
Abstract
Introduction
Balance and posture can be affected in various pathologies such as Parkinson disease, brain stroke, and the elderly. 1 Reduced balance increases the risk of falls with all the consequences that it entails (morbidity, mortality, and cost for social security). Balance training is an important part of the rehabilitation to avoid the above-mentioned complications. 2 To first assess patients and, subsequently, to quantify the patient's evolution, two options are possible as follows: quantitative evaluation of balance using force plate (FP) in a laboratory 3 or a qualitative evaluation using scales such as the Berg Balance Scale. 4 Both approaches have advantages and disadvantages. Quantitative evaluation is very accurate, but access to this kind of tool is limited to specially-equipped laboratories and does not allow regular measurement for patient follow-up or evaluation.
Qualitative evaluation is easy to perform and does not require any material. Despite the fact that these scales have been validated for various neurological conditions, 5 they are not sensitive enough to detect small clinically relevant changes. 4 Since a few years, the idea of integrating video games in rehabilitation of various pathologies such as brain stroke, 6 cerebral palsy, 7 Parkinson disease, 8 and elderly 9 has emerged. These games are played with the console, and therefore, there is no way to record or control what the patients are really doing. Specially developed video serious gaming (SG) centered around rehabilitation exercises using Wii Balance Board™ (WBB) as controllers has been previously developed. 10 Center of pressure (CP) displacements are recorded during these rehabilitation exercises for later analysis.
Currently, although several studies have shown good results for balance assessment during static conditions (e.g., Romberg test 11,12 ), for force estimation 13 and the fact that posture assessment performed with several WBB gave similar results, 14 the use of the WBB as a tool for clinical assessment remains controversial. 15,16
In the clinics, WBB has been used to assess patients suffering from various diseases such as Parkinson's disease 17 or other conditions as for instance anterior cruciate ligament injuries, 18 and with elderly patients. 19,20 However, to our best knowledge, there is currently no study on the use of WBB to assess balance during dynamic SG exercises. Therefore, the aim of this study was to validate the use of WBB to assess CP displacement during rehabilitation exercises.
Materials and Methods
Participants
Thirty five young healthy adults (age = 25 [3] years, height = 174 [11] cm, weight = 65 [13] kg, 14 females) participated in this study. This study was approved by the Ethics Committee of the Erasme Hospital (CCB: B406201318023), and written informed consent was obtained from all subjects before their participation. No participants presented any neurological or orthopedic disorders and none of the subjects was taking medication at the time of the study that may have influenced balance or posture.
Procedures
A WBB (size 45 × 26.5 cm) was placed on the top of FP (size 50 × 46 cm; AMTI model OR6-6, Watertown, MA) that was embedded within the laboratory floor. This setting allows simultaneous measurement with the FP and the WBB. The WBB was connected to a laptop (Intel Core I5, Windows 7, 6 GB RAM) through Bluetooth connection; data were retrieved using a custom-written software based on the WiimoteLib software 21 during the SG. WBB and FP data collection frequency were 100 and 1,000 Hz, respectively. The FP was calibrated before measurement. For the WBB, no calibration procedure was used although some methods have been proposed in the literature. 11,12,17 –19 Such calibration-free methodology was adopted because one of the purposes of this study was to evaluate the clinical WBB usability without the practical constraint of systematic calibration.
Participants played two mini-games: the Flight Simulator (Fig. 1A), in which the player has to control a plane by displacing (mainly mediolateral) CP to collect stars and avoid rocks, and the Wipe Out (Fig. 1B), in which the player has to clean the screen covered of mud using a tissue controlled by CP mediolateral and anterior–posterior displacements.
