
Abstract
Introduction
Depression is highly prevalent among individuals with diabetes, 1,2 and more than half may experience less severe depression symptoms. 3 Depression is associated with suboptimal diabetes self-management behaviors such as lower glucose self-monitoring 4,5 as well as with adverse clinical outcomes, including nephropathy, retinopathy, hospitalization, and death. 6 –10 Nearly one in ten people in the United States (U.S.) have diabetes, 11 suggesting that widely disseminated programs effective to reduce psychological distress in diabetes patients could have significant public health impact. Moreover, studies suggest that diabetes paired with a comorbid mental health condition is associated with significantly increased cost of care. 12
Telehealth is a mechanism with the potential to reach the large diverse U.S. diabetes patient population. 13 Although traditional therapeutic strategies have been demonstrated effective to improve depressive symptoms among people with diabetes, 14 –16 less is known about the impact of telehealth-delivered behavioral health interventions to improve mental health and diabetes self-management.
The purpose of this study was to evaluate the feasibility and potential impact of a tele-behavioral healthcare program uniquely designed to treat comorbid behavioral health issues associated with diabetes to change participant depression, anxiety, and stress measures. Secondary aims were to (1) determine whether the degree of change in depression, anxiety, or stress scores varied by participant demographic or clinical characteristics and (2) evaluate changes in glucose self-monitoring frequency and glucose levels from program initiation to graduation.
Materials and Methods
Study Design and Participants
AbilTo is a digital healthcare provider that offers behavioral healthcare services through telephone and secure video to patients across the United States. Populations served include individuals with chronic medical conditions, sudden medical events, or difficult life transitions. This was a retrospective study of deidentified records from 466 consecutive AbilTo diabetes program graduates who enrolled in the program during a 6-month period between August 1, 2014, and January 31, 2015.
Persons were eligible to enroll in the diabetes program if they had a documented diagnosis of having diabetes mellitus in combination with a recent change in medical status, such as an acute event (e.g., hospitalization) or a new medication regimen. Persons with the following criteria were ineligible for enrollment and redirected for clinical consultation and referral: (1) suicide attempt in the past 3 years, (2) psychiatric hospitalization in the past year, (3) current suicidal ideation or nonsuicidal self-injury, (4) bipolar disorder, symptomatic in the past year or not medication stable, (5) severe substance abuse disorder, substance intoxication or withdrawal, or high score on substance use disorder assessment, (6) psychotic symptoms, (7) borderline intellectual functioning; major neurocognitive disorder, (8) domestic violence or homicidal ideation, and (9) end-stage illness. Among 778 persons who completed their first therapy visit, 549 (71%) remained enrolled for at least half way through the program and 494 (63%) graduated (Supplementary Figure S1; Supplementary Data are available online at
Program Description
AbilTo's diabetes program was specifically designed to help individuals with diabetes understand and better manage depressive symptoms in support of medical compliance and positive lifestyle changes. The program was developed using evidence-based approaches and behavior change tools, including cognitive behavioral therapy, acceptance and commitment therapy, mindfulness, and motivational interviewing, and clinical guidelines to reduce depression, anxiety, and stress and to improve self-management and outcomes among people living with diabetes. The program was designed by the AbilTo clinical team in collaboration with an interdisciplinary advisory group of neuropsychology, clinical psychology, clinical social work, and other medical professionals.
Program delivery occurred through telephone or secure video based on participant preference. The program was administered by a care team, which was made up of a behavioral health provider (licensed clinical social worker or equivalent [LCSW]) and a behavioral coach. Care teams received standardized Association of Social Work Board-certified training provided by AbilTo to ensure consistent and quality delivery of AbilTo's best practice diabetes program protocol.
The AbilTo diabetes program comprised an initial consultation and 15 sessions completed within an ∼8-week period. The initial consultation included a baseline interview and was conducted by an LCSW on the care team. The initial consultation was followed by eight sessions with an LCSW and seven sessions with a behavioral coach. During the course of the program, the LCSW and the behavioral coach participated in case conferences under the guidance of an LCSW clinical supervisor to review participant progress. The clinical supervisor also reviewed session notes on a weekly basis to ensure high quality and adherence to the treatment protocol. The protocol comprised modules targeted to specific skills and tailored to the individual participants' needs and goals, drawing from the principles of cognitive behavioral therapy and other evidence-based behavioral health intervention strategies.
