
Abstract
Introduction
Increasingly across the United States, where an individual lives can often determine their level of access to healthcare. Currently, 49% of the 3,107 counties in the United States, in which 9.5 million Americans reside, do not have a single obstetrician/gynecologist. 1 This is especially true in rural states, where access to specialty care is limited due to the lack of tertiary care centers and the distance that patients are required to travel to obtain routine recommended healthcare, such as obstetrical or gynecological care. The Health Resources and Services Administration's Office of Rural Health Policy found that only 10% of the country's doctors work in rural areas despite the fact that 25% of the nation's population lives in rural areas. 2,3 In addition, there are only 40.1 specialists per 100,000 rural residents compared to the 134.1 specialists per 100,000 urban residents. 2,3 In Arkansas, 63 of the state's 75 counties have been classified as nonmetropolitan, according to the 2000 census. Furthermore, 51% of Arkansans lived in a nonmetropolitan county compared to only 20% of people living in nonmetropolitan counties in the nation as a whole. 4 As a result, rural patients' access to specialty gynecologic care, such as colposcopy, is severely limited.
Despite widespread screening through Pap smears and the reduction of cervical cancer in the United States, the rural South continues to show elevated incidence of cervical cancer and elevated mortality rates related to cervical cancer. 5,6 From 2007 through 2011, the South had the highest incidence rate of cervical cancer cases at 8.5 per 100,000 women compared to the national incidence rate of 7.5 per 100,000 women. During the same time period, the South also had the highest mortality rate for cervical cancer at 2.7 per 100,000 women compared to the national mortality rate of 2.3 per 100,000 women. 6 Based on data from 2013, which are the most current, Arkansas has a mortality rate for cervical cancer of 2.4 per 100,000 women, and it has an incidence rate of cervical cancer of 7.5 per 100,000 women based on the most current data, which are from 2011. 7 Many disparities exist in rural areas that can compound risk factors leading to cervical cancer for these women. Specifically, there are demographic disparities, including low socioeconomic status 5 and low level of education. Also, there are health-related disparities, which include lower screening rates, lower rates of follow-up for abnormal test results, lack of health insurance, and lack of access to proper screening or treatment. 5 In addition, there are geographical factors, including greater travel distance 5 to trained healthcare providers. Finally, many rural women may not be informed about appropriate resources that are available to them to help reduce the problems related to seeking care. 8 One option to help reduce the burden of seeking care for cervical cancer is the use of telecolposcopy.
Telemedicine has been used widely in rural populations as a strategy to help reduce patient costs and improve access. 9 Research has demonstrated that removing geographic barriers to care improves both access to care and outcomes. 10,11 Among various solutions proposed to help with this problem, telemedicine has been shown to be a viable technique for improving geographic access to care and has demonstrated both improved access to multiple medical specialties and a willing acceptance by patients. 1 In a survey of 2,329 women attending the University of Arkansas for Medical Sciences (UAMS) regarding their ability and willingness to seek care if it was not available in their hometown for cervical cancer screening, 14.6% would defer for 1 month, 9.7% for 3 months, 14.5% for 6 months, 16.1% for 12 months, and 29.3% would not seek care. This survey helped validate that when rural patients face barriers to their healthcare, they often defer their needed care due to those barriers. 8
To meet the needs of at-risk women throughout the state of Arkansas, a collaborative pilot project involving UAMS and the Arkansas Department of Health began in 2006 utilizing telecolposcopy for impoverished women requiring this service. This study found that over a 17-month period the program had scheduled 1,812 visits and performed 1,298 colposcopic examinations from patients in 68 of the 75 counties in Arkansas. This pilot study proved to be very successful and has resulted in successful grant applications and an expansion of the project to eight distant spoke sites. 10 The start-up costs associated for this project were $44,000 per site or $352,000 for all eight spoke sites. This included a telemedicine cart ($18,000 per unit), a colposcopy machine ($6,000 per unit), instruments used for colposcopy examinations ($16,000 per site), and an autoclave ($4,000 per unit). Additional costs can be incurred such as clinic personnel time spent at both the spoke site and UAMS, clinical space to perform the procedures, and other supplies. These costs can vary depending on the number of personnel available and resources that are already available depending on the spoke site and/or organization. Although the telecolposcopy service is growing and expanding, a comprehensive cost savings of the telemedicine service versus the traditional face-to-face service at the University clinics have not been evaluated. In general, cost analysis studies of telemedicine services have been inconclusive 10 and this study aims to contribute to the body of literature that evaluates patients' access to care based on travel time and transportation costs. The purpose of this study was to describe patients utilizing this program and to review the accessibility to care and its impact related to the use of a telecolposcopy.
