
Abstract
Introduction
Conceptualization
Department of Health & Family Welfare, Government of Himachal Pradesh (HP), realized that due to the terrain hostile climatic conditions and isolation of most regions in the state, providing conventional affordable quality healthcare to the community would be impossible. With 90% of the 6.8 million population living in rural areas, HP is the least urbanized state in India with very limited access to specialty healthcare. Government measures to motivate, train, and incentivise the local and external doctors have been unsuccessful. Low population density added to the problem. The valley is isolated for 6 months of the year due to heavy snowfall and freezing temperature of minus 30°C, making movement almost impossible due to road blockages. The objective of the new telemedicine program was to create a conducive environment in remote areas providing the required healthcare support systems, saving lives, and improving the quality of life. Patients requiring emergency care were stabilized before moving them to secondary or tertiary healthcare facilities. Previous attempts to introduce telemedicine, connecting more accessible parts of HP to a government medical college in the region, had been unsuccessful. 1,2
Apollo Telehealth Services (ATHS) submitted a detailed proposal, to provide remote healthcare to the district of Lahaul and Spiti (height of 3,600 m and population 34,000). ATHS would be responsible for the entire work, including providing technology solutions (connectivity, software and hardware), providing teleconsultants, and creating awareness among the tribal communities. A detailed need assessment study was carried out. The team interacted with all stakeholders, including administrators, doctors, district health officials, patients, and the community at the state, district, and village level. It was found that people commuted 20–50 km for primary and up to 250 km for secondary healthcare. Clinical problems included COPD, tuberculosis, asthma, pneumonia, osteoarthritis, diabetes, hypertension, jaundice etc. ATHS was asked to provide Tele-emergency and Telespecialty and Super Specialty services on a public–private partnership (PPP) mode. Government Health facilities at Kaza and Keylong (Fig. 1) were chosen for the initial implementation.
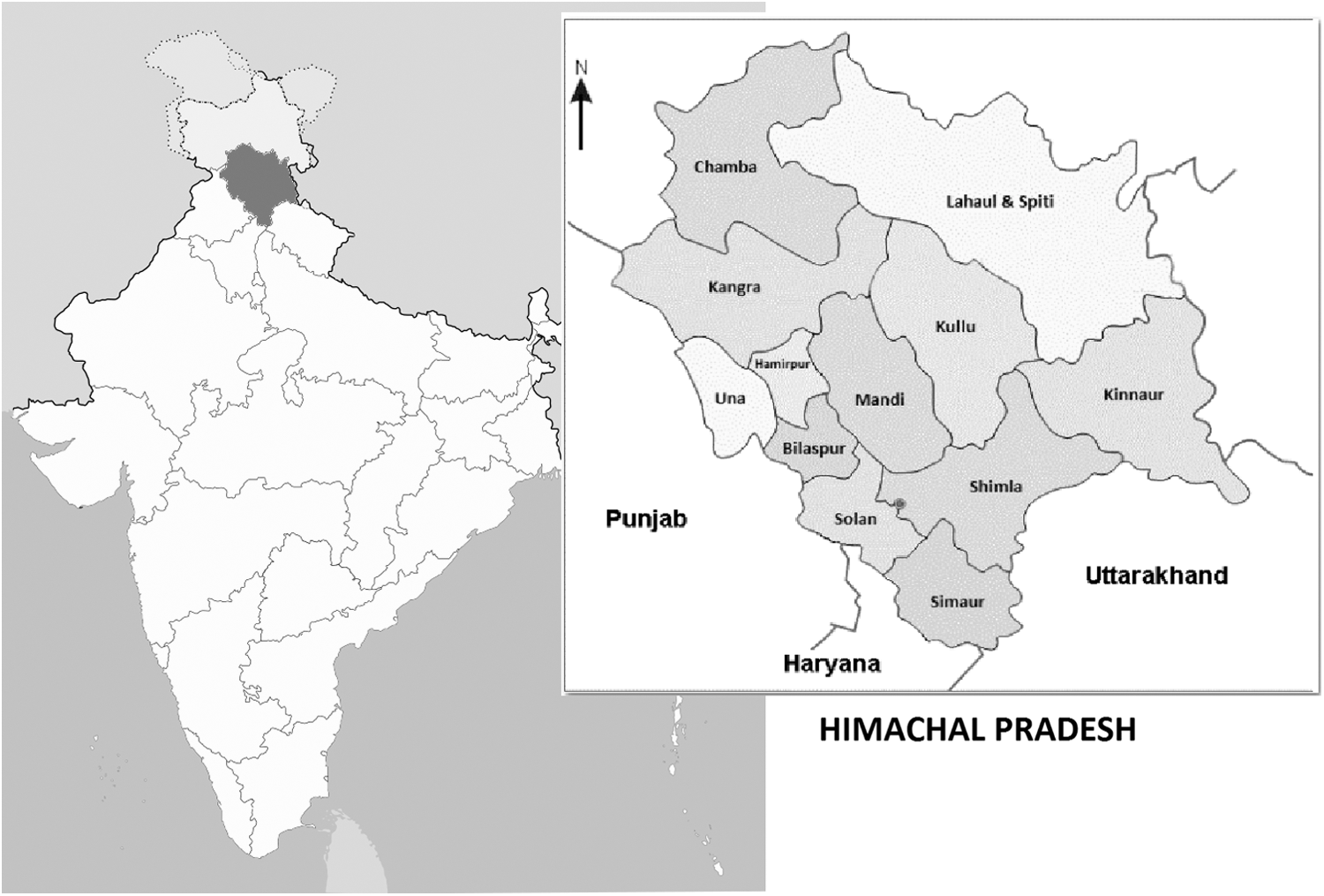
Location of Himachal Pradesh and districts of Himachal Pradesh.
Program management approach included need assessment, budgeting, and defined service level agreements for all major activities. The implementation component included training, capacity building, CME programs, weekly and monthly project reporting, efficient community engagement, and optimized capacity utilization. The monitoring component included joint managing committee reviews, and evaluation component included an impact assessment study, measurable milestones, and monthly reports (Figs. 2 and 3).