The telehealth program protocol was delivered through a customized technology platform. This platform ensured consistent program delivery using a proprietary content management system, which provided a secure system in compliance with HIPAA to allow sharing of session notes among the LCSW, behavioral coach, and the clinical supervisor. Through the platform, the national network of providers had direct access to standardized protocols and online forms to be used to guide each session. Providers also used the platform to input session notes into a protected electronic record, schedule next sessions, and securely message participants.
Measures
Participant characteristics, including age (years), sex, U.S. region (west, mid-America, southeast, and northeast), past medical history (cardiac, endocrine, gastrointestinal, gynecological, hepatic, pulmonary, neurological, nutritional, renal, or sexual disease/disorder; history of major surgery, trauma, or tuberculosis), and psychological health history (depression, anxiety), were self-reported and systematically documented by the LCSW on the care team immediately before program initiation as part of the initial consultation.
The primary outcome was change in the severity of depression, anxiety, and stress measures from baseline to program graduation. Depression, anxiety, and stress were measured using the Depression Anxiety Stress Scale 21 (DASS-21). 17 The DASS-21 has been validated to assess depression, anxiety, and stress symptoms in diverse populations. 18 –20 The DASS-21 contains seven items each to measure depression, anxiety, and stress for a total of 21 items. For each item, participants were asked to use a 4-point frequency scale to rate the extent to which they experienced the item over the past week (0 = never; 1 = sometimes; 2 = often; 3 = almost always). Depression, anxiety, and stress scale (DASS) scores were calculated by first summing the points for each individual scale score, then multiplying by a factor of two. Non-normal is defined as a depression scale score >9 points, an anxiety scale score >7 points, or a stress scale score >14 points. 17,21 Non-normal DASS scores were further categorized as mild, moderate, severe, or extremely severe based on established guidelines. 22 The DASS-21 was administered immediately before program initiation at the initial consultation and was repeated at program graduation by an LCSW on the care team.
Secondary outcome measures included (1) change in adherence to morning glucose self-testing (self-testing and documenting at least once weekly) and (2) change in morning blood glucose level (weekly average of morning glucose readings recorded by the participant using a point-of-care monitor; mg/dL) from program week 1 to graduation. These data were systematically collected by the care team during week 1 and graduation sessions.
Statistical Analyses
Descriptive statistics were used to illustrate characteristics of the study population, the proportion of participants in each DASS category at baseline and at graduation, and the proportion of participants testing morning glucose level at baseline and at graduation. A comorbidity score was calculated by summing the total number of comorbid conditions (of a total of 14); this score was dichotomized at the median (>2 vs. ≤2). Changes in DASS scores for depression, anxiety, and stress, as well as change in mean morning glucose value, were calculated (1) as the absolute difference in value at graduation versus baseline and (2) as the percent change in value from baseline to graduation.
Single-arm paired t-tests were used to evaluate change in (1) DASS scores and (2) morning glucose levels from baseline to graduation. Univariate associations between participant characteristics and changes in DASS scores and morning glucose levels were examined using generalized linear regression models. Chi-square tests were used to evaluate differences in the proportion of participants who were testing morning glucose at baseline versus graduation and the associations between above normal (≥100 mg/dL) and high (≥mean) glucose levels and DASS score category (non-normal vs. normal).
Analyses were completed using SAS statistical software (version 9.4; SAS Institute Carey). Statistical tests were two-sided with alpha set at 0.05.
Results
Baseline Characteristics of Diabetes Program Participants
Demographic and clinical characteristics of program participants are presented in Table 1. More than half of participants were over 55 years old and 44% were male. Participant location varied by U.S. region; the fewest (16%) were from mid-America (p = 0.0001). Almost 50% of participants had >2 comorbid medical conditions. Past psychological history of depression or anxiety was reported by 58% of participants and half had an elevated baseline depression, anxiety, and/or stress score. The majority of participants (92%) had a baseline morning glucose level ≥100 mg/dL.
Baseline Characteristics of Consecutive AbilTo Diabetes Program Graduates (N = 466)
DASS, depression, anxiety, and stress scale; SD, standard deviation.
Analysis included n = 281 participants with baseline morning glucose values.
Depression, Anxiety, and Stress Outcomes
No significant associations were observed between participant demographic characteristics and baseline DASS score, except females had on average a 1.6-point higher baseline anxiety score versus males (Table 2). Self-reported psychological history of depression and anxiety were each significantly associated with higher baseline DASS scores. Higher comorbidity (comorbidity score >2) was associated with higher baseline depression, anxiety, and stress scores. Elevated morning glucose (≥100 mg/dL) was not associated with baseline DASS scores.
