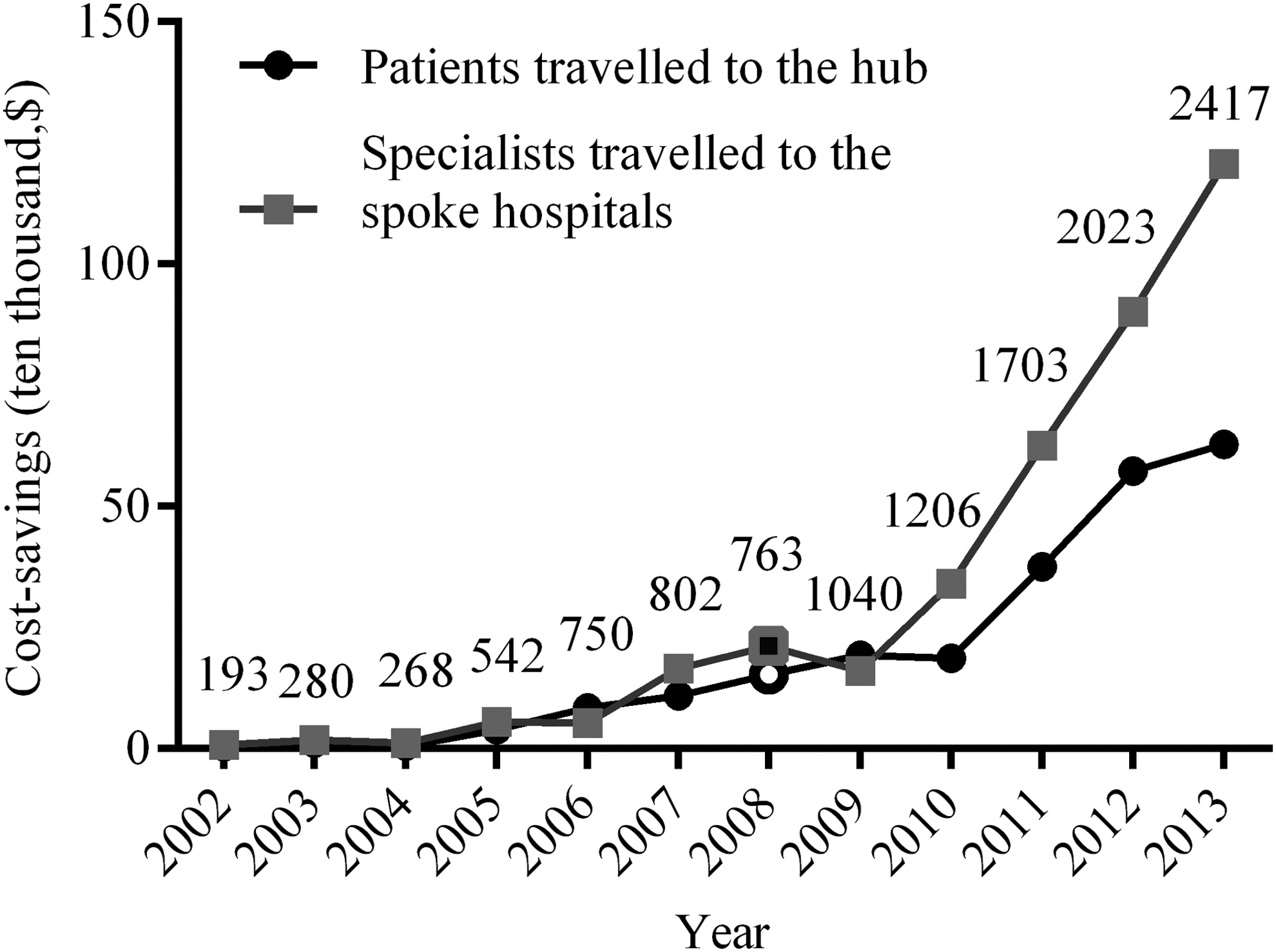
Total cost savings (US $) for all of the patients compared with teleconsultation. The number of patients by calendar year is shown at the top of each gray box.
Table 4 describes the daily cost differences in 100 patients with CVD before and after teleconsultation. The costs of laboratory investigation decreased from ¥27,641 to ¥7,076 or a 74.4% decrease in the postperiod of telemedicine services. Meanwhile, further imaging investigation costs were greater by 1.6 times after teleconsultation. The western medication costs increased by 31.4%, whereas the costs of traditional Chinese medicine decreased by 74.9% due to the neurologists’ opinions. Altogether, the costs of original diagnosis and treatment in the spoke hospitals were ¥90,796 or $13,464, whereas they were ¥162,672 or $23,214 after teleconsultation; that is, the telemedicine model costs increased by 79.2%.