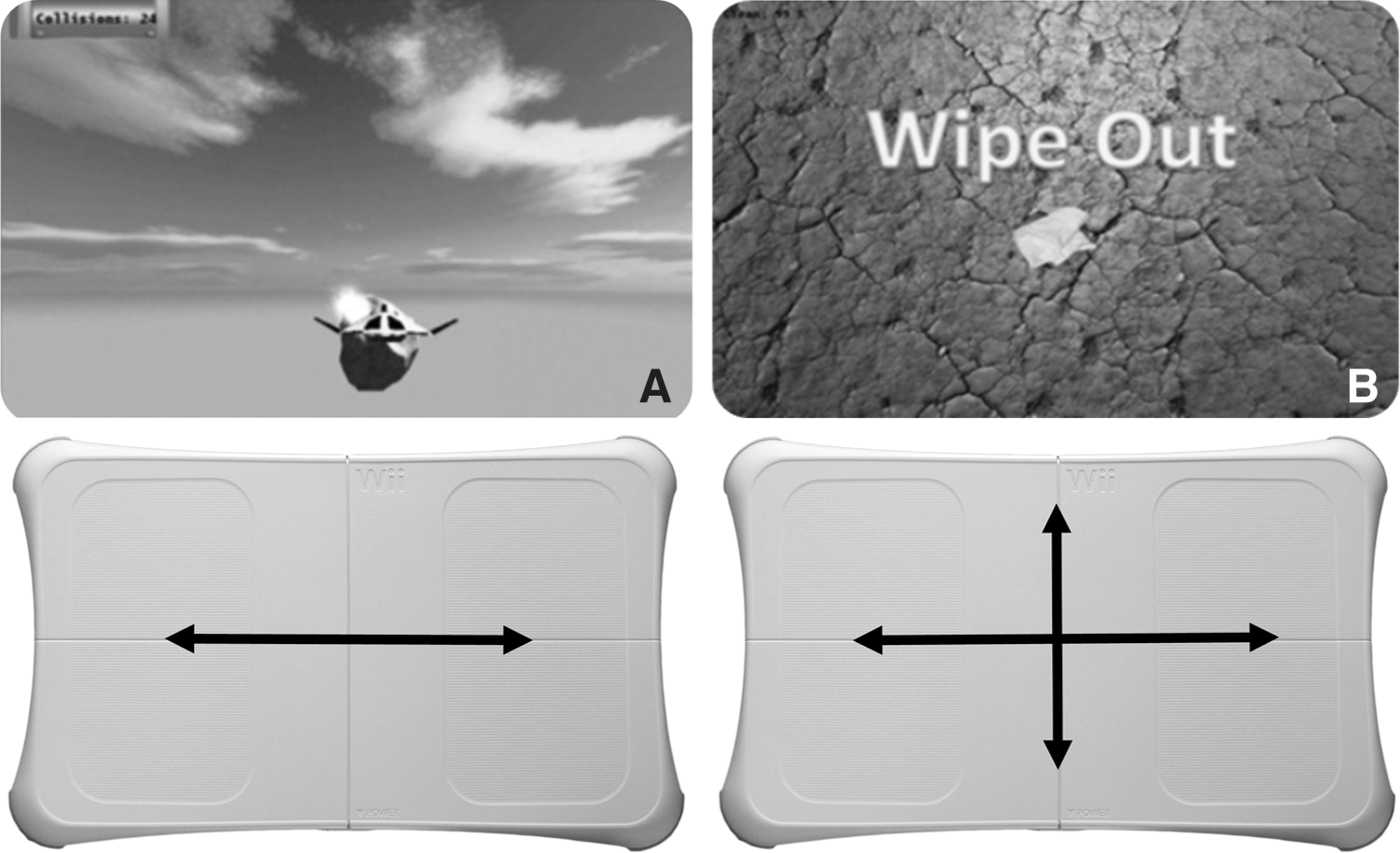
Illustrations of the serious gaming used in this study.
Data Processing
Based on CP, displacements recorded during SG in total 9 variables were processed using a custom-made MATLAB code (The Mathworks, Natick, RI).
22
Previous works have shown that the time interval between samples of WBB was inconsistent;
12
therefore, linear interpolation of the raw signals of WBB sensors was applied to get a regular sample rate of 1,000 Hz.
23
Both data from WBB and FP were then filtered using a second-order Butterworth low-pass filter with a cutoff frequency of 12 Hz.