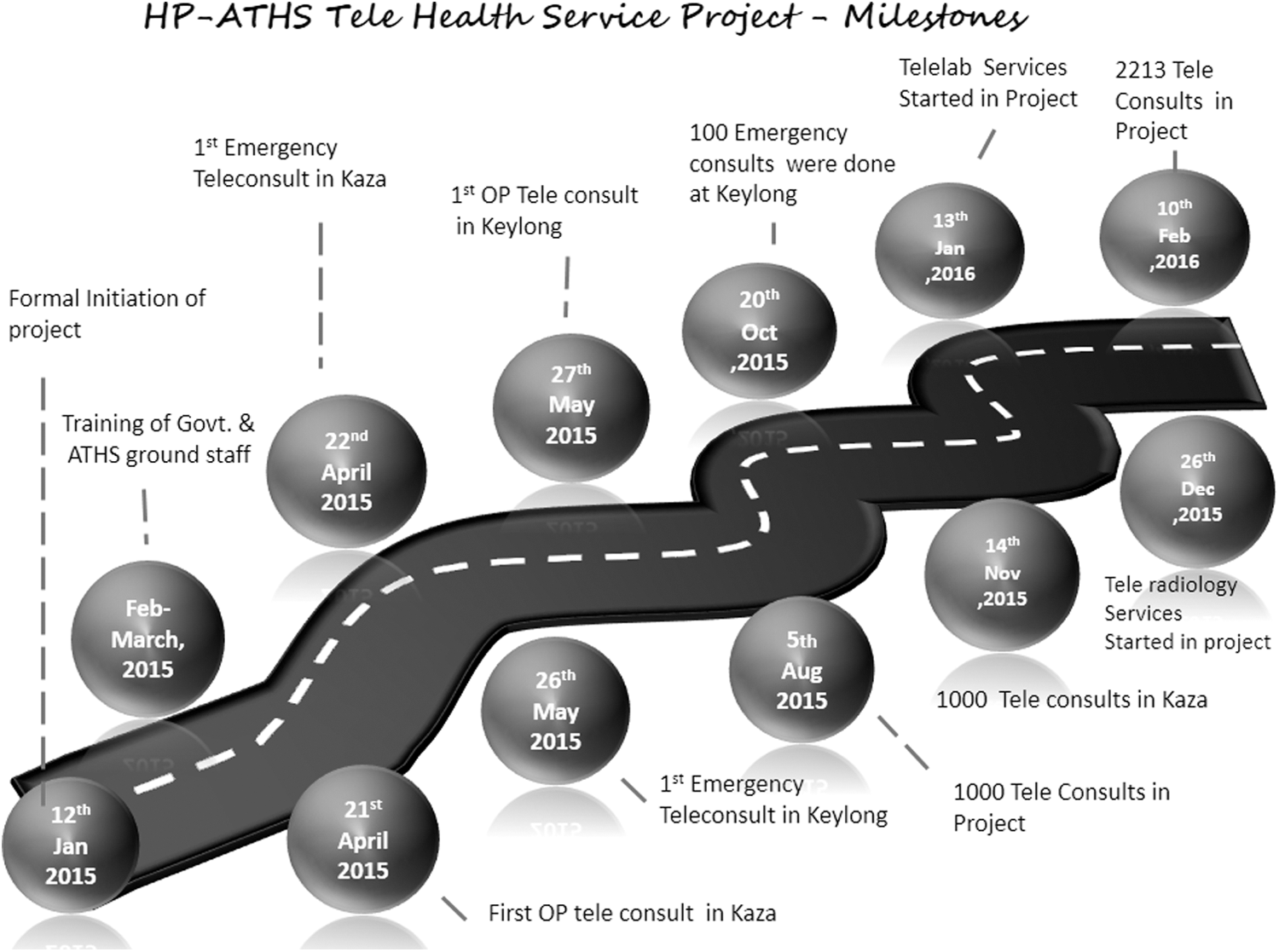
HP-ATHS telehealth project milestones. HP-ATHS, Himachal Pradesh Apollo Telehealth Services.
Monthly report sample first page of Himalayas telehealth. The patient gave permission to use this photograph.
AIM
This included providing access to quality multispecialty health services virtually, through the existing Government Health System, reducing cost and travel, providing 24/7 emergency services, providing government doctors in isolated rural areas access to specialist health information, services, and support, and providing authenticated validated health information to the community promoting health literacy, thus encouraging preventive and promotive healthcare-seeking behavior.
Implementation Process
Human resource provisioning included inducting an existing medical resource team into a training program for capacity building. After an intensive 3-month training at Chennai (Fig. 4), a Telehealth Coordinator/Facilitator and two Telehealth Community Linkage Coordinators were posted at Kaza and Keylong. Training covered basics of telemedicine and telemedicine equipment, information technology training, familiarity with tele-emergencies, trouble shooting for managing Internet connectivity, petty cash accounting, MIS and Reporting, and community linkage programs.