Discussion
This article, which is the first large study of implementation and utilization of the telemedicine program in China, demonstrated that there has been rapid development of telemedicine in undeveloped areas of China in the last 12 years with the incremental number of teleconsultations year by year. These changes may be attributable to the government's emphasis on regional development in the west, particularly in primary public healthcare and the Regional Collaborative Medical Service. The present data demonstrated that the principal participants of telemedicine covered the majority of rural areas in western China, whereby large populations live in remote areas with medical resource deficits and increased burdens of disease.
Given the size and spread of this program, it reflected the general situation of telemedicine practice and application in other parts of the country. The feasibility and effectiveness of telemedicine in our survey were similar to those in developing countries, such as India 9,10 and Brazil, 11 showing that telemedicine is a good tool for making specialist healthcare services available and convenient to patients and their families, as well as consultants. It has a positive overall impact on people's health status and China's medical and health system reform. 23
The diseases observed in our study covered all of the disease classifications in the ICD-10 system. The consultants were able to evaluate patients across a broad spectrum of complex clinical conditions using telemedicine. Neoplasms represented the most common condition, which ranked high and was rapidly increasing in the last 12 years. This phenomenon may be explained by the current epidemiological situation in China 24 that neoplasms constitute the most prevalent disease in recent years and that the symptoms are often atypical, which may cause confusion as well as exhibit a lack of necessary examination equipment to confirm the diagnosis. The government should reinforce training and investment to improve the situation in rural hospitals. Neoplasms were followed by injuries (nearly exclusively traffic related) and circulatory diseases, such as stroke and IHD. The leading risk factors for these diseases included environmental pollution, traffic hazards, hypertension, obesity, and high sodium diets. 24 The distribution of diseases observed by telemedicine indicates the changed health profile in China. Policies for improving the physical environment, road systems, diets, and behaviors that lead to these diseases are required.
While changes in diagnosis and treatment would also occur in in-person evaluations at hubs, the significant changes in diagnosis and management regimens in our study imply benefits of appropriate medical care for the majority of the underserved rural population as a result of telemedicine application. Our study findings are consistent with those of previous studies, which have demonstrated that telemedicine effectively improves diagnostic accuracy and management in clinical care when on-site specialists are unavailable. 25 –29
The patients with mental disorders, diseases of musculoskeletal system and connective tissue, and neoplasms had the largest proportion of major diagnosis changes, which reflected the complexities of cases and diagnostic difficulties. The government should regard these issues as primary targets for telemedical care and should invest more to address substantial unmet needs. For patients with injuries, less treatment change was linked with diagnosis change, which indicated that even when a correct diagnosis was made by a primary care physician, the prescribed therapy was frequently inappropriate. The result is similar to other research findings, 30 which indicated that treatment should be improved by continuing learning and accumulating experiences under the instructions of specialists of the hub.
More than 50.0% of the patients had major changes in diagnosis as a result of performing further investigations. This high proportion indicates that the primary care sites may lack basic integrative medical equipment and technical support for accurate diagnosis. For example, more patients with circulatory diseases than other diseases were transferred to the hub primarily due to the absence of angiography techniques.
We also noted the importance of additional professional knowledge of local doctors. A total of 67.2% of doctors in China have only been educated up to the junior college or secondary school level, and the urban–rural disparities in doctors’ qualifications and training were common across the country. 1 There has been a great improvement in the physicians’ skills because they can accumulate clinical experiences from consulting with experts at the hub. More effective policies will be needed to enhance their professional skills and integral levels. The hub should be more proactive in scheduling online teaching rounds, consultations of difficult cases, and other types of diversified tele-education activities regularly every month to provide access to ongoing medical, educational, and training opportunities for the referring primary care providers.
As for the referral pattern, a relatively small proportion of patients have been transferred to the hub because those with severe and complicated clinical situations are not suitable for transfer. In addition, several spoke hospitals are far away from the hub, that is, 2,974 km for hospitals in Xinjiang. Given the geographical reasons, transportation difficulties, and limited economic conditions, the patients and their doctors may choose to transfer to a superior hospital nearby if needed.
Evidence for the cost-effectiveness of teleconsultation in comparison with the conventional methods of sending patients or specialists for face-to-face appointments is controversial. Studies in the United States 31 –33 and Australia 34,35 have reported that the cost of telemedicine was lower than that of conventional consultations. In contrast, another U.S. telehealth model generated no cost benefit, likely because of the primarily small number of patients studied. 36 Based on our findings, the telemedicine application has proven to decrease the economic burden of patients and their families. Our study included a large number of patients from long distances. The total savings had increased over the years in proportion with the increase in the amount of consultations. A steep rise in cost savings, which started in 2010, may be due to expansion of services after the earthquake, leading to economies of scale.
In the present cost analysis, the threshold was most sensitive to changes in the costs of the patients’ travel, followed by the costs of the coordinators’ salaries and maintenance when the patients traveled to the hub for in-person visits. The costs that had the least impact on the threshold were the registration and consultation fees. The primary contributor to cost savings was the avoidance of travel by the patients and their accompanying family members and specialists. 34,37,38 The transportation savings may vary depending on the distance of the spoke hospitals from the hub. The Chinese health system does not pay for patients’ travel, so this is a saving for the patients. This information is important for planning telemedicine services.