Association Between Participant Characteristics and Baseline DASS (n = 466)
Northeast = reference group.
Values shown in bold indicate statistical significance.
Significant reductions in mean depression (−8.8 points (−51%); p < 0.0001), anxiety (−6.9 points (−45%); p < 0.0001), and stress (−9.9 points (−45%); p < 0.0001) scores were observed from baseline to graduation among participants with elevated scores at baseline. In univariate analyses, age, sex, and higher comorbidity score were not associated with changes in DASS scores.
Among participants with elevated baseline depression scores, 67% transitioned to normal depression scores by graduation. Similarly, 59% of participants with elevated baseline anxiety and 70% of participants with elevated baseline stress scores transitioned to normal scores by graduation (Fig. 1). Fewer than 7% of participants experienced worsening in one or more DASS category scores from baseline to graduation, whereas most participants with non-normal baseline DASS score improved to a less severe depression (81%), anxiety (80%), or stress (86%) category by graduation (Fig. 2).
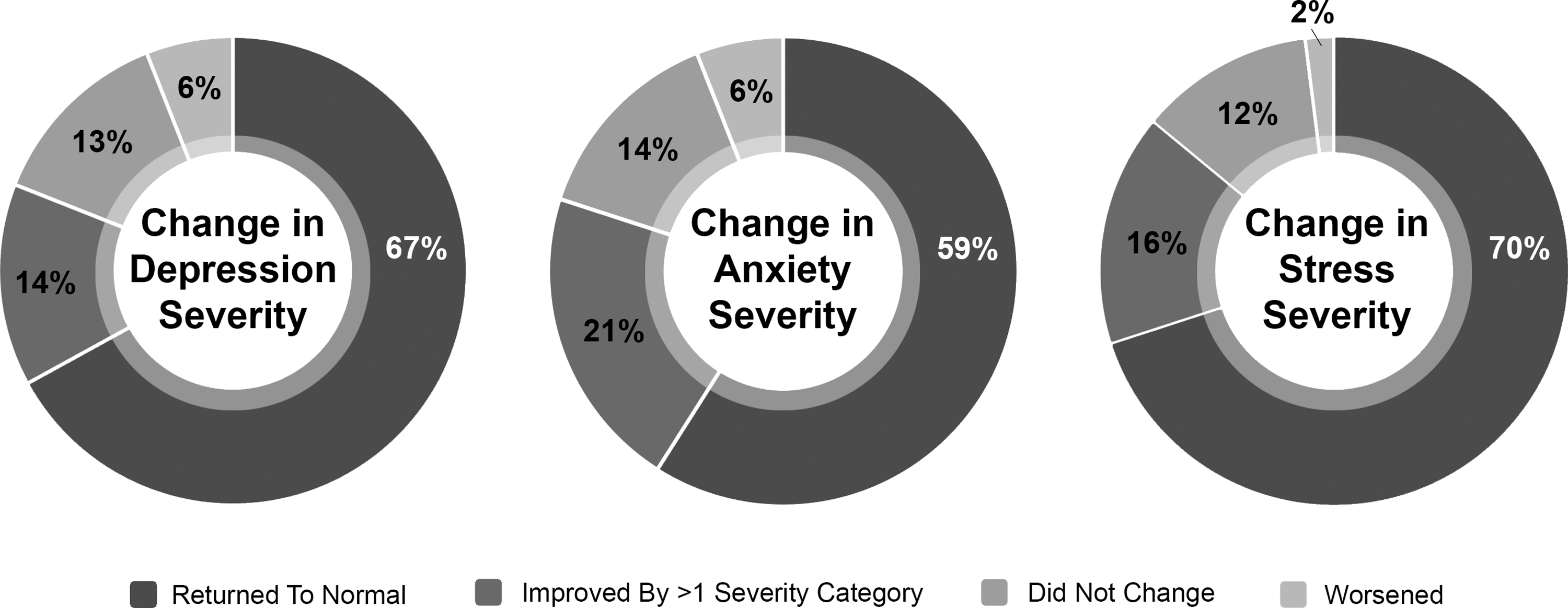
Change in DASS severity among diabetes program participants with elevated baseline scores. DASS, depression, anxiety, and stress scale.
