
Abstract
Introduction
Telecare to Deliver Multicomponent Care Models for Serious Mental Health Conditions
Collaborative chronic care models (CCMs) were established to address the needs of individuals with complex, chronic medical illnesses. 1,2 CCMs consist of six elements: (1) work role redesign for anticipatory continuous care, (2) patient self-management skill enhancement, (3) provider decision support, (4) information management, (5) access to community resources, and (6) organization and leadership support. 3 These elements are operationalized in various ways depending on facility capabilities and needs. While initially developed to treat chronic medical illnesses, CCMs have also been applied to depression treated in primary care 4,5 and a wide variety of mental health conditions. 6,7
However, establishing CCMs to treat complex conditions requires both a critical mass of patients with the diagnosis of interest plus providers with specialty expertise in its treatment in the same venue—requirements rarely met in U.S. healthcare. 8 Telehealth modalities have potential to overcome this limitation in reach 9 of CCMs by bringing together specialists and patients across different sites. Ideally, with modern communications and informatics technologies, virtual teams can come together seamlessly across distance to support an individual's healthcare needs.
The U.S. Department of Veterans Affairs (VA) recognized that bipolar disorder could be addressed through telehealth application of CCM principles. In 2011, the VA telehealth and mental health leadership established the Bipolar Disorders Telehealth Program, utilizing a multidisciplinary team, or “clinical microsystem,” 10 to complement local care through clinical video teleconferencing (CVT). More than 100,000 veterans receive VA care for this diagnosis each year. 11 Bipolar disorder affects 9 million Americans and is characterized by high rates of morbidity and early mortality. 12 The condition is also characterized by a high prevalence of medical 13,14 and mental 13,15,16 comorbidities, requiring coordinated management of multiple conditions. Nonadherence with medications is endemic. 17 On the positive side, CCMs for bipolar disorder have an extensive evidence base 6,7 and have been endorsed by multiple clinical practice guidelines. 18 –20
The Promise and Challenge of Telecare for Severe Mental Health Conditions
Ample evidence demonstrates the feasibility and benefit of using remote clinicians to deliver care for depressive and anxiety disorders using telephone, 21,22 CVT, 23,24 or other informatics-based modalities. 25,26 However, less is known regarding the feasibility or impact of telehealth modalities for severe mental health conditions or its use for multicomponent models such as CCMs (see Discussion section), and we are aware of no studies of telecare for bipolar disorder. Moreover, substantial implementation challenges exist, including provider skepticism, technology barriers, licensing and credentialing, 27 and concerns about privacy and security risks. 28
Thus, more evidence regarding the feasibility and impact of telehealth modalities is needed, particularly in naturalistic settings outside of clinical trials. 29 We, therefore, undertook an evaluation of the acceptability and clinical impact of the CVT-based bipolar CCM deployed in the VA healthcare system after enrolling the first 400 participants.
Materials and Methods
Program Description
Bipolar Disorders Telehealth Program currently supports 0.6 FTE psychiatrist and 2.6 FTE psychologists based across two facilities in New England. Clinicians are credentialed and privileged to deliver care through memorandum of understanding between the Office of Telehealth Services and each patient site, providing clinical care consistent with American Telemedicine Association (ATA) guidelines for telemental health. 30 Sites were recruited by means of word-of-mouth initially and then through conference calls with regional VA mental health leadership across the country.
Clinical procedures are based on the Life Goals Collaborative Care Program, a bipolar CCM
31,32
which is guideline endorsed
18,19
and listed on the Substance Abuse and Mental Health Administration's National Registry of Evidence-Based Programs and Practices ( • Structured diagnostic assessment, including comorbidities (CCM element: provider decision support). • Psychopharmacologic consultation (CCM element: provider decision support). • Life Goals Self-Management Skills Program (CCM element: self-management skill enhancement) consisting of six structured, manual-based modules covering goals and values, mania and depression profiles and coping responses, provider visit preparation. • Follow-up monitoring, including measurement-based symptom assessment and liaison with primary providers (CCM elements: information management, work role redesign for anticipatory continuous care).
