
Abstract
Introduction
In Japan, catheterization laboratories are available in each medical service area. In contrast, cardiovascular centers capable of cardiac surgery are quite limited. Critically ill patients in rural areas must be transferred to receive advanced medical care. Making optimal treatment decisions is sometimes difficult for the inexperienced physician. Recently, the utility of teleconferencing has been reported in the management of cardiovascular diseases. We have developed a Digital Imaging and Communications in Medicine (DICOM) telemedicine network (Kumamoto telemedicine network) to enable open cardiology conferencing between distant hospitals. The Aso Medical Center is located about 40 km from the nearest cardiovascular center capable of cardiac surgery. The mean time to transfer from Aso to hospitals in Kumamoto is 48 min. We investigated the utility of a teleconference system in this area.
Materials and Methods
The Kumamoto telemedicine network consists of 2 high-volume centers and 12 rural low-volume hospitals without on-site cardiac surgery (Fig. 1). Travel distance between the hospitals and the referral center ranges from 40 to 113 km. The network consists of a central server and multiple clients that can retrieve and display DICOM images. The central server is located in the Kumamoto Central Hospital. All DICOM images were stored losslessly in the digital filing system. The clients' angiographic images were stored in the digital moving image filing system (Nahri AQUA®; Nexis Corp., Fukuoka, Japan). Other DICOM images, including computed tomography (CT) and echocardiography, could also be transmitted. The images were transmitted through broadband connections, such as asymmetrical digital subscriber line (13–18 megabits per second [Mbps]) or optic fiber (100 Mbps) without image compression. Angiographic teleconsultations were performed in the online mode. Patient data were transmitted using a Web-based consultation system (Nexis TASKI System®; Nexis Corp.). Network security was based on a firewall (FirePass® 1230 Remote Access Controller; Fujitsu Corp., Tokyo, Japan) and a virtual private network (network service: FLET'S VPN WIDE; NTT WEST Corp., Osaka, Japan; router: YAMAHA® RTX1200; YAMAHA Corp., Hamamatsu, Japan).

Kumamoto telemedicine network. The Kumamoto telemedicine network consists of 2 high-volume centers and 12 rural low-volume hospitals. The central server is located at the high-volume center in Kumamoto. The network provides secure Internet communication with SSL-VPN technology. SSL-VPN, secure sockets layer virtual private network.
Aso is a small rural city with a population of ∼30,000. More than 30% of the population is older than 65 years. The Aso Medical Center is the only low-volume hospital, where a cardiologist works regularly. We retrospectively examined the cardiology consultation cases in the Aso area before and after the telenetwork era. The waiting period for transfer from the Aso area to high-volume centers before the implementation of telemedicine was compared to that after the implementation of telemedicine.
All data were expressed as mean ± standard deviation. For the statistical analysis, the prevalence of patients transferred to high-volume centers was compared by chi-square test between the telemedicine era and the pre-telemedicine era. Waiting periods were compared by an unpaired t test. Values of p < 0.05 were considered to be statistically significant.
Results
Between January 2010 and December 2014, a total of 293 teleconferences were conducted in the network (Table 1). The mean patient age was 71 ± 12 years. At the Aso Medical Center, teleconferences started in June 2012. We investigated the prevalence of patient transfer from the Aso Medical Center to high-volume centers before and after network system deployment. Between June 2012 and December 2014, teleconferences were carried out in 48 cases (30 coronary artery disease, 6 peripheral artery disease, 3 aortic aneurysm, 3 deep vein thrombosis, 2 inflammatory aortitis, 1 annuloaortic ectasia, 1 cardiac tamponade, 1 myocarditis, and 1 heart failure). A successful communication connection was obtained in all cases. In the pre-telemedicine era (from April 2010 to May 2012), 10 of 18 patients with cardiovascular disease diagnosed by imaging modality were transferred to high-volume centers to get a second opinion. After the initiation of the teleconferences, 10 of 48 patients were transferred to the high-volume center (Table 2). Telemedicine-based collaborative care significantly decreased the frequency of patient transfer from the Aso area (p < 0.05). The waiting period did not significantly change after the implementation of telemedicine (9.2 ± 6.9 vs. 17.2 ± 19.2 days, p = 0.23).