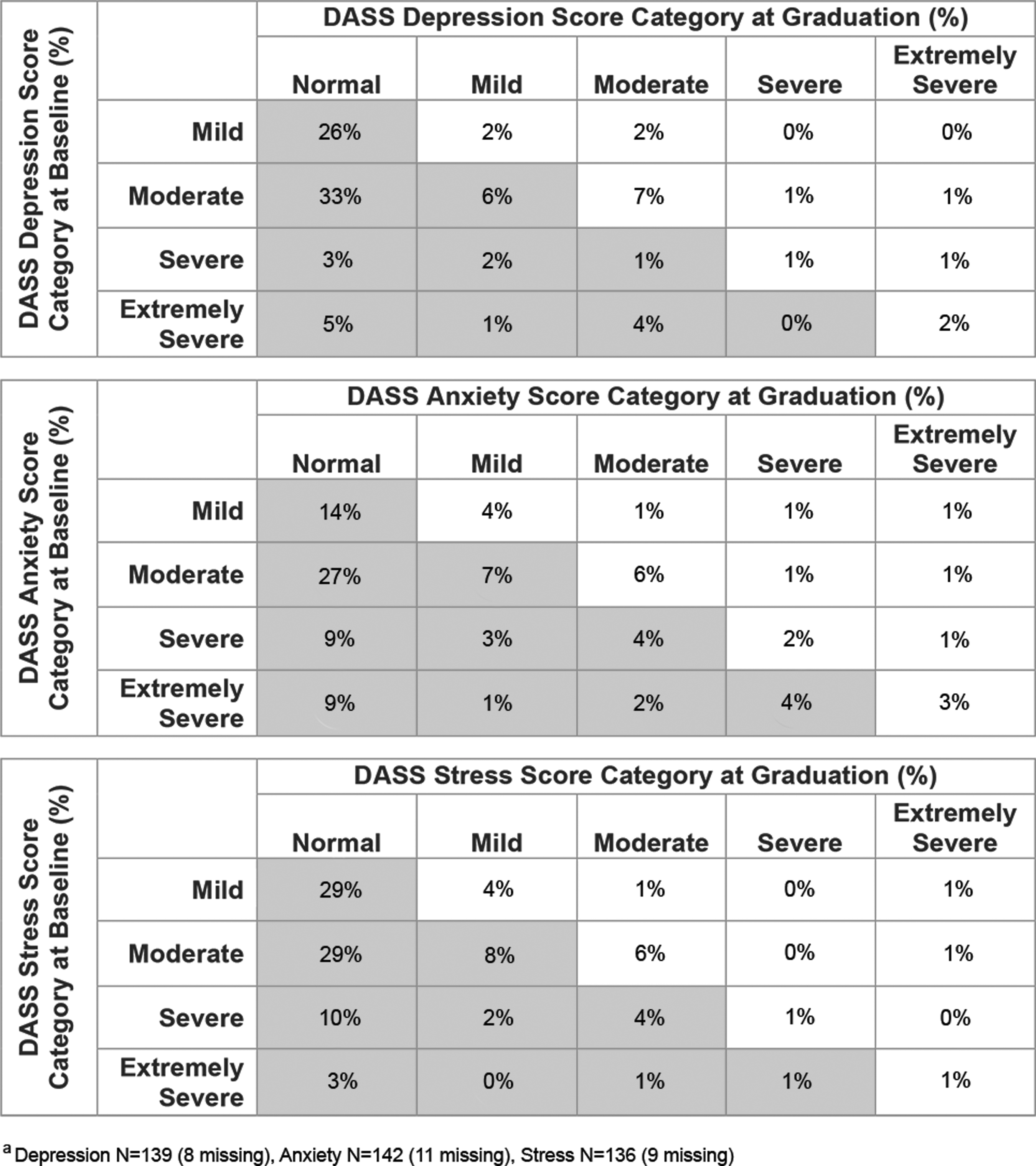
Change in DASS severity categories among diabetes program participants with elevated baseline scores.
Diabetes Self-Care and Outcomes
At baseline, data were available from 281 (60%) participants who had tested and recorded morning glucose levels. The mean baseline morning glucose level among these participants was 146.2 ± 50.9 mg/dL. At graduation, significantly more participants reported glucose self-testing at least once per week (69%; Fig. 3); mean morning glucose at graduation was 135.8 ± 43.1 mg/dL.