The program is operationalized as a consultative team model: In addition to conducting self-management sessions and doing follow-up monitoring, bipolar Telehealth staff make medication and monitoring recommendations to the primary mental health provider but do not write orders (Fig. 1). Participants are enrolled for ∼6 months, although the length of enrollment is determined by completion of tasks rather than strictly chronological time. As illustrated in Figure 2, the intake is completed by the program psychiatrist, focusing primarily on diagnostic, psychopharmacologic, and medical issues, as well as administering health status self-report rating scales. This is followed by six Life Goals Skills Management Program modules delivered by the program psychologist, with additional optional modules as clinically indicated. At ∼1 month after the final Life Goals session, the psychologist conducts a booster session to reinforce Life Goals lessons and to administer the health status self-report rating scales. We estimated that these activities would take ∼6 months, given scheduling complexities and the need for extra sessions for some individuals.
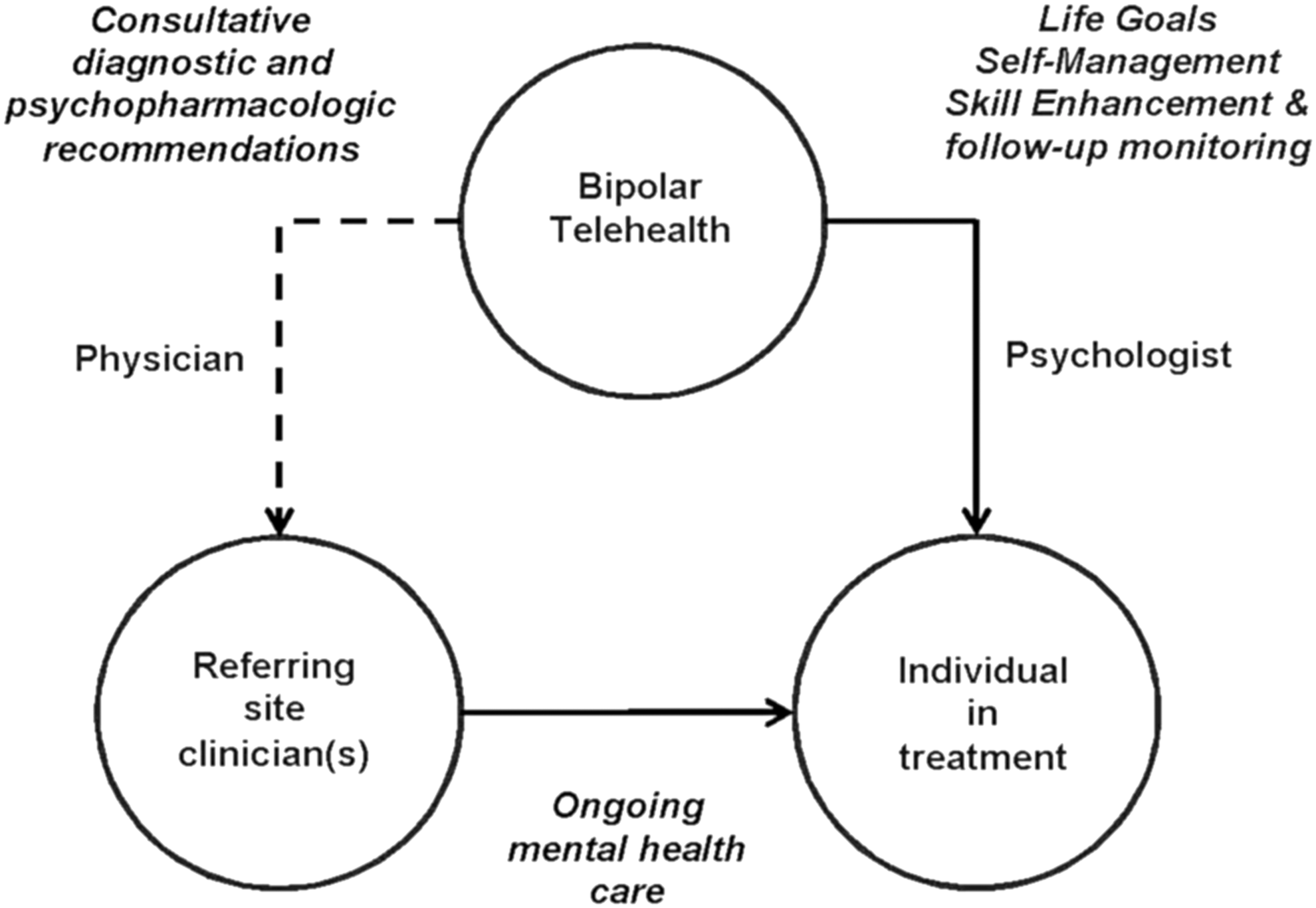
Bipolar Telehealth represents a clinical microsystem, constituted in time-limited manner, 10 to focus on the individual's unmet biopsychosocial needs in the context of bipolar disorder. As outlined in the text, the Bipolar Telehealth psychiatrist provides differential diagnosis and psychopharmacologic consultative