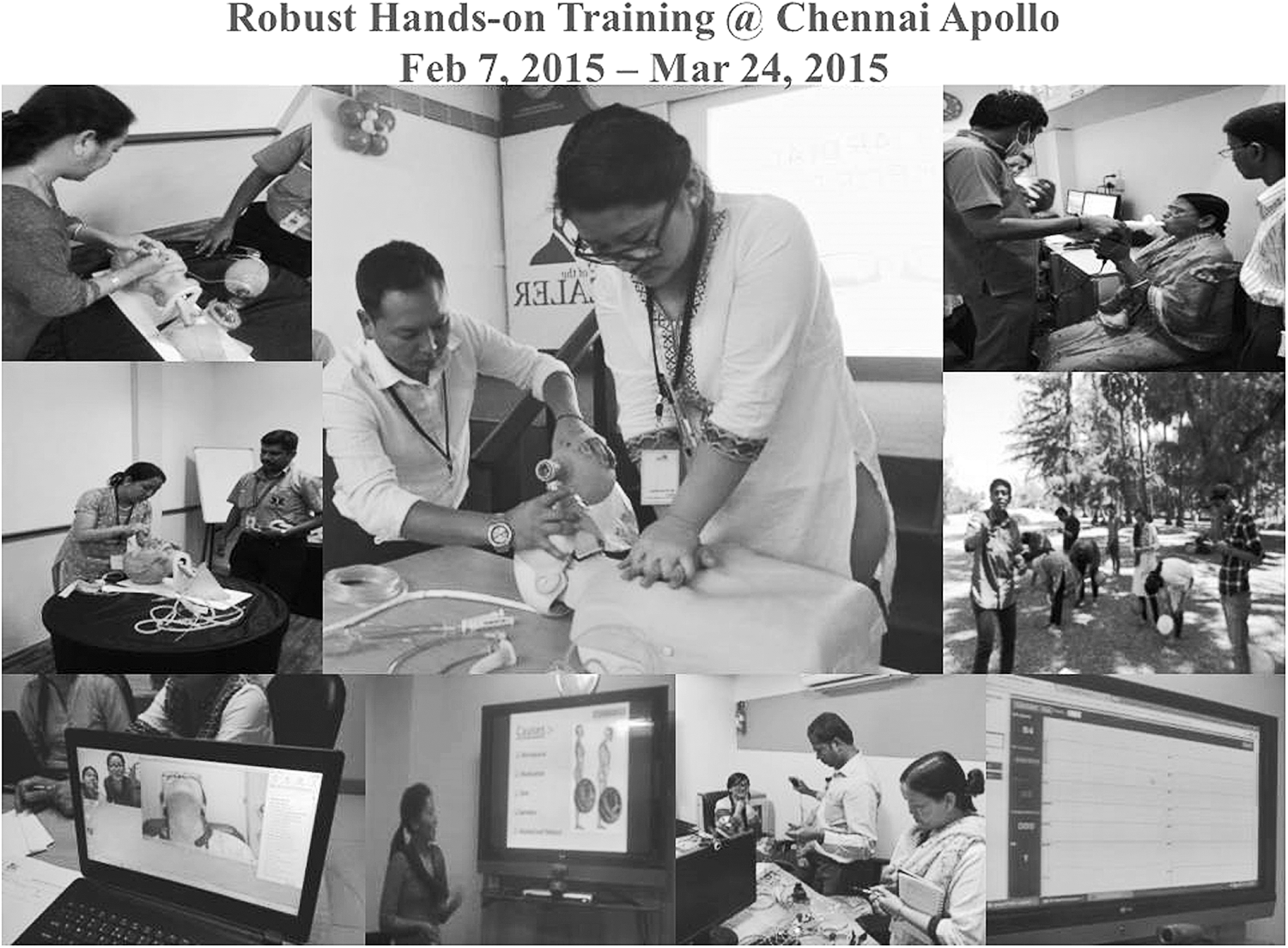
Training at Chennai for telemedicine coordinators. The patients gave permission to use their photographs.
Simultaneously, the required infrastructure was procured. After training, the team moved with the equipment to the project site, activating the site within 20 days (Fig. 5). ATHS initiated a well-integrated teleconsultation unit with remote diagnostic devices (digital 12-lead ECG, Spirometer, 3 and Stethoscope) (Figs. 6 –8) and seamless Internet connectivity of 512 Kbps, enabling telehealth services to the government Community Health Centers in Kaza and Keylong. X-ray films were scanned and sent to Chennai. The telemedicine system blended seamlessly with existing OPDs. With support of a well-trained Telehealth facilitator, patients were able to get teleconsultation with Apollo specialty doctors at Chennai. 3,4 An online appointment booking system facilitated patient interaction. The patient Comprehensive Patient Health Information System (CPHIS) was updated in real time. Personal interaction by telemedicine coordinators on both sides ensured that traditional human touch continued. Scheduled telecamps (virtual out patient services [OPs]) were organized in 15 different specialties and super specialties. If the local government doctor wanted a teleconsult for a “walk-in OP patient,” this was also provided.

Setting up telemedicine in Himalayas.
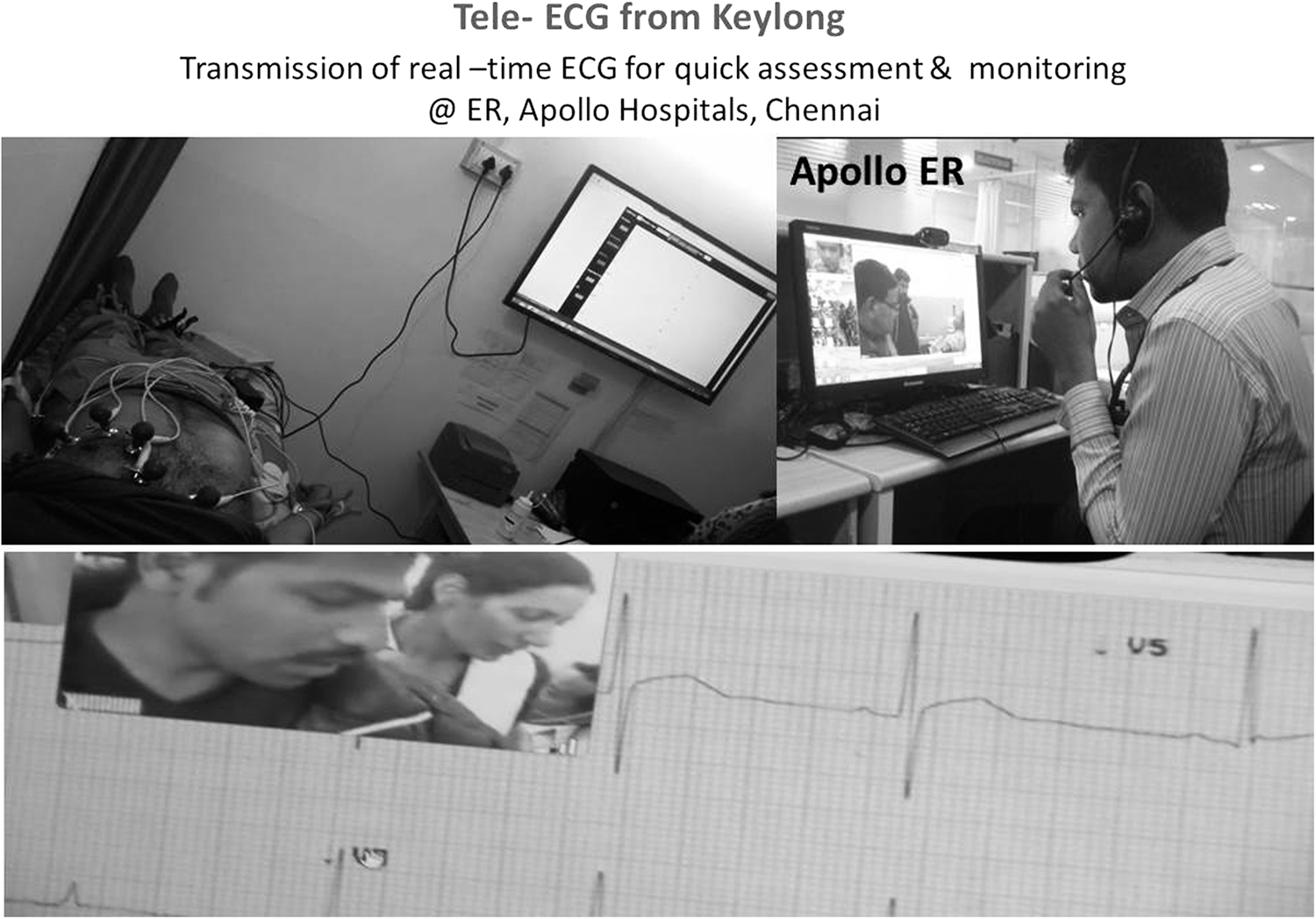
Tele-ECG in Himalayas.

Telespirometry in Himalayas. The patients gave permission to use their photographs.

Telestethoscope. The patients gave permission to use their photographs.
Tele-Emergency Support Services
An experienced ER specialist from Apollo Main Hospital Chennai telementored the CMO/duty nurse at Kaza and Keylong to provide initial medical support to stabilize patients. One hundred seventy-one out of 2,213 teleconsults were emergencies. Emergency medicine, medical disposables, hardware/software, emergency mobile cart, and videoconferencing systems for direct real-time interactions between the casualty at HP and ER specialists at Chennai were made available.
Challenges and Difficulties Encountered During Implementation
Mobilizing equipment within time constraints, facing melting snow and landslides was the first obstacle. 5,6 Bandwidth issues (technical and commercial) were mitigated by seeking redress at the highest level. Dedicated, customized Very Small Aperture Terminals were provided by BSNL 7 —(India's largest government network provider). Major change management issues were faced with the local staff, who initially perceived telehealth as a threat. Limited infrastructure, multiple dialects, poor health-seeking behavior, and total unawareness of telehealth compounded the challenges. Technology provided virtual specialists on a screen—but making available drugs prescribed and tests requested was extremely difficult. Making sophisticated urban teleconsultants constantly use generics for limited medicines available and avoiding multiple and sophisticated investigations were also difficult. Trained coordinators made house-to-house visits to create awareness within the community (Fig. 9).
Coordinators reaching the community in Himalayas. The staff and patients gave permission to use their photographs.
Benefits of the Project to Various Stakeholders