11,12
For WBB, CP an anterior–posterior (CP AP) and mediolateral (CP ML) displacements were obtained from the four strain gauge loads located at the four corners of the plate using equations (1) and (2), respectively:
where PL, PR, FL, and FR are the displacement values from the posterior left, posterior right, front left, and front right WBB sensors, respectively. 11
For FP, CP AP and CP ML displacements were obtained using equations (3) and (4), respectively
24
:
where H is the height between the FP and the surface of the foot of the subjects (in cm), Fx, Fy, and Fz are force, and Mx and My are torque projections, respectively.
Most of the articles comparing WBB and FP are only focusing on the total length of CP displacement during the trial 11 –17 to analyze balance instability. In this article, a wider range of variables that were identified as relevant balance outcomes were processed from the available CP data 25 : - the total displacement of sway (DOT); - the area of the 95% prediction ellipse (often referred to as the 95% confidence ellipse 26,27 ) (Area); - the dispersion of CP displacement from the mean position (SD AP and SD ML); - the distance between the maximum and minimum CP displacement (AdCP AP and AdCP ML); - the mean velocity of CP displacement (MV AP and MV ML); - and the AP and ML displacements of the total CP sway divided by the total duration of the trial (TMV). Although all these outcomes are computed based on the COP coordinates, the agreement between WBB and FP must be studied for each variable.
Statistical Analyses