recommendations to be acted on (or not) by the individual's on-site mental health provider. The Bipolar Telehealth psychologist then works directly with the individual in treatment, using the Life Goals Self-Management Skill Enhancement Program 30,31 and monitoring health status. The dotted line represents consultative recommendations and the solid lines represent direct treatment.
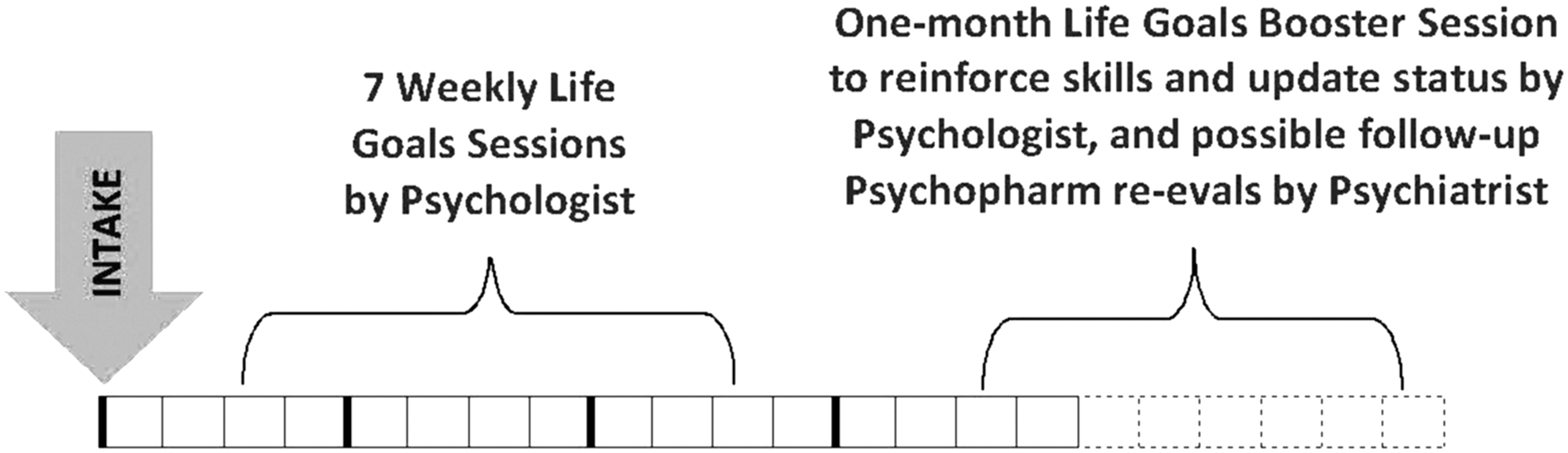
Enrollment in Bipolar Telehealth begins with a comprehensive biopsychosocial intake by the psychiatrist, covering primarily (1) assessment of differential diagnosis and psychiatric comorbidities, (2) psychopharmcologic and medical comorbidity management, and (3) self-report health status assessment using standardized health status measures. This is followed by 7 weekly Life Goal self-management skill enhancement 30,31 modules conducted by the psychologist focusing on self-management skill enhancement and health status monitoring. Approximately 1 month after the final Life Goals session, a booster session is scheduled to reinforce Life Goals skills, terminate the consultation, and readminister the health status assessments. We inform providers and individuals in treatment that the overall program enrollment may last 6 months, with the actual time in program varying due to wait times between intake and Life Goals, scheduling flexibility of Life Goals sessions, and the use of additional Life Goals modules to address other issues (e.g., physical wellness, harm risk, psychosis, anxiety).