However, the findings may not be generalized to models with lower patient numbers and shorter travel distances. The government can apply net savings in enhancing infrastructures, resources, and service capabilities of remote hospitals. The current findings should be relevant to health service planning in rural areas of China and other countries where vast distances separate patients from adequate healthcare services.
In the longer term, it is conceivable that the wider adoption of the telemedicine system might result in more significant cost savings. For instance, it would provide additional financial benefit to the healthcare system after full inclusion of teleconsultation in the scope of medical insurance reimbursement by the Chinese government. Although the protocols that the experts provided after teleconsultation in CVD might not be cheaper, they were based on the guidelines. The physicians at the spoke sites usually perform some basic checks and the drugs are sometimes used improperly. The new therapeutic strategies after teleconsultation may be more standardized, rational, and suitable for patients. The medical expenses may be increased, but the costs of transportation and the others are greatly reduced, which makes the telemedicine model a cost-saving program in general. Nevertheless, our prior work provides only an estimate of the potential cost-reducing value of telemedicine. Additional evidence from prospective trials and research is warranted.
Response time is an important factor for facilitating rapid identification and intervention for diseases in telemedicine, especially for emergency consultation. In the present study, the average response time (1.6 days) was shorter compared with the results in other studies. 39,40 The response time also varied year by year to some extent. A rapid response time was achieved through the introduction and implementation of standard operational protocols and regular view and feedback of performance. However, certain consultations might require the attention of highly skilled specialists who had very busy work schedules, which occasionally may cause delay. Nonetheless, with a more streamlined process, the overall response time can be shortened to approximately 8 h, according to the military telemedicine program. 41
One solution calls for the hospitals to establish a green channel, especially for cases that present from the emergency room and the ICU. Despite the difficulty of cross-origin resource sharing in China hampering the implementation of a synchronous desk-to-desk consultation, which establishes real-time communication, data transfer between primary doctors and specialists directly is needed. In the management of crisis or emergency state after teleconsultation (e.g., side effects after giving new therapies remotely), even personal digital assistants (smart phones) can be used for data transfer and video calls.
The telemedicine system has several limitations. The total number of consultation events was fewer than those in many developed countries, such as the United States 42 and Portugal, 43 likely because telemedicine in China began comparatively later. The majority of the spoke hospitals were general hospitals, and more specialized hospitals such as psychiatric hospitals should be involved in the program. Moreover, telemedical intervention in our study is used only in inpatient settings, instead of outpatient settings, although it is technically feasible in both situations. 44 With the sustained and rapid development of China's economy, more telemedicine platforms should be constructed in the future to benefit outpatients and patients in the community or at home more widely and conveniently. Besides, expanding the influence and reputation of teleconsultation through propaganda in local communities is of great importance. In this way, the primary care physicians and patients can improve their awareness of telemedical approaches so that the knowledge gap can be bridged and the optional referral can be minimized. Additionally, the TCWCH can be divided into several small subcenters according to different specialties. The quality of equipment and hardware facilities should be improved, as well as the quality of medical records and images transmitted from the spoke hospitals, 45 –47 to avoid distraction and establish effective communication.
On the other hand, the flaws of the study itself should also be addressed. For example, there was selection bias in the study sample. Moreover, this is a pilot cross-sectional descriptive study with no comparison group, which could potentially affect the validity of the study results. Furthermore, it involves various kinds of diseases and the clinical heterogeneity may be one of the disturbing factors. We mainly evaluated the correction of inaccurate diagnosis and inappropriate treatment after teleconsultation in this article. Long-term follow-up regarding prognosis and unintended consequences of the program is needed in the future.
In summary, the present study provided robust evidence concerning the effectiveness and benefits of the telemedicine program, especially in rural regions of China, which shows that such a program is not only feasible and can greatly improve the quality of clinical management of patients but also highly cost-effective. The information generated should be relevant to expanding and further developing similar systems in other regions of China in the future. As a long-term strategy, the government should incorporate telemedicine as an important and critical component of the new medical reform to effectively tackle the large challenges in public healthcare.
Footnotes
Acknowledgments
The authors thank all of the participants in this program for their cooperation; Prof. Zheng-Ming Chen (Clinical Trial Service Unit and Epidemiologic Studies Unit, Nuffield Department of Population Health, University of Oxford) for his internal review of an earlier version of the manuscript and his constructive criticism; and Prof. Zheng-Min Yan (Department of Health Economics, West China School of Public Health, SCU) and Dr. Jin Wen (Clinical Epidemiology and Evidence-Based Medicine Center, West China Hospital, SCU) for providing advice on health economic evaluation. This work was supported, in part, by the National Natural Science Foundation of China (Nos. 81371529 and 81071140), Key Projects in the National Science and Technology Pillar Program during the Eleventh Five-Year Plan Period of China (No.2006BAH02A27), and Postquake Aid Construction Fund from the Hong Kong Government.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.