The stakeholders included the 34,000 citizens of the district, the healthcare providers in the Government of HP, and the National Health Mission of the Government of India—as successful implementation of this project could result in escalation to other remote areas. Members of the community have been trained and provided with jobs. Social Health Education Programs to provide knowledge empowerment and health literacy have been started. 8 Our 2-year experience in Tamil Nadu 9 indicates that we could create a significant awareness of health-related issues among the community. The urban “elite” consultants in the metros now have an opportunity to understand the real problems in rural India. This will encourage city doctors to spend effort and time in “virtually” attending to their less-empowered brethren. It required a radical transformation to make these consultants manage individuals with only a clinical diagnosis.
Cost-Effectiveness
The government of HP had been willing to spend $375,000 (USD)/year as compensation to make available 10 specialists for the district. These salaries were almost triple of what is normally paid. Despite these inducements, it was not possible to persuade doctors to physically reside in the district. Additional expenses were incurrred on helicopter evacuations for seriously ill patients. The total cost of the telehealth project for 15 months, with its major societal impact, was $350,000 (USD). A detailed survey of 105 users of the telehealth services indicated that in addition to saving considerable effort, time, physical discomfort, and emotional stress, $13,040 (USD) would have been spent in travel alone for obtaining perhaps suboptimum healthcare. If extrapolated to all the users provided teleconsults so far, the community would already have saved $217,000 (USD). The nontangible benefits are literally priceless and cannot be quantified, including the happiness that a caring government has facilitated quality accessible healthcare with no cost to the end user. Benefits to the environment include reducing carbon footprint, as about 100 ambulance trips of 150 km and probably five helicopter evacuations have already been avoided.
Achieving Clinical and Service Excellence
A detailed preliminary assessment of the Telehealth Services in the first 100 days was presented as an interim report to the government. This critical self-review pointed out the challenges, difficulties, and limitations and offered doable suggestions. The government responded immediately sanctioning telelaboratory services, increasing availability of drugs, providing additional backup power etc. Figure 10 shows the speciality distribution and Figure 11 the age distribution. The distribution of the specialty and superspecialty teleconsults, 10 constituting 69% given from Chennai, are enumerated in Figure 12 –19. The remaining 31% of teleconsults were given by experienced family physicians from the Medical Response Center at Hyderabad. Frequency of uitilization of different specialties may give a general idea of the incidence and prevalence of those clinical conditions in the community, although there are other compounding factors. As can be seen from Figures 12 –19, only a provisional clinical working diagnosis could be arrived at, due to infrastructure limitation, but it sufficed for management of symptoms.

Distribution of specialty teleconsultations.