The target population consists of veterans enrolled in VA outpatient care with known or suspected bipolar spectrum disorders, including cyclothymia and schizoaffective disorder, without other exclusion criteria. Individuals are required to be in treatment with a local mental health provider and agree to CVT-based evaluation.
In the first year of the program, we added a chart review consultation option for individuals who could not or would not participate in CVT evaluation, to provide at least some consultation to all providers who requested our assistance. This consultation focuses on diagnostic and psychopharmacologic aspects of care, with asynchronous communication between consultant and referring provider inspired by Project ECHO 33 methods (chart review consultation followed by invitation to the referring provider to dialogue with the consultant by e-mail and telephone).
Services are accessed by means of consultation request in the patient-site electronic health record. Clinical communications are made using chart note in the patient-site electronic health record plus e-mail, telephone, and secure messaging communication with providers as needed. Safety contingency plans are established with each site before the program is opened at that site.
Program Evaluation Plan
This program evaluation was approved by the VA Connecticut Institutional Review Board. Evaluation was informed by ATA guidelines for evaluating telemental health, 34 particularly treatment engagement, including identification of subpopulations at risk for not being reached; participation in treatment; clinical impact; patient safety; and quality of care.
Data Analysis
Program evaluation focused on the first 400 participants (November 2011 through May 2014) with data analyzed in 2015 to allow for a 1-year prospective follow-up for the 400th participant. Demographic, diagnostic, medication, laboratory, and clinical service utilization administrative data were gathered from the VA Corporate Data Warehouse.
Self-report health status rating scales were obtained as part of routine clinical care at intake evaluation and termination. These included the Internal State Scale 35 for manic and depressive symptoms, well-being, and perceived conflict; the AUDIT-C 36 adapted for both alcohol and drug use; the VR-12 37 for overall mental and physical quality of life; and the standardized VA assessment for risk of harm to self or others.
To characterize quality of care, we selected a priori four characteristics that were endorsed in VA clinical practice guidelines and were among the foci of our psychopharmacologic consultation: increased lithium use, decreased antidepressant use, increased prazosin use among those with comorbid post-traumatic stress disorder (PTSD), and increased lithium serum level monitoring among those taking this medication.
Two complementary sets of contrasts were of interest. First, we conducted within-group pre/post-analysis on participants for whom we were able to obtain health status self-report at intake and termination; this includes those who completed both the CVT interview and the Life Goals Self-Management Skills Program (n = 79). Second, we reasoned that some impact on psychopharmacologic strategies should result even for those who only received chart review consultation; we again used a pre/postanalytic strategy here, comparing the year before versus the year after consultation, including those who completed CVT intake and those received only a chart-review consultation (n = 379); the former group contained both those who did and did not subsequently enroll in Life Goals. Our secondary analyses compared these three groups to determine whether quality impacts were limited to one of these subgroups.
Two-group comparative data were analyzed using the t-test or χ2 test, while pre/postcomparisons were analyzed using the paired t-test, McNemar's test, or Fisher's exact test (in the context of unpaired pre–postdata). Tests of differential change over time for distinct subgroups were explored using Mantel–Haenszel tests.
Results
Treatment Engagement
Bipolar Telehealth partnered with 13 medical centers, including 9 hospital-based clinics and 6 community clinics distributed across 8 VA regional networks and 11 states. Consults per facility ranged from 2 to 153, received from a total of 129 providers (range: 1–22 consults per provider).
Participation rates were comparable to 31 or better than 32 Life Goals participation rates in facility-based bipolar CCMs. Twenty-one consults (5.3%) were discontinued for administrative reasons. Of the remaining 379 consults, 296 (78.1%) completed CVT intake and the remainder received chart review consultation through telephone. Those completing CVT assessment spent a mean of 183.7 ± 74.4 days enrolled (median 168, range 59–398).