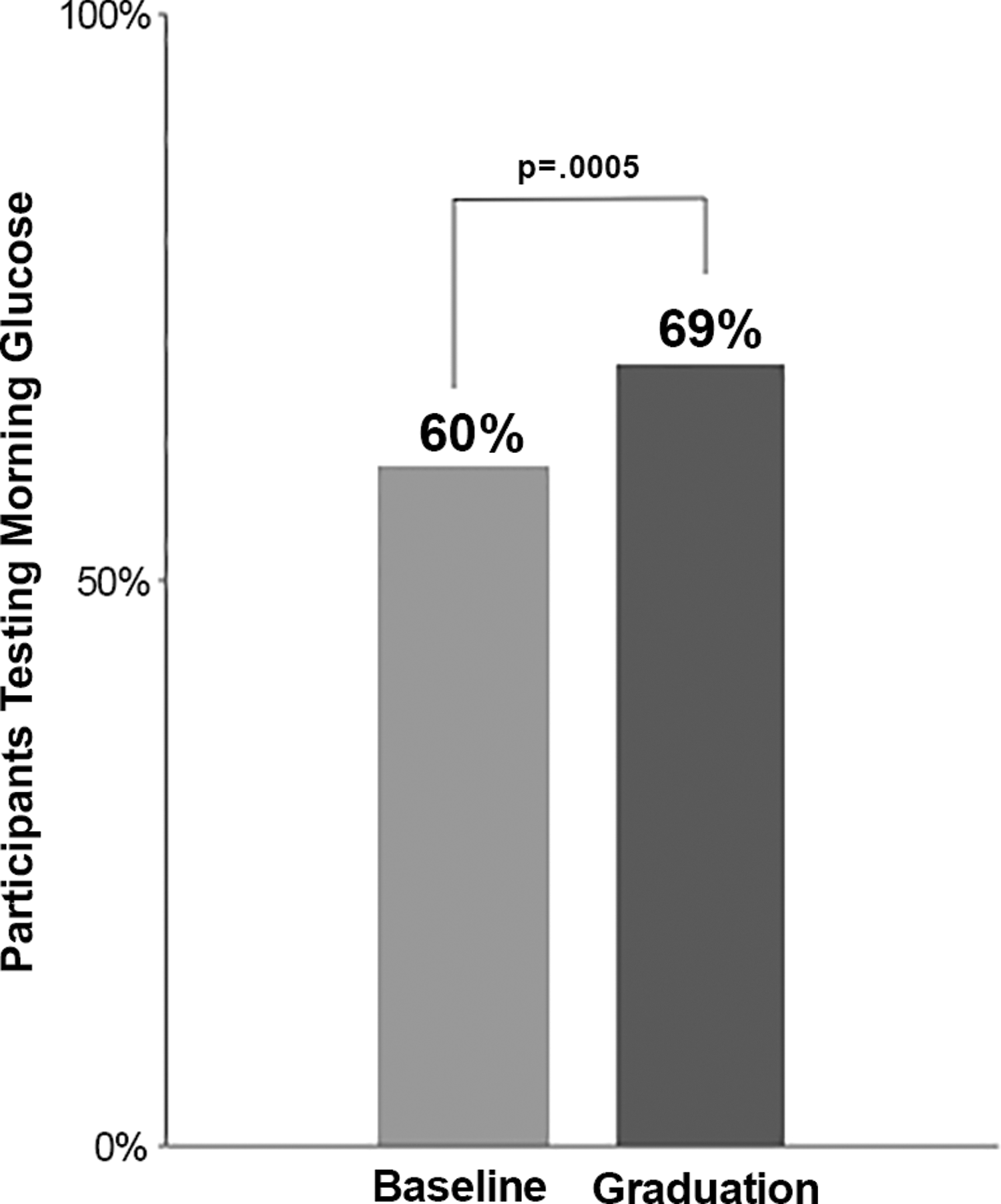
Proportion of participants performing glucose self-testing at baseline and at graduation.
The mean absolute change in morning glucose from baseline to graduation was −12.3 mg/dL (p = 0.0002). When the sample was restricted to participants with above normal (≥100 mg/dL) morning glucose at baseline (n = 214), the absolute change in glucose from baseline to graduation was −15.8 mg/dL (p < 0.0001). Age, sex, or U.S. region was not associated with percent change in morning glucose; higher baseline morning glucose levels were associated with greater mean reductions in glucose over the program period.
Participants with normal depression scores at graduation were more likely to have lower morning glucose levels (<the mean) at graduation versus those with non-normal graduation depression scores (odds ratio [OR] = 2.0; 95% CI = 1.1–3.7); similar associations were observed between normal graduation anxiety (OR = 1.2; 95% CI = 0.7–2.1) and stress (OR = 2.1; 95% CI = 1.1–3.9) scores and odds of having lower glucose levels at graduation.