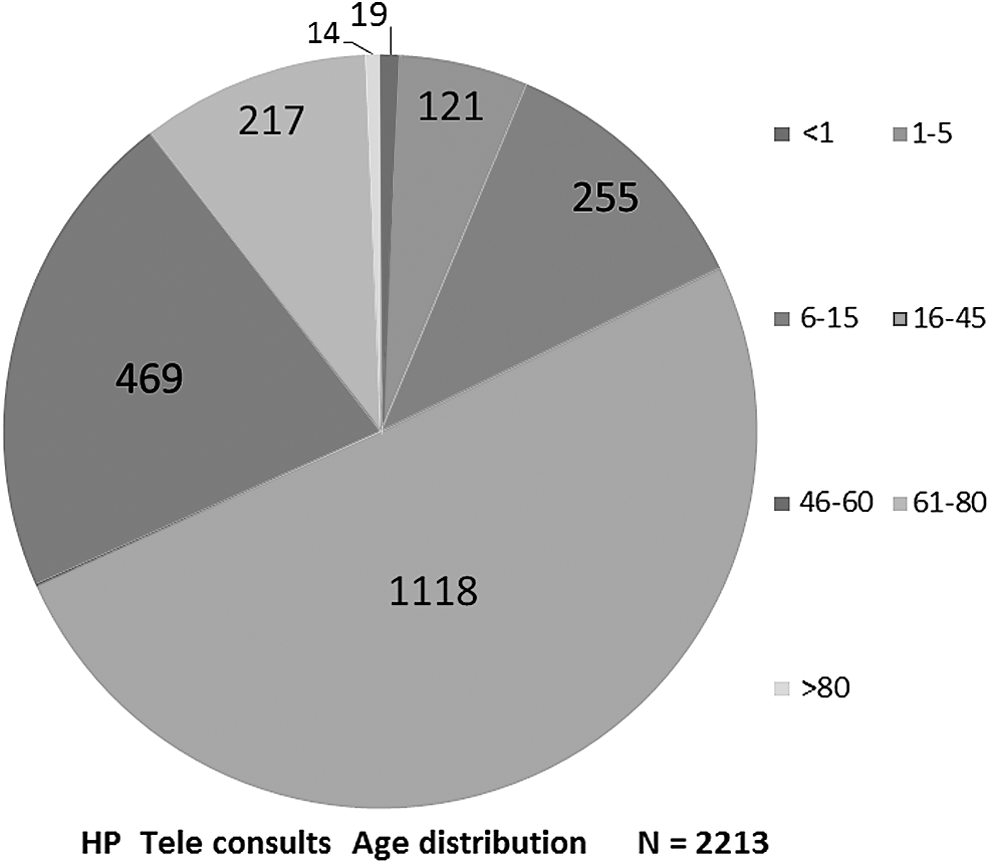
HP teleconsults age distribution.

Orthopedics clinical diagnosis, N = 359.

Gastroenterology clinical diagnosis, N = 191.

Obstetrics and gynecology clinical diagnosis, N = 187.
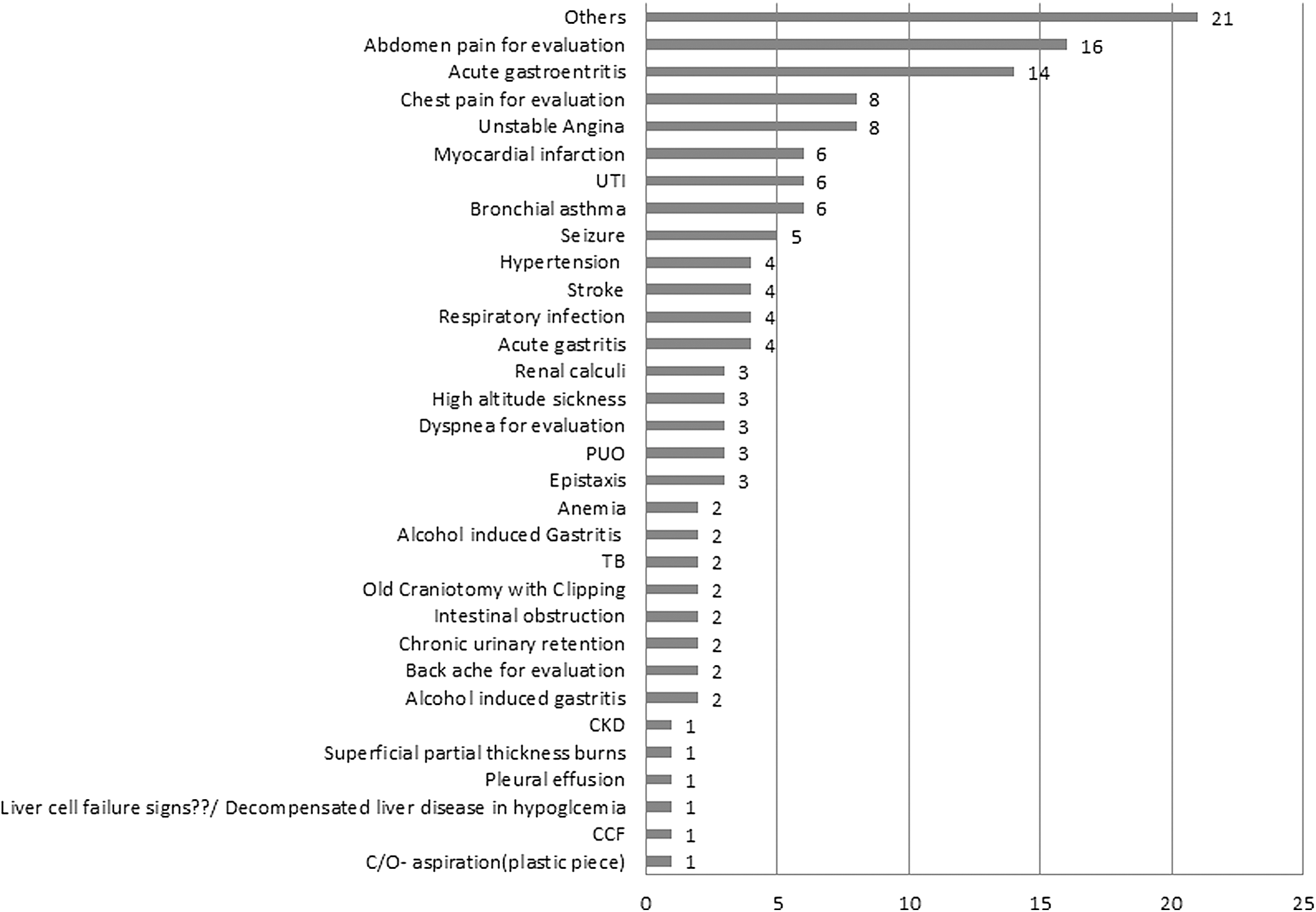
Emergencies clinical diagnosis, N = 169.