Materials and Methods
Women from rural sites in Arkansas who had an abnormal Pap test or abnormal visual examination and who needed further evaluation by colposcopy with possible biopsy were referred to a telecolposcopy program at UAMS located in central Arkansas. The program began in 2006 and is still active, currently having scheduled more than 11,000 patients within the state of Arkansas from all 75 counties. In 2014, an Access database was created to improve data quality and management. The Access database contains all information regarding patient demographics, referral county, colposcopy site, Pap smear result, sexual history, smoking history, and whether or not the patient had the GARDASIL shot series. For the purpose of this article, only information collected in the Access database will be discussed and analyzed.
Results
From January 2014 through April 2015, a total of 940 unique patients were seen using telecolposcopy at UAMS. Some patients may have had multiple visits during this time period, but only one of their visits, usually the most recent visit, was included in the analyses. Data from an earlier visit were only included if data were missing from the most recent visit. Telecolposcopy was performed at eight remote (spoke) sites, located at County Health Units, which in this sample served patients from 72 of the 75 Arkansas counties. Patients ranged from 17 to 62 years of age with a mean age of 28.9 ± 6.26. Most of the patients seen were Caucasian with the largest number referred from Pulaski County. Figure 1 shows the frequencies of referrals from each county in Arkansas. Of the eight spoke sites, the highest volume of patients was seen at the Hempstead County (20%) and Lonoke County (20%) sites. Table 1 lists the top referral counties by number of patients referred and by percentage. Some of the counties listed reported the same frequencies; therefore, more than one county may be listed for a given ranking. In addition, four of the counties listed with the highest referral volume represented counties in which spoke sites were located. However, while the Lonoke County spoke site was one of the busiest sites, Lonoke County was not listed as a top referral county. This is attributed to the fact that patients attending the Lonoke County site were referred mostly from other busier counties such as Pulaski County.
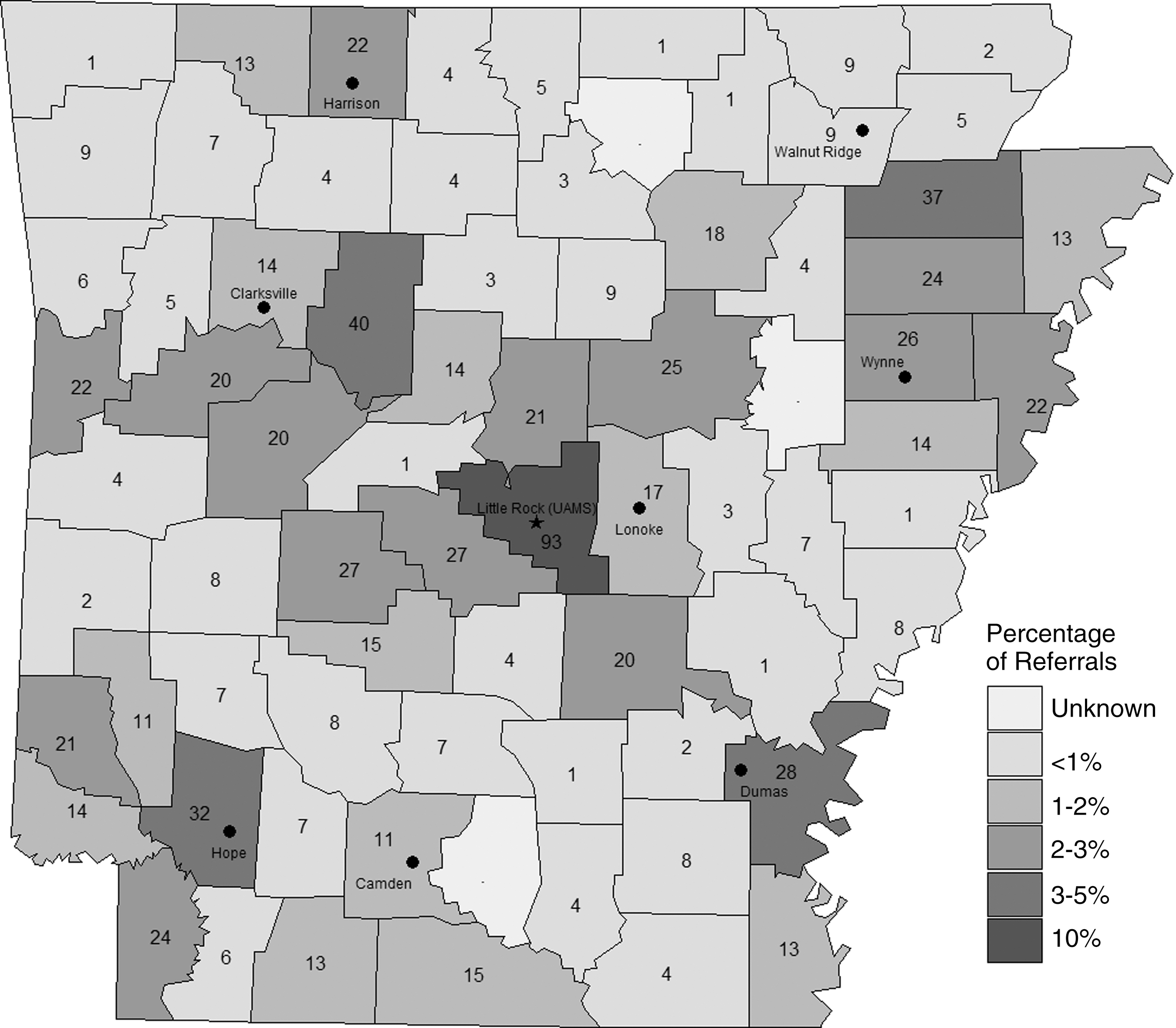
Map of referrals per county.
Top 10 Frequencies for Referral Counties