Of 254 participants judged clinically appropriate for Life Goals self-management follow-up, 181 (71.3%) entered Life Goals. Of these, 129 (71.3%) completed the program, while 52 (28.7%) began but did not complete. Life Goals completers had a mean of 9.23 ± 3.58 CVT sessions, while noncompleters still participated in a mean of 3.75 ± 2.46 sessions.
Predictors of Program Participation
Participant demographic and clinical characteristics are summarized in Table 1, which compares those who underwent CVT evaluation and those who could or would not and received a chart review consultation only. Those who underwent CVT evaluation were significantly more likely to be married, but did not differ on a wide variety of other demographic and diagnostic characteristics. Those who underwent CVT evaluation were less likely to have been hospitalized but did not differ in other treatment experience in the prior year. Of the 254 judged appropriate for Life Goals Self-Management Program enrollment after CVT evaluation, completers (n = 129) did not differ from eligible noncompleters (n = 125) on any of the characteristics summarized in Table 1.
Baseline Demographic, Clinical, and Treatment Characteristics of First 400 Participants
Values differ at p ≤ 0.01.
Values differ at p ≤ 0.05.
Clinical Impact
Among Life Goals Self-Management Program completers for whom self-rating scales from intake and program completion were available (n = 79), significant improvements were seen in manic, depressive, and conflict symptoms, 35 as well as mental but not physical quality of life 37 (Table 2). No difference was seen in well-being self-ratings, 35 likelihood of being in any mood episode, 35 reported harm risk, or problem drinking. 36
Clinical Status at Baseline and Pre/Post-Treatment Clinical Status Among Life Goals Completers
Values differ at p ≤ 0.02.
Values differ at p ≤ 0.001.
CVT, clinical video teleconferencing; ISS, Internal State Scale.
Among all individuals completing CVT evaluation (n = 296), there was a small but nonsignificant decrease in the rate of mental health hospitalization from 1 year after evaluation based on McNemar's test (n = 71 [24.0%] to n = 61 [20.6%], p = 0.31). There were no significant differences between eligible Life Goals completers and noncompleters.
Patient Safety
There were no suicides while enrolled in Bipolar Telehealth. We learned of two suspicious (accident vs. suicide) deaths subsequent to the end of program contact: one death in an individual who was referred but did not respond to enrollment attempts and one death 3 months after CVT evaluation in an individual who wished only initial evaluation without Life Goals follow-up. There was one medical death several days after chart review consultation in a veteran who could not be enrolled in CVT evaluation.
We identified two suicide attempts during program enrollment, one despite activating the home medical center for a higher level of vigilance. There were eight occasions when program staff engaged on-site clinicians to address suicidal ideation disclosed during a CVT session, and three hospitalizations for suicidal ideation.
Quality of Care
Quality of care indices are summarized in Table 3. As predicted, among those who completed CVT evaluation (n = 296), lithium use increased in the year after CVT evaluation compared to the prior year (McNemar's test: n = 106 [35.8%] to n = 154 [52.0%], p < 0.001), while antidepressant use decreased (n = 143 [48.3%] to n = 103 [34.8%], p < 0.001). Among those with a comorbid PTSD diagnosis, prazosin use increased (n = 30 [21.9%] to n = 48 [35.0%], p = 0.02). Rates of obtaining lithium levels among those taking lithium, already high among individuals referred to our program, did not change in the subsequent year (n = 81 [76.4%] to n = 114 [75.5%], p = 0.88).
Quality of Care 1 Year Before Intake Versus 1 Year Following
McNemar's test was used to compare proportion meeting criteria 1 year before versus 1 year after consultation (paired samples) in those completing CVT evaluation (n = 296) for lithium level and prazosin use; Fisher's exact test was used because the population of lithium users and the population of those with a PTSD diagnosis changed from 1 year before to 1 year after consultation (unpaired samples).
Mantel–Haenszel test was used to identify differences in pre- versus post-consultation between those who completed CVT evaluation (n = 296) and those who received only chart review consultation (n = 83).