Pediatrics clinical diagnosis, N = 162.
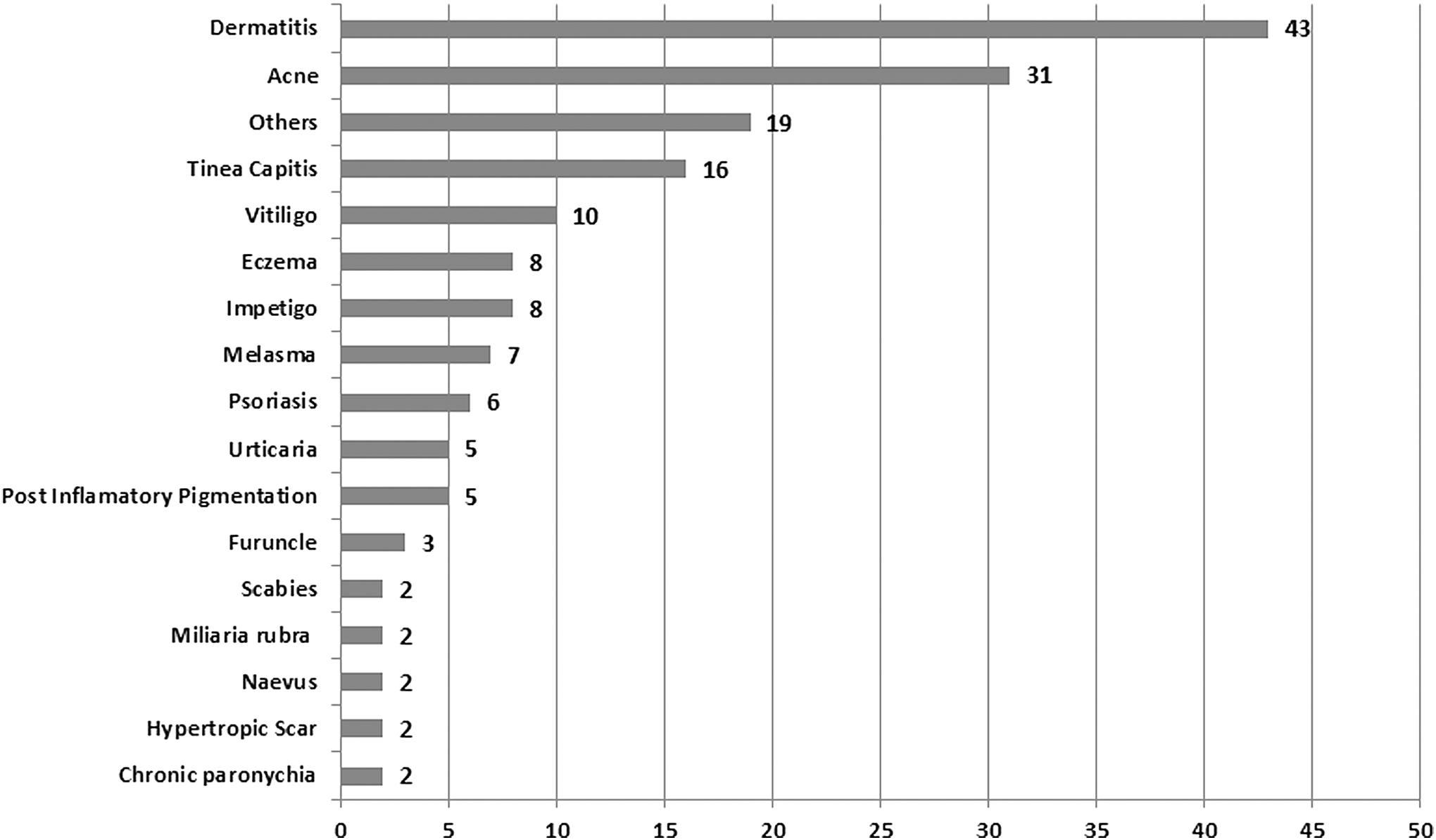
Dermatology clinical diagnosis, N = 171.