Discussion
This retrospective analysis of records from over 460 participants in a behavioral telehealth program for patients with diabetes documented significant improvements in mental health and diabetes self-care outcomes. Depression, anxiety, and stress symptom scores each improved by at least 45%; and more than 65% of participants with non-normal baseline depression scores recovered to normal by the end of treatment. Frequency of glucose self-testing increased to almost three of four participants, with significant reductions in mean morning glucose levels observed among participants with elevated baseline glucose values. Normal depression score was associated with lower glucose level at program end.
The specific impact of remotely delivered behavioral therapy interventions on depression, anxiety, and/or stress among patients with diabetes is not well studied. Prior research has examined the impact of educational telehealth interventions on diabetes patient self-management and psychosocial health outcomes and has established feasibility and acceptability. 23 While some of these data have shown that education-based programs can be as effective as in-person interventions to improve emotional well-being, 24 others have yielded no significant differences in mental health improvements, 25 highlighting a need for targeted tele-behavioral health interventions for patients with diabetes.
Our study demonstrated that a standardized behavioral health program, grounded in evidence-based approaches and tailored to diabetes patients, can be successfully delivered through telehealth. Participants experienced significant improvements in depression scale scores associated with clinical improvement and return to normal among two-thirds of participants with non-normal scores at baseline. These results corroborate findings from a small (N = 83) 10-week pilot trial recently conducted by Aburizik et al. 26 The intervention was not solely targeted to diabetes, but results supported efficacy of a counselor-delivered tele-behavioral health intervention to significantly reduce depressive symptoms among U.S. veterans with a chronic condition (diabetes, hypertension, and/or chronic pain). 26 Similarly, Piette et al. recently showed that telephone-delivered, nurse-administered, cognitive behavioral therapy decreased depressive symptoms among a sample of diabetes patients recruited from a community healthcare system. 27 Our program had several distinct characteristics. First, in addition to targeting and improving depressive symptoms, our program targeted and improved anxiety and stress, as well as participants' individual diabetes self-care goals. Second, our program utilized a national network of trained and supervised LCSW therapists, in contrast to site-specific nurses or counselors. Third, our program systematically identified and engaged diabetes patients during a teachable moment such as a recent hospitalization, which may promote behavior change. 28 Fourth, our program enrolled participants from a larger, diverse, nationally drawn sample.
Participants experienced an increase in glucose self-monitoring frequency, with almost three of four testing their morning glucose levels at the time of program completion. Prior data to demonstrate the impact a psychological telehealth intervention has on diabetes self-management behaviors are sparse. However, proof of concept for tele-interventions to increase frequency of glucose self-monitoring and improve glycemic control has been demonstrated through educational and clinically focused interventions. 29 –35 In addition, psychotherapy interventions for diabetes patients, not delivered through telehealth, have been shown to be effective to improve glucose self-monitoring frequency. 14 The results provide new evidence that a behavioral health intervention specifically designed for tele-delivery can be associated with improved diabetes self-management.
Strengths of this study include the evaluation of behavioral health and clinical outcomes among participants in an evidence-based diabetes behavioral telehealth program. Consistent with prior research, our results linked depressive symptoms and glucose levels at program completion, supporting external validity of the clinical data. 36 –38 An additional strength is the national sampling of participants, which (1) allowed us to evaluate associations between diverse participant characteristics and observed changes in DASS scores and glucose levels and (2) illustrates the potential for generalizability and widespread dissemination.
This research has limitations. The nonrandomized single-arm design limits causal inferences linking the program to outcomes. The study includes program completers and results may not be generalizable to participants who did not complete the program. Glucose measures were documented based on self-reported data, which may be subject to bias.
In conclusion, this study demonstrated the feasibility and potential impact of an evidence-based tele-behavioral health program to improve mental health and self-management among persons with diabetes. Depression, anxiety, and stress symptoms, and mean glucose levels decreased among program graduates, while frequency of glucose self-testing increased. Future aims include reassessment of participant outcomes over the longer term to determine persistence of improvements gained over the course of the program period. The high national prevalence of diabetes and associated comorbid depressive symptoms indicate a need for diabetes-focused behavioral health programs that could possibly be filled by a national, scalable, behavioral telehealth program.
Footnotes
Disclosure Statement
H.M.-G., A.L., and L.V. are employees of AbilTo. A.P. is an employee of and holds an equity interest in AbilTo. She serves as AbilTo's Chief Clinical Officer. R.L.P. is an employee of and holds an equity interest in AbilTo. She serves as AbilTo's Chief Medical Officer.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.