
Abstract
Introduction
Cell phones are now integrated into everyday life, with nearly three-quarters of the population worldwide routinely utilizing mobile health (m-health) technology. 1 Nearly 90% of adults in the United States have a cell phone; and 98% of cell phones have short message service (SMS) text messaging (TMs) capability. 1,2 TMs are becoming an easy-to-use, inexpensive means of delivering behavioral interventions to improve health outcomes. 2 –4 However, limited evidence is available on who will use these TM interventions and how to best screen and approach patients for participation in trials of TM interventions.
Such evidence is needed in cancer care due to the steady increase in the number of cancer cases diagnosed annually; and by 2030, cancer will surpass heart disease as the leading cause of death in the United States. 5 TM interventions have been shown to improve self-efficacy and depressive symptoms in various populations. 6,7 Evidence to date of TM interventions in cancer supports improvement in health outcomes such as obtaining a mammogram, medication adherence, regular physical activity, and proper nutrition. 8 –10 One study found a 95% response to TMs for medication adherence. 9 Testing TM interventions in cancer populations is highly significant, and the first important question is patients' willingness and ability to participate in trials of these interventions.
Enrollment in research using mobile phones, particularly in those who are older than 50 years with comorbidities, is understudied. Those 65 or older comprised 59% of cancer patient population 11 and many of these patients are treated with oral anticancer agents. Cancer treatment in pill form is estimated to be 25% of all treatment and growing exponentially. 12 This shift in the treatment paradigm results in patients being seen less in cancer clinics and taking medication at home. Thus, a need exists to help those with cancer treatment in pill form to have interventions like TMs to assist with medication adherence and symptom management.
The implication for trials that TM interventions among cancer patients treated with oral anticancer agents is that the window of opportunity for approaching patients in physicians' office becomes narrower. Thus, to ensure generalizability of findings from modern trials to broader populations, cancer patients need to be approached in settings other than physicians' offices, using methods that are different from the traditional face-to-face approach. One such setting is specialty pharmacies that dispensed $87 billion in cancer medications in 2012, with estimated costs quadrupling to $400 billion by 2020. 13
Therefore, the purpose of this study was to report findings regarding enrollment of adults with cancer in a TM trial to improve health behavior outcomes. The objectives were to (1) report on the acceptability of a TM intervention in adults with cancer; (2) examine characteristics and health status of adult cancer patients, prescribed an oral anticancer agent, screened and enrolled in a TM intervention trial to support medication adherence; and (3) compare recruitment settings (specialty pharmacy versus community-based cancer clinics).
Materials and Methods
Study Design
This was a secondary data analysis. Screening and baseline data are from two randomized controlled trials deploying a TM intervention.
Sample
The two trials shared the same eligibility criteria: 21 years of age or older, prescribed an oral anticancer agent for cancer treatment, owned a personal cell phone, and able and willing to receive and send a TM. Patients also had to be able to speak, read, and understand English. Those with cognitive impairment that limited the ability to understand and answer questions were excluded, as evaluated by the recruiters at the specialty pharmacy and cancer clinics. In total, between the two trials, 462 individuals were screened; 248 of those were eligible and 161 consented and were enrolled.
Setting
Screening occurred at a large national specialty pharmacy and five community-based cancer clinics between July 2013 and October 2014. Specialty pharmacies focus on high cost, complex medication therapy for patients with diseases such as cancer, multiple sclerosis, and rheumatoid arthritis to rare genetic conditions. 14 Medications in specialty pharmacy range from oral to cutting edge injectable and biologic products. The cancer clinics consisted of physician offices where doctors who specialize in treating cancer oversee care and treatment. 15 One of the cancer clinics was a National Cancer Institute (NCI) designated Cancer Center. 16 All sites were in the United States.
Original Study Procedures
The original studies include two randomized controlled trials funded by the NCI (N = 75) and the McKesson Foundation (N = 80). Following consent, baseline data were collected through telephone interviews. Patients were randomized to receive either a TM intervention timed to their medication regimen for 21–28 days (one oral anticancer agent cycle) to promote medication adherence to oral anticancer agent or symptom management, or usual care in a control group. The conceptual approach was guided by the principles of Self-Efficacy Theory. 17 We hypothesized that engaging patients through TMs would heighten attention to concentrate on tasks and improving self-efficacy would support task completion (i.e., medication adherence to the OA or use of symptom management strategies). Findings are published elsewhere. 18,19
Measures
Baseline data were collected on characteristics (age, sex, race, and ethnicity), employment status, and level of education. The presence of 10 of the most commonly occurring comorbid conditions was assessed. With regard to cancer, the cancer type and stage, and days since the oral anticancer agent treatment started were collected. Data on the complexity of the oral anticancer agent treatment, simple (once daily dosage) or complex (multiple dosages or cycling on and off the medication), were also examined.
Cognition was assessed using the Cimprich Attentional Function Inventory, which is scored from not at all to extremely well. 20 Three constructs were examined using subscales in the instrument: effective action, attentional lapses, and interpersonal effectiveness, with internal consistency reliability of 0.95.
Self-efficacy for medication taking or barriers was assessed. The Medication Adherence Self-efficacy Scale (MASES-R) (Cronbach's α 0.92) 21 was used. In addition, the Beliefs about Medication Questionnaire (BMQ, specific part) with two subscales, (1) beliefs about the necessity of medication (higher score indicating higher perceived necessity) and (2) concerns about medication (higher score reflecting more concerns) (Cronbach's α 0.77), was used. 22
Social support was also assessed. The Medication Specific Social Support (MSSS) tool (Cronbach's α 0.79) was used. 23
Symptom severity and interference of 19 symptoms commonly experienced from side-effects of oral anticancer agent treatment. The Symptom Inventory was used to examine the presence, yes or no, severity on a scale of 1 to 