Counties where a spoke telecolposcopy site is located.
Both these counties reported the same number of referrals.
Before each visit, a patient survey addressing risk factors for developing cervical cancer was administered and found that most of the patients were nonsmokers (61% vs. 39%). Among patients who reported being smokers, the average daily use was 11.4 ± 6.60 cigarettes, and the average number of years of smoking was 10.0 ± 6.54. Questions regarding sexual history were asked as well with the average age of first sexual experience being 16.2 ± 2.47, the average number of partners in a lifetime being 8.4 ± 9.19, and the average number of partners in the last 12 months being 1.5 ± 1.81. Finally, patients were asked about whether or not they had received any of the GARDASIL shot series. Most women reported that they never received the shot(s) (88%), followed by 12% that reported they had at least one out of the three GARDASIL shots, and there was one patient who reported that she was not aware of whether or not she had been vaccinated.
Patients were referred initially with abnormal screening Pap smears. The most common abnormal Pap results referred for telecolposcopy were as follows: low-grade squamous intraepithelial lesion accounted for 58.0% of the patients, followed by atypical squamous cells of undetermined significance at 13.1%, and then by atypical squamous cells that cannot exclude high-grade lesion at 12.9%. Pap smears showing high-grade squamous intraepithelial lesion made up 7.8%, while atypical glandular cells were reported in 4.7% of the patients referred. Finally, patients referred with normal Pap smears made up 3.5% of the referrals.
After being seen through telecolposcopy, each patient was given an impression based on the assessment by the hub-site clinician. Over half of the impressions were identified as low-grade lesion (51.0%). This was followed by high-grade lesion (24.4%) and benign (23.7%). A very small percentage of impressions were listed as cancer or cervicitis (0.64%) followed by polyps (0.22%). Compared to the biopsy results, the most common diagnosis was cervical intraepithelial neoplasia I (40.1%), followed by benign (29.4%), cervical intraepithelial neoplasia II, cervical intraepithelial neoplasia III and carcinoma in situ (18.1%), atypia (0.52%), and cancer (0.13%). A total of 11.4% of the patients did not have a biopsy, and 0.39% had a biopsy, but with an inadequate sample.