All dependent variables were normally distributed (Kolmogorov–Smirnov test); therefore, parametric tests were applied. For every parameter, Pearson's correlation coefficients (R), equations of the regression lines, and two-tailed paired-sample t test were computed. Since there is no consensus in the literature about the use of correlation coefficients or intraclass correlation coefficient (ICC) to assess agreement between both devices, ICC (Two-way mixed average measures) was also computed and presented. The agreement between both devices was examined using limits of agreement (LOA) with Bland and Altman (B&A) plots. 28 All statistical analyses were conducted using MATLAB.
Results
Table 1 (Part 1 and 2) presents the mean results and statistics (R, ICC, t test, and LOA) of the variables for the two games and Part 3 presents the mean results for both games. Linear regression equations and correlations are presented in Figure 2 (mean results of the two games). Bland & Altman plots are presented in Figure 3 (mean of the two games). For each parameter, highly significant differences were found for both games, but excellent correlations were obtained (mean R = 0.95 and 0.96 for Flight Simulator and Wipe Out, respectively). Concerning the values obtained during the two different games, same values were obtained in the mediolateral directions (250 and 280 mm for the WBB, 244 and 296 mm for the FP, for Flight Simulator and Wipe Out, respectively). The anterior–posterior displacement values were much higher for the Wipe Out games (71 and 188 mm for the WBB, 61 and 191 mm for the FP, for Flight Simulator and Wipe Out, respectively).
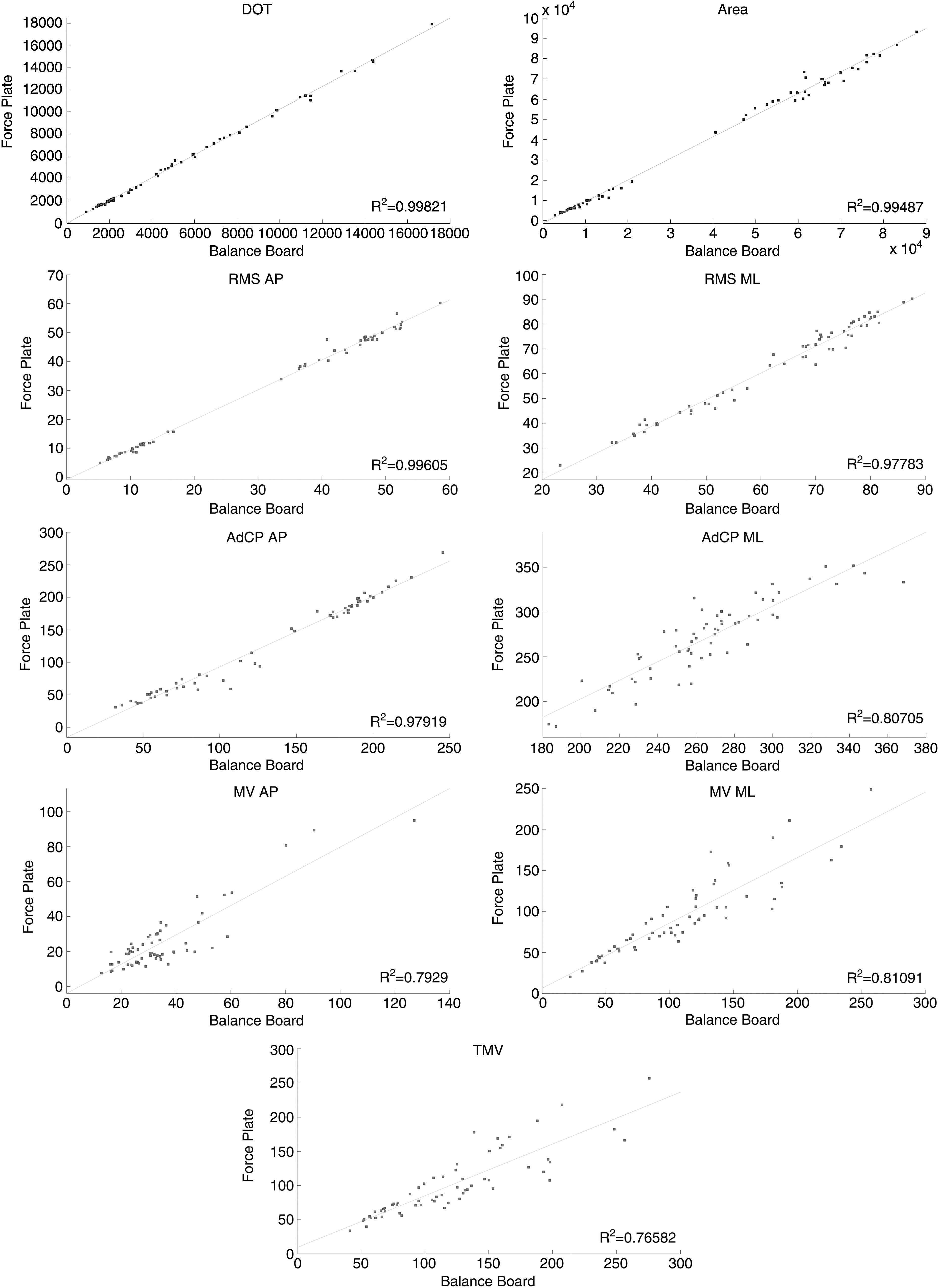
Scatter plots, correlation lines, and equations for the nine different balance variables obtained during the Flight Simulator game.