PTSD, post-traumatic stress disorder.
Two further analyses explored potential mechanisms for these quality enhancements. We first explored whether medication use changes applied to CVT completers only or to all individuals referred to our program (Table 3). In each case, the Mantel–Haenszel test indicated that improvements in these domains were significantly higher among CVT completers than noncompleters. We then assessed whether those among CVT completers who completed the Life Goals Self-Management Program differed from those who did not complete Life Goals. We found no significant differences in any of the four quality indicators (data not shown).
Discussion
Results in Context
These data demonstrate that CVT-based modalities can successfully utilize multicomponent CCM interventions to reach, engage, and impact health indicators for individuals with complex, chronic mental health disorders such as bipolar disorder. The program's first 400 participants came from a wide geographic area across 11 states, including small, rural community-based clinics. Notably, as demand increased, the specialty “hub” of the hub-and-spokes system expanded from one to two medical centers, demonstrating that the clinical microsystem 10 can be implemented even with a virtual center of clinical expertise.
What is known to date about telecare for serious mental health conditions? The VA has seen steady growth of CVT-based treatment for various mental health conditions since the mid-2000s, 38 with consequent reductions in hospitalizations and days hospitalized in the year after versus year before initiation of CVT-based treatment. 39 However, relatively few reports of telehealth-based interventions specifically for serious mental health conditions exist, within or outside of the VA. For PTSD, systematic review data indicate medium to large effects for telepsychotherapy of various types over short term, although enduring effects at 1–6 months are variable. 40 Multicomponent CCMs involving telephone-based supplements of on-site care have demonstrated efficacy for PTSD 41 as well as depression treated in primary care, 42,43 with one trial also providing access to CVT-based consultation. 41 We are aware of no reports of CVT-based interventions for bipolar disorder, while for schizophrenia, evaluation of technology-assisted treatment has been limited to informatics-based technologies, but not CVT. 44
Acceptability of CVT-based treatment for individuals with mental health conditions has been mixed. One study demonstrated high acceptability for low-income Hispanic women volunteering to be randomized to CVT versus in-person treatment for depression. 45 However, another study of low-income depressed individuals in the United States demonstrated that while 76% endorsed the idea of CVT-based depression treatment, only 38% made appointments and 17% attended sessions. 46 In a controlled trial of in-person versus home-CVT delivery of exposure therapy for PTSD, CVT participants reported difficulty tolerating the more stressful aspects of treatment. 47 Qualitative data on CVT-based medical consultation indicated that patients valued the increased access and less travel, but did not consider it the “best care” compared to in-person consultation. 48 Therapeutic alliance ratings by observing psychologists were lower in CVT than in in-person sessions. 49
Bipolar Telehealth Program Evaluation Across Five ATA Domains
Participation rates were at least similar to those of the facility-based face-to-face bipolar CCMs on which the intervention was based. 31,32 CVT participation was acceptable to a broad population, as analysis of predictors of participation revealed no subpopulations at risk for nonengagement.
Clinical impact can be contextualized in light of the chronicity and severity of bipolar disorder. Individuals who completed CVT evaluation and the Life Goals Self-Management Skills Program experienced significant improvements in mental quality of life as well as manic, depressive, and conflict symptoms. For context, in over a 10-year prospective follow-up, individuals with bipolar disorder spend approximately half their lives with clinically significant symptoms, accompanied by substantial psychosocial impairment. 50,51 Thus, although regression to the mean cannot be excluded without random assignment, program completion was associated with significant clinical improvement, consistent across multiple measures.