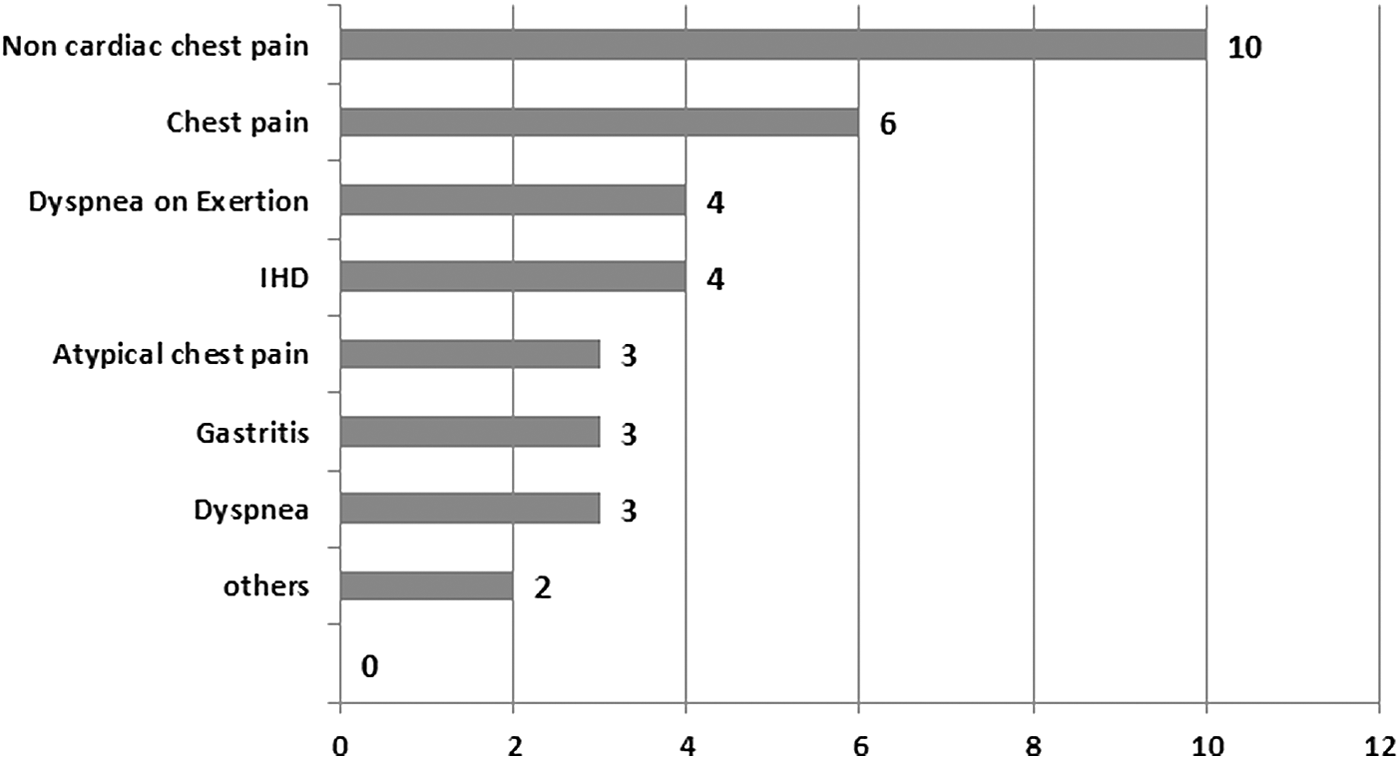
Cardiology clinical diagnosis, N = 56.

Urology clinical diagnosis, N = 28.
Telelaboratory Services
Using a U.S. Food and Drug Administration (FDA)-approved Point-of-Care Diagnostic (POCD) Kit, blood biochemistry, including lipid profile, LFT, RFT, HbA1C, Hb, and PCV, was made available at the remote telemedicine location itself. The local staff were virtually trained and soon became adept at using the kit (Fig. 20). In 7 weeks, random blood sugar was checked in 434, Hb in 325, PCV in 307 had TSH, Troponin I in 8, besides urine routine in 28, TSH 6, and lipid profile in 2, resulting in better clinical management.

Deployment of Point-of-Care Diagnostic (POCD). The patient gave permission to use her photograph.
Telecervical Cancer Screening
In a first of a kind, pilot initiative telecervical cancer screening has commenced (Fig. 21). A nurse trained semivirtually performs a cervical speculum examination and takes a smear after coating with acetic acid. These images are captured and sent to a senior consultant gynecologist in Chennai who reviews the images and counsels the patient. Smears are couriered to Chennai where the slides are evaluated by a trained cytopathologist. Out of the first six patients for whom this was done, clinically four were normal and two were diagnosed to have cervical erosion.

Tele cervical cancer screening. The patients gave permission to use their photographs.
Patient Satisfaction
Objective assessment of user satisfaction is under way. An interim interview of 659 patients (Fig. 22) revealed that 75% were delighted and only 9% dissatisfied with the telehealth services provided 11 (Ref. 11 due to patient confidentiality, only a single edited VOC audio has been provided in the public domain).

Voice of Customer patient feedback. The patients gave permission to use their photographs.
Discussion
While successful PPP in Healthcare in India are reported, most of them are Health Insurance related, for example, Yeshasvini Health scheme in Karnataka and Arogya Raksha Scheme in Andhra Pradesh. Emergency Ambulance Services in Tamilnadu and mobile hospitals in Uttaranchal are other examples. 12 Specialized services include Apollo hospitals operating a dialysis unit for the state government of Uttarkhand with telenephrology consults being added shortly. 13 Although an administrative decision, for PPP to be successful, political and community support are essential. The novelty of this first of a kind initiative is evidence that if used judiciously and customized, PPP can change the healthcare landscape, if interests of all stakeholders are considered. Formulating legal and regulatory framework together, the confidence of both players to invest in such partnerships would increase. PPP will help mobilize resources for specialist healthcare.