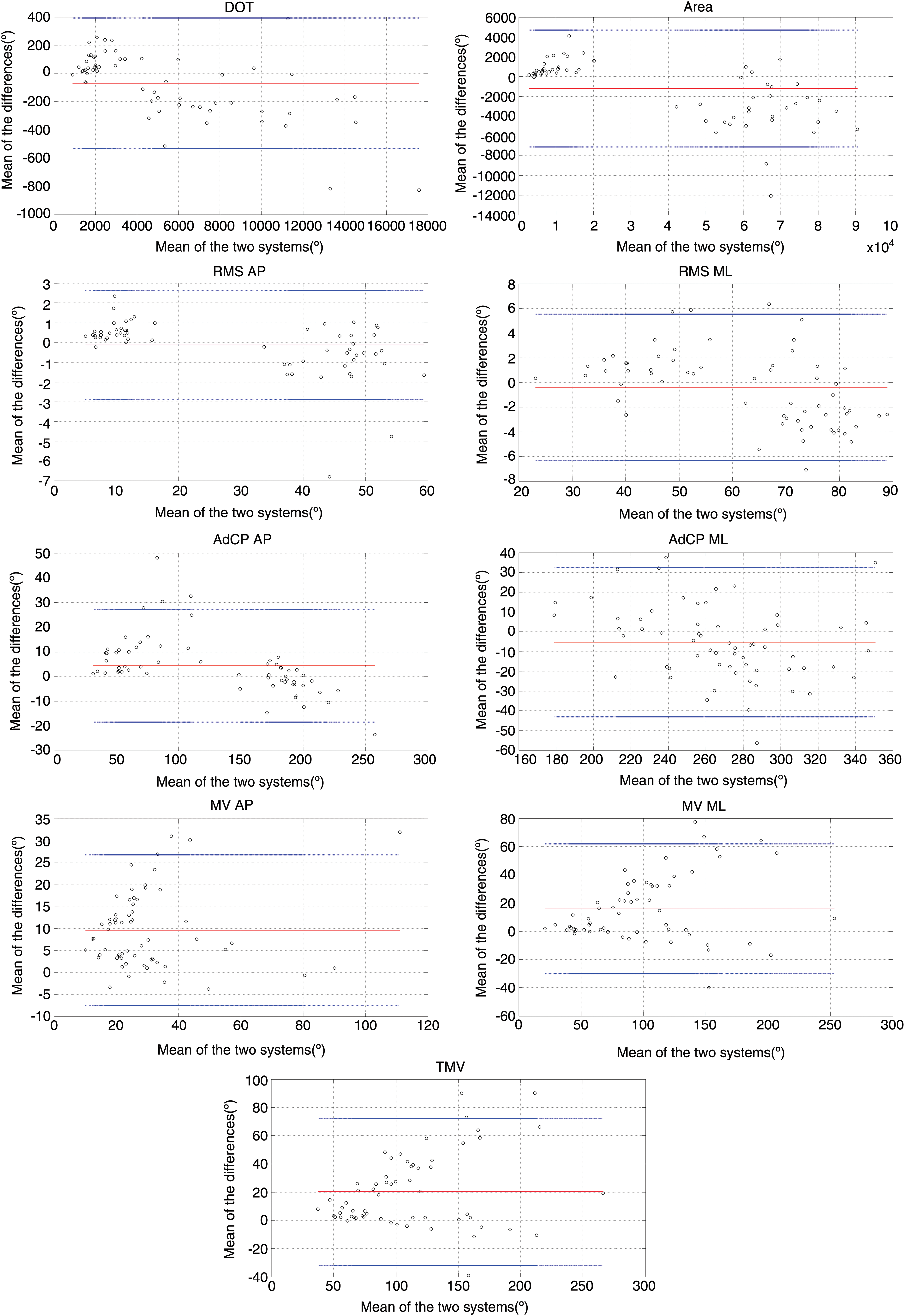
Bland & Altman plots for studied variables for the Flight Simulator game. Red lines (middle one) represent the mean difference between the devices. Blue lines (extremities) indicate upper and lower agreements (2SD). Color image is available online at
Mean (std) Results for the Two Games
FP, force plate; ICC, intraclass correlation coefficient; LOA, limits of agreement; R, Pearson's correlation coefficient; WBB, Wii Balance Board™.
Discussion
This is the first study comparing WBB and FP during games (dynamic balance) and the first to focus on a broad range of balance outcomes used in clinics. Results are therefore difficult to compare. However, our results can be compared with previous studies concerning CP path length (DOT). Some results for WBB-based balance assessment during static conditions might well be inferior to some traditional FP. 15,16 That is mainly caused by the fact that a WBB is less sensitive than the golden standards. According to the International Society for Posture and Gait Research, a device that measures posture should have the following specifications for time functions (X = x(t) and Y = y(t)): accuracy better than 0.1 mm, precision better than 0.05 mm, and a resolution higher than 0.05 mm. 29 These values have been adopted for balance assessment in the static condition.
This study is focusing on the use of WBB, but both static 30 and dynamic 31 balance can also be assessed using the Kinect™ sensor. However, this sensor is less sensitive to track CP displacement. The WBB can detect smaller CP displacement and is, therefore, more adapted for balance assessment and rehabilitation by allowing proprioceptive feedback.