Patient safety considerations can also be viewed in context. Meta-analytic data indicate that the suicide rate in bipolar disorder exceeds the standardized mortality ratio 15-fold, 52 and the disorder is the single diagnosis most highly associated with completed suicide among veterans. 53 Not only was CVT-based consultation not associated with lapses in patient safety, the care model increased vigilance, activating the individual's home medical center staff on multiple occasions to respond to suicidal ideation; this enhanced response may have contributed to the lack of reduction in hospitalizations in the year before versus after consultation. Although there were no suicides during program enrollment, two suicide attempts were identified. We cannot calculate an accurate event rate with so few suicide attempts and an inexact person-year denominator for follow-up. However, using the mean follow-up of 183.7 days for 129 Life Goals completers plus 52 Life Goals noncompleters, we can estimate the duration of follow-up as (183.7/365) × 181 = 91.1 person-years, yielding a suicide attempt rate during Bipolar Telehealth enrollment of 2.2% per year. In comparison, summary data from a large number of naturalistic follow-up studies of unselected populations with bipolar disorder estimate the suicide attempt rate at 2% per year. 54 Thus, it is perhaps surprising that there were not more suicide attempt rates among participants since they were, by definition, sufficiently complex or unstable that they were referred for specialty care.
Broad-based improvements in quality of care indices were seen in the year after Bipolar Telehealth evaluation, and it is difficult to ascribe these improvements to regression to the mean or secular trends. Lithium use is highly evidence based, and stands alone among antimanic agents as having antidepressant 55 and antisuicidal effects. 56 However, rates of use have been low and have continued to drop over recent years, 57 likely, in part, due to the relatively narrow therapeutic-toxic window and the need for careful monitoring in comparison to other agents. Nonetheless, lithium use increased 45.3% in the year after Bipolar Telehealth consultation. In addition, antidepressant use, which can cause manic episodes and is recommended for sparing use in most guidelines, dropped 28.0%, while prazosin use in individuals with comorbid PTSD increased 59.8%. Thus, it is likely that Bipolar Telehealth enrollment had impact on the clinical care of enrollees. Moreover, because this program was evaluated outside of the confines of a formal randomized controlled trial, these data provide a needed extension of the existing literature. 29
Limitations
The impact of CVT implementation of the bipolar CCM cannot be determined assuredly without a randomized controlled trial. Regression to the mean for particularly symptomatic individuals, secular trends, random changes in clinical course, incomplete ascertainment of events, and confounding by indication cannot be ruled out. Assessments were not blinded, but self-reports were used to minimize the risk of interviewer bias. In an exploratory program evaluation such as this one, correction for multiple comparisons is less critical than in a scientific study seeking to disprove a hypothesis, although we can conclude only that the program appeared to be widely accepted and associated with a broad spectrum of improvements in health status and quality of care.
Conclusions and Future Directions
The Bipolar Telehealth experience indicates that CVT-based modalities can be utilized to implement multicomponent CCM treatment to reach, enroll, and impact the clinical course of individuals with severe mental health conditions such as bipolar disorder. The program had beneficial effects across four prespecified ATA domains: patient engagement, participation in treatment, clinical impact, and quality of care. Thus, these data support the use of CVT modalities for complex mental health populations requiring complex treatment models such as CCMs to maximize health outcome.
While randomized clinical trials will always be useful in further defining effects of clinical interventions, the beneficial effects of Bipolar Telehealth broadly align with results of earlier randomized controlled trials of the facility-based bipolar CCM on which the program is based.
31,32
It would be more informative at this point to focus attention on the following: • Extension of videoconference-based CCMs to other serious mental health conditions, • Investigation of the barriers and facilitators to broad implementation
58
of such CVT-based models, and • Evaluation of the business case for their deployment and sustainability in clinical practice.
Footnotes
Acknowledgments
Although this work was funded by the U.S. Department of Veterans Affairs, the views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the U.S. Government. The authors appreciate the comments of Eric Smith, MD, MPH, on a prior version of this article. This work was supported by clinical funds from the U.S. Department of Veterans Affairs and VA Health Services Research and Development center grant #CIN-13-403 and VA Quality Enhancement Research Initiative grant #QUE-15-289.
Disclosure Statement
Dr. Bauer receives royalties from Springer Publishing and New Harbinger Publishing for work related to the collaborative chronic care model for bipolar disorders. No other authors report conflicting interests. This work was supported by clinical funds from the Department of Veterans Affairs Office of Telehealth Services. Dr. Bauer receives royalties on publications based on the Life Goals model from New Harbinger and Springer. Other authors have no disclosures.