Telehealth in the Himalayas, has much in common with that provided in other inhospitable terrains. In the jungles of northeastern Peru, telehealth was initially enabled with two-way voice and digital radio connections. 14 In another pilot project, telehealth was deployed in 39 rural sites of the Alto Amazonas province, in the center of the Peruvian Amazon region. 15 Continuous virtual remote monitoring in remote hostile areas was demonstrated when a swimmer was closely monitored across the amazon basin of Peru and Brazil over 70 days. 16 Satellites have brought reliable voice communication in the 1970s with the Alaska Federal Healthcare Access Network (AFHCAN). This satellite-based system linked 248 sites, including 158 village health centers, to address the small indigenous population spread over a large area and shortage of doctors in Alaska. 17 Although in some ways the social and clinical issues were comparable, the authors have used a different technology. VSee, a HIPAA-compliant telehealth app, is being used for video conferencing, keeping patient data secure with 256-bit AES encryption. Partnering with e-KSS VSee has provided peer-to-peer low-bandwidth video that worked over satellite broadband and 3G networks in the Amazon. 18 Several publications 19 –21 have highlighted the specific challenges encountered in providing health services in mountainous areas. Although many solutions have been suggested, telemedicine is not one of them. Reports describing remote healthcare in the Himalayas deal with sporadic telemonitoring of physiological parameters in climbers. Daniel et al. 22 studied sublingual microcirculation in volunteers. Doctors in Yale University 23 had daily virtual morning rounds and treated nonemergency conditions such as high-altitude headache, gastroenteritis, and uncomplicated pneumonia in climbers. Several complex cases were discussed with consultants. Clinical tests repeated at various altitudes along the way to the Everest Base Camp have been reported. 24 Publications reviewing the deployment of telemedicine for regular continuous clinical care in mountainous areas and other remote isolated regions are limited. Martinez et al. 25 demonstrated that 9 months after setting up a telemedicine system in the Amazon region of Peru, consults increased from three per month per facility to 23. Of 205 emergency transfers from 39 health facilities, teleconsults saved 28%. Voice and e-mail communication through VHF radio were feasible and useful for rural telemedicine in these inhospitable terrains. Patients in the White Mountains, New Hampshire, have virtual access to board-certified neurologists. 26 Telepsychiatry services are available for the residents in the Blue Ridge Mountains in the Eastern United States. 27 A pilot project was said to have been carried out in the mountain villages of Myagdi district, Nepal, where health workers and patients were connected to central hospitals. However, specific information is not available. Northern Pakistan, known for its difficult terrain, extreme climate, and isolation, has very poor health services. In 2005, the Commission on Science and Technology for Sustainable Development in the South (COMSATS) collaborated with the International Development Research Centre (IDRC) and the Baltistan Health and Education Foundation to establish a telehealth service. As wireless local loop and digital telephone exchanges were insufficient, and COMSATS established the first Internet service. The 1,000th teleconsult was done in May 2006. 28
All seven hospitals in the mountainous Comune di Nuoro (Sardinia) catering to 270,000 people have access to telehealth. 29 Although the Nuoro province is said to have one of the highest peaks in Southern Europe and can only be traversed by rough country roads, it is not comparable to Kaza and Keylong height of 3,650 and 3,080 m, compared to 560 m in Nuoro where this study is being carried out. Here, the temperature can go down to −30°C. At Nuoro legacy, PABXs and leased lines were replaced with high-speed switches, and a 3Com Wireless LAN Building-to-Building Wireless Bridge, between the hospital networks. For this study, a novel reliable 24/7 premium package was worked out with a committed bandwidth of 512 Kbps uplink and 512 Kbps downlink. This package from BSNL 7 was highly subsidized, considering the healthcare application. Normally, expensive C-Band satellite or intermediate Ku-Band satellite connectivity would have been the options. Ku-band normally available with service providers is unreliable in terms of committed bandwidth. It normally works on shared bandwidth in the given region, depending on the capability of the transponders of the Satellite, which is synchronized with the V-SAT terminal of the site. This solution works on a first in–first out principle for data packet transfers over the network, reducing reliability. Wireless connectivity (WiFi, WiMax) was not possible due to the Himalayan range altitude and contiguous mountain range with no line off-site. Terrestrial optic fiber connectivity, although available, was unreliable due to physical cable cuts in the summer and inability to relay data during winter.
Tele-Emergencies
Several publications dealing with tele-emergencies were reviewed. 30 –37 In a study of 60,193 emergency department encounters presenting over 30 months at 21 hospitals, tele-emergency services were used only in 3.5%. 38 No reports were available of regular tele-emergency services being provided in high-altitude isolated areas. 7.7% of teleconsults in this study were emergencies.
Conclusion
In the first 42 weeks, 1,747 patients, including seven overseas tourists, have utilized telehealth services constituting 5.15% of the district's population. Mean distance travelled for specialist teleconsultation is now 35 km as against the original 250 km. Every 88 min, a new patient was treated in the telehealth centers in Lahaul and Spiti (lowest population density of two persons per square kilometer). Every fourth day, a patient was stabilized through Tele-Emergency services. Reviewing the interim report, the National Health Systems Resource Centre, WHO—the Collaborating Centre for Priority Medical Devices and Health Technology, Government of India, recognized this particular PPP delivering remote healthcare as “… a good, replicable, and innovative practice for 2015.” 39 Harsh weather, cultural isolation, and infrastructure limitations compound the challenges in carrying out a detailed scientific impact analysis. However, this is ongoing and will form the basis of a subsequent report. The HP-ATHS program has already made a sustainable healthcare impact within an isolated community, unequivocally demonstrating that remote healthcare delivery in a PPP mode is socially relevant, financially sustainable, and scalable. This preliminary analysis indicates that, given the right partners, it is possible to innovate, customize, and scale up remote healthcare in inhospitable terrains in a PPP mode anywhere in India. Looking to the future, the Government of India proposes to commission SATCOM-based telemedicine centers for four holy pilgrimage sites in the Himalayas. 40
Footnotes
Acknowledgments
Prathap C. Reddy, Founder Chairman; Preetha Reddy, Vice Chairperson; Sangita Reddy, Joint Managing Director; Anupam Sibal, Group Medical Director; Sathyabhama DMS; Sathyanarayana Reddy, former CEO; Anne Moncure, former CEO; Arvind Sivaramakrishnan, CIO; and V. Subbiah, COO—all from Apollo Hospitals; Vikram Thaploo, CEO, Apollo TeleHealth Services; various teleconsultants from Chennai and Hyderabad, including Dhavapalani, Head Emergency Services, and Ayesha Nazneen, Ramesh, Vishnu, and Anusha; the field workers at Kaza & Keylong, Samriti Sharma, Sonam Lamo, Thinley Tsomo, Lamo Butit, Tanzin Yeeyong, Tanzin Dolker, Kewal Krishan Tenzin Norbu, Tenzin Lhanze, Chhering Dolma, Saroj Kumari, Padma Butit,and Yangchen Dolker. Mohan Lal Shashini, Angdui Norbu, and Balkrishnan all helped in different ways.
Mrs. Vijayalakshmi Ganapathy rendered secretarial assistance. Permission has been obtained from patients, used in video demonstrations.
Disclosure Statement
No competing financial interests exist.