The current study assesses balance in dynamic conditions (SG), in which subjects are stimulated by the game to move toward the edges of their base of support. Therefore, the range for CP displacement is much larger, and the sensitivity of the WBB is probably far less an issue. We also found almost perfect correspondence (R = 0.99, ICC = 0.99 [0.99;1]) between results obtained with WBB and FP. 11,12,17 The aim of this study was to determine whether or not differences between CP signals have influences on the variables used in clinics instead of trying to find a perfect correspondence between the CP signals. Therefore, in addition to DOT, 8 variables that are clinically relevant for posture analysis were computed.
According to the literature, ∼40 parameters can be derived from CP, including the mean velocity that is considered as the variable offering the highest reliability among different trials. 21 Another FP-based study underlined the importance of the speed by reporting that peak velocity showed the highest reliability. 32 Concerning the speed variables derived from CP displacement, good correlations were found for the anterior–posterior speed (R = 0.84 and 0.99 for the Flight Simulator and the Wipe Out, respectively), the mediolateral (R = 0.95 and 0.99 for the Flight Simulator and the Wipe Out, respectively), and for the TMV (R = 0.94 and 0.99 for the Flight Simulator and the Wipe Out, respectively). The global results are a bit lower for speed parameters (R = 0.89, 0.90, and 0.88 for MV AP, MV ML, and TMV, respectively). Scatter plots and B&A plots show that there seem to be two different clouds of points for speed-related parameters (Figs. 2 and 3).
In Figure 4, results of the two games were separately plotted to check whether or not there are differences and it appears that the regression lines and the coefficients of determination are not the same for the two different exercises. These results are suggesting that the WBB could be used to assess these parameters related to velocity of CP displacement that are more sensible to compare different age groups or different health conditions. 33 However, it is important to note here that speed-related parameters obtained with the WBB seem to be sensitive to the kind of exercises performed. Indeed, for the Flight Simulator, a difference of 15(7) mm/s was found for the anterior–posterior displacement (i.e., this displacement is supposed to be minimal) with an overestimation of the WBB. Results of agreements were lower for this parameter (R = 0.84, ICC = 0.77 [0.52;0.89]). This trend was not found for AP displacement.
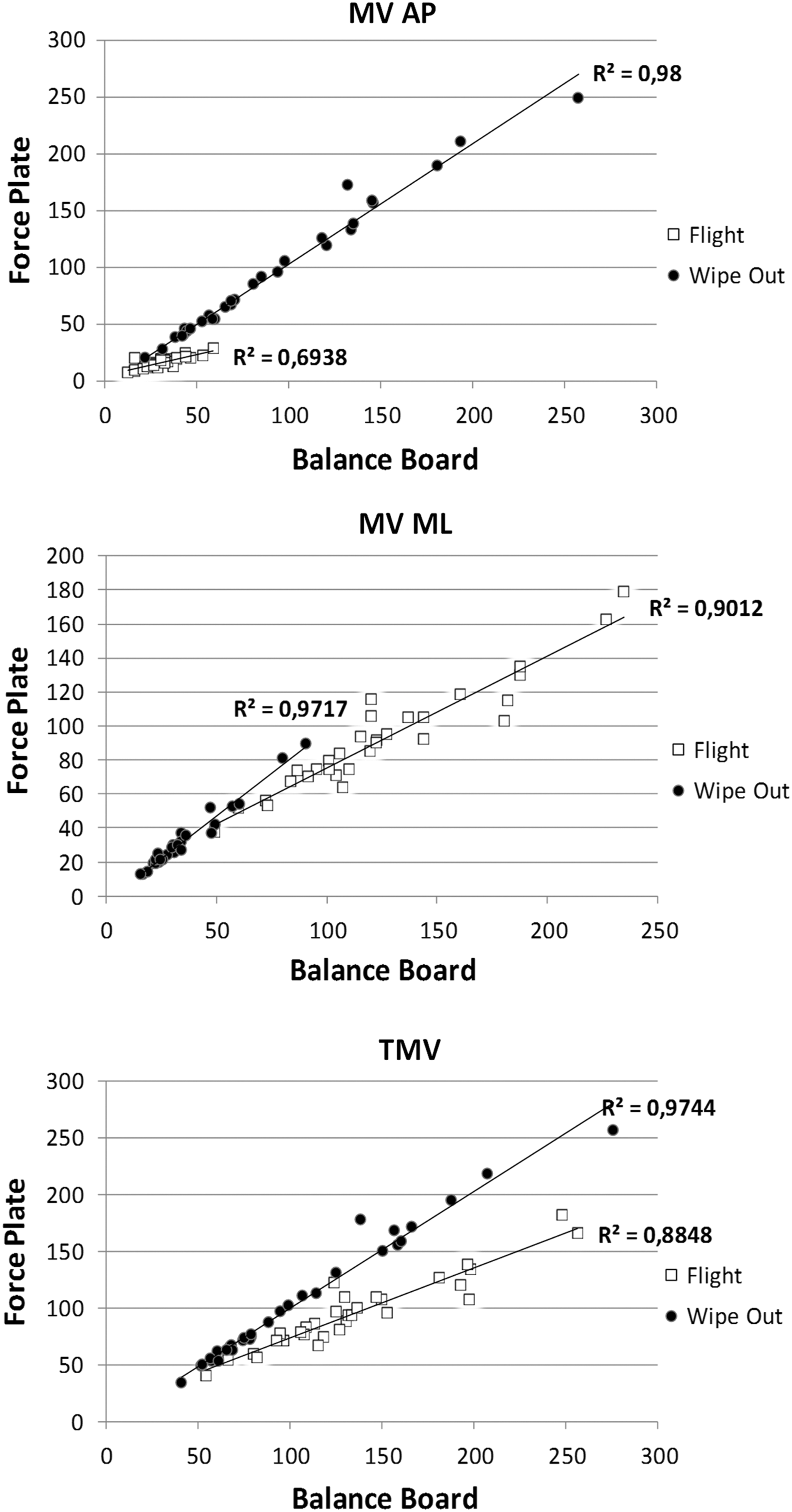