Finally, we considered the transportation cost and travel time for a patient to drive from her home county to UAMS, which is a cost and a loss of time that can be avoided for a patient since a telecolposcopy program is available. If the telecolposcopy services did not exist, going to UAMS would have been the only other option for patients in seeking care within Arkansas. The transportation cost and travel time were computed for each of the 75 Arkansas counties. The per-patient transportation cost associated with each county was calculated assuming a gas mileage of 22 miles per gallon (mpg) and a gasoline price of $3.36 per gallon, based on price estimates of regular gasoline from 2014. 12 The driving distance, not the Euclidean distance, was measured in miles from the centroid of the most densely populated zip code in the most populous city in each referral county to the centroid of the zip code for UAMS. To determine the round-trip per-patient transportation cost from the referral county to UAMS, the driving distance in miles was divided by mpg; then the resulting number of gallons was multiplied by cost per gallon of gas; and then the resulting one-way cost was doubled. Following these computations, the minimum, median, and maximum round-trip per-patient transportation costs were obtained and were $6.75, $32.68, and $65.67, respectively. The mean cost was $33.25 ± $13.15. In addition to potential cost savings from not having to travel to UAMS, patients would possibly save time. For the 75 Arkansas counties, the minimum driving distance to UAMS is about 22 miles, which corresponds to Pulaski County and less than 0.5 h of travel time, while the maximum driving distance to UAMS is about 215 miles, corresponding to travel from Benton County and more than 3 h of travel time. The median and mean driving distances to UAMS are about 107 and 109 ± 43.0 miles, respectively, corresponding to less than 2 h of travel time.
Discussion
Cervical cancer screening and diagnosis (colposcopy) is an important public health concern. Broad adoption of cervical cancer screening has coincided with a 60–70% reduction in the incidence of cervical cancer. However, underserved portions of the population still exist. 13 The lack of adequate cervical cancer screening is frequently noted by newly diagnosed cervical cancer patients. For women diagnosed with cervical cancer or present with abnormal screening results, especially those of racial/ethnic minorities, a large number do not receive follow-up care or treatment. 14,15 A variety of barriers to access contribute to this problem and include lack of health insurance, low income, 16 limited knowledge or trust in the medical system, 17 and low self-efficacy, especially in populations with limited health literacy. 18 A study by Laedtke and Dignan 19 found that women referred for follow-up after an abnormal screening were less likely to follow-up if they traveled longer distances. The availability of healthcare services near patients in need is a factor in the success rate of cervical cancer screening. One effective acceptable method of providing cervical cancer screening to those with limited access, including rural settings, is through telecolposcopy. Numerous factors make rural telecolposcopy a more affordable alternative to in-person visits.
In general, healthcare costs in the United States are higher than in any other developed country. 20 As a result, practitioners and policy makers must examine the value of our healthcare delivery system if we are going to adequately care for all people. In addition, we must consider the cost to the patient to access the healthcare facility. This could include but is not limited to the cost of gas, distance traveled, potential loss of work hours, and potentially relying on alternate family members to accompany the patient to the visit and/or to provide childcare. While this program did not collect specific information from the patients to determine the cost-effectiveness, we were able to compute cost avoidance based on travel time for each county in Arkansas.
We were able to demonstrate that this program has provided some sustainability statewide since its inception in 2006 and that patients are willing to participate in this telehealth program. In the current study, we were successful in reaching patients across the majority of the counties in the state to perform telecolposcopy at the eight remote (spoke) sites. However, of the 940 unique patients, 10 patients did not have referral county information available due to missing data elements. Therefore, we cannot determine whether these patients came from the 3 counties not represented in the data or from the 72 counties that were represented in the analysis. As a result, we are unable to accurately report on demographical information for these three counties and the reason for this absence can be attributed to missing data elements.
While this article focused on patients that were referred and sought care over a 15-month time period from January 2014 to April 2015, this time period coincided with the publication of new practice guidelines regarding cervical cancer screening and referral of abnormal results released in March 2012. In essence, these guidelines recommend less frequent screening and fewer abnormal results requiring referral for colposcopy. As a result of these changes, the overall number of patients referred to the program decreased from earlier years. Even though guideline changes attributed to a decrease in the number of referrals, the program has still proven to be successful in increasing access, patient compliance, and availability of resources that may not have been otherwise available. The implementation of this program indicates that colposcopy services can be accomplished in a rural state with limited healthcare resources. The cost savings of a rural telecolposcopy program should be considered as healthcare communities strive to maximize effectiveness of cervical cancer programs.
Footnotes
Acknowledgments
The authors acknowledge Shirley Anthony for data gathering and data entry and Amit Saha for database design and review. This project was funded by the Health Resources and Services Administration's Office for the Advancement of Telemedicine (1 H2AIT16616 and 6 H2ARH24765-02-01).
Disclosure Statement
No competing financial interests exist.