Overview of the Kumamoto Telemedicine Network Participating Hospitals
Clinical Characteristics of Patients Transferred to High-Volume Centers
Case Presentations
Case 1
A 59-year-old man presented to a medical clinic with a low-grade fever for 10 days. Oral antibiotic treatment for a bacterial infection did not reduce the fever. The patient complained of intermittent abdominal pain. The patient was referred to the Aso Medical Center for further evaluation. Laboratory examination revealed a normal white blood cell count (7,470/mm3 with 72% neutrophils) and elevated serum levels of C-reactive protein (7.0 mg/dL). Abdominal enhanced CT showed a crescent of soft tissue density in the anterior wall of the abdominal artery. Teleconferencing was performed between the Aso Medical Center and Kumamoto Central Hospital. With the probable diagnosis of inflammatory aortitis, intravenous antibiotics were started after taking blood cultures. Follow-up CT examination revealed an aneurysmal change of the aorta. After the second teleconference, the patient was transferred to the Kumamoto Central Hospital for surgical treatment (Fig. 2).
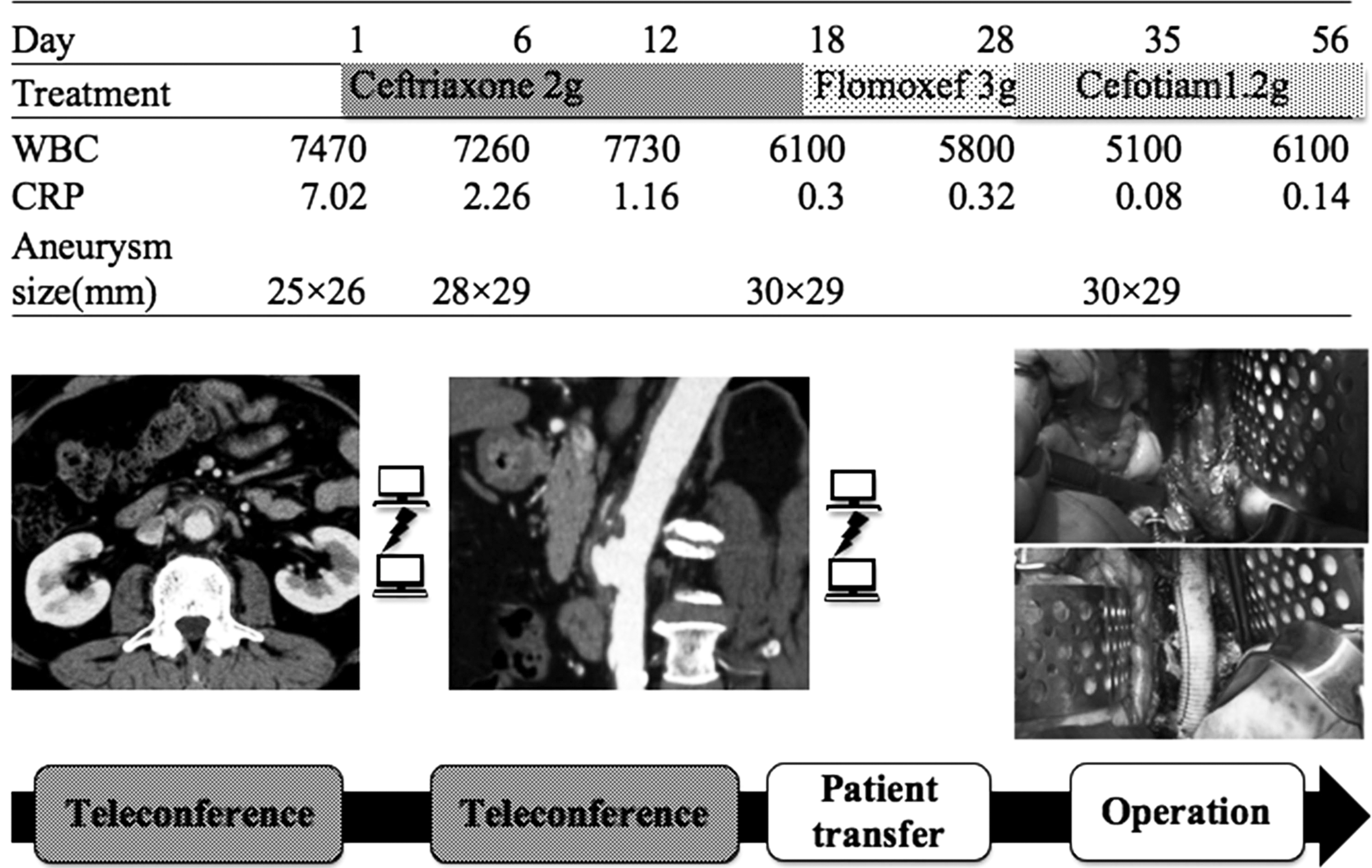
Clinical course of the patient with inflammatory aortitis. Axial contrast-enhanced CT showed a normal-caliber abdominal artery. Thickening of the aortic wall and periaortic soft tissue density were also observed. Despite antibiotic therapy, follow-up CT showed an expanding aortic aneurysm. After the second teleconference, the patient was transferred to the high-volume center. CT, computed tomography.
Case 2
A 75-year-old man was admitted to the Aso Medical Center for exertional angina. Coronary CT revealed severe organic stenosis in the left circumflex coronary artery (LCx). Optimal medical treatment, including beta-blockade, did not relieve the chest discomfort with exertion. After the teleconference, the patient was transferred to the Kumamoto Central Hospital for percutaneous coronary intervention (PCI). Coronary angiography showed a chronic total occlusion of the LCx, where a coronary stent was implanted. The length of hospital stay for PCI was 3 days. Nine months after PCI, follow-up coronary CT revealed patency of the coronary stent and a progressive atherosclerotic lesion in the right coronary artery. The patient did not have angina. A stress test was negative for ischemia. As a result of the teleconference, the patient was not transferred. Periodic follow-up examinations have been performed at the Aso Medical Center.
Discussion
In Japan, teleradiology developed dramatically in the 1990s. 1 Travel to distant urban hospitals is sometimes difficult for elderly people living in rural areas due to concerns about traffic and physical and economic considerations. Development of a telemedicine network is one of the important subjects in anticipation of a coming super aging society. Our study demonstrates the utility of a telemedicine network for facilitating appropriate transfers of patients with cardiovascular diseases living in rural areas.
In recent years, the concept of a heart team has been proposed for the treatment of cardiovascular diseases. 2 A multidisciplinary heart team has been strongly recommended in the European, American, and Japanese guidelines on myocardial revascularization. 3 –5 Akasaka et al. reported that there is no significant difference in the clinical outcomes following PCI procedures between hospitals with or without on-site cardiac surgery in Japan. 6 However, formation of an ideal heart team is quite difficult in rural areas because of a shortage of medical providers. Teleconferencing has the potential to provide optimal medical treatment comparable to heart teams. 7 –12 While not statistically significant, the waiting period tended to be extended after the implementation of telemedicine. Increased use of nonemergency medical transportation might have contributed to the extension of the waiting period.
The cost-effectiveness of telemedicine remains controversial. 13 –15 The initial and running cost of a telemedicine network is an important concern. Sharing information is useful to avoid unnecessary duplicate examinations. Pre-examination of data contributes to shortening of the hospital stay. Overutilization of myocardial revascularization therapy is precluded by the use of a multidisciplinary teleconference. Electrocardiogram, echocardiography, and biochemical examination of blood were routinely performed in patients transferred to high-volume centers. In Japan, these examinations cost about $180 in total. Reducing unnecessary transfers to high-volume centers can directly suppress the cost by limiting these examinations. In these respects, a telemedicine network might suppress the total medical expense. As to our study's limitations, we could not perform a prospective study to evaluate the effectiveness of telemedicine, and the sample size was too small to make a definitive conclusion. A prospective study is needed in the future to confirm the cost-effectiveness of telemedicine.
Angiographic telemedicine has been tried for about 20 years. Image quality was insufficient for clinical study. In a DICOM network, lossless images are accumulated in the central server. These data can be analyzed exactly. Thus, a network system might facilitate multicenter clinical research using the DICOM images.
Conclusions
Teleconference is a useful tool for making decisions for appropriate treatment. The Kumamoto telemedicine network enables a close relationship between high-volume centers and rural hospitals. This collaboration has the potential to improve cardiac care in rural areas.
Footnotes
Acknowledgments
Coinvestigators of Kumamoto telemedicine network are as follows: Kumamoto University: Kenichi Tsujita and Seiji Hokimoto, Kumamoto Central Hospital: Hitoshi Sumida and Katsuo Noda, Sakanashi Heart Clinic: Toshihiko Sakanashi, Arao Municipal Hospital: Ichiro Kajiwara, Hitoyoshi Medical Center: Shinichi Nakamura and Hideki Oka, Tamana Central Hospital: Kenichi Komori, Yamaga Medical Center: Masaya Fukuda and Keisuke Ohba, Amakusa Medical Center: Seiji Sakaino, Kumamoto Saishunso National Hospital: Ikuo Misumi, Izumi Regional Medical Center: Shigenobu Tateishi, Gokase Town Hospital: Tomoki Okazaki, Minamata City General Hospital and Medical Center: Hideki Maruyama, and Bethesda Clinic: Hiroshi Kugimiya. We thank Kazuyoshi Murayama for network system operation. We thank Yasuhiro Nagano and Yoshio Yamabe (Yamabe Power Studio) for their important contributions to the illustration.
Disclosure Statement
No competing financial interests exist.