Scatter plots, correlation lines, and equations for the three different parameters related to velocity of CP displacement, the two games are presented separately. White squares are used for Flight Simulator and black circles for Wipe Out.
Unlike the other previous studies, no calibration procedure was used before measurements. However, results were highly correlated using the WBB data directly without any calibration step. This approach is hence more user-friendly compared to an approach where a calibration procedure is required and could therefore be easily used in private practice or installed in patient's home. Results of this study open up new possibilities in the field of rehabilitation and patient's follow-up. Further work is needed to get a better understanding of the possibility of the use of WBB coupled to SG rehabilitation exercises. Are the results obtained stable and reproducible over time if the status of patient is stable? Are the results obtained correlated to the severity of the disease? Is the method sensitive enough to detect modification in the status of the patient? From a clinical and rehabilitation point of view, more works are also needed to not only determine if the games are efficient for the patients but also to determine: which patients (age group, pathology) are most likely to receive such kind of treatment and have favorable outcomes? How many sessions are needed? What is the best duration of these sessions? Clinical studies are currently running to assess if those games can be used to increase balance and posture in patients (e.g., children with cerebral palsy, elderly patients, or patients with chronic obstructive pulmonary disease).
In conclusion, this study confirms the good results previously presented of the WBB compared to gold standard laboratory FP. This study provides relevant additional data. The first aspect is that it is not required to perform any calibration procedure before using the WBB to assess balance during dynamic exercises. The WBB provides comparable data for displacements and velocities derived from CP during SG. Therefore, the WBB coupled with rehabilitation exercises could be used to assess and to follow in a quick and inexpensive way the patients' evolution using a new paradigm in revalidation. Indeed, all the data collected during the rehabilitation exercises could be used to regularly monitor the status of the patients and to adapt and configure those exercises to the actual physical abilities of the patients. Therefore, the exercises would be more effective since they are specially configured and adapted to the functional abilities of the day.
Footnotes
Acknowledgment
This study is a part of the ICT4Rehab and RehabGoesHome projects (
Disclosure Statement
No competing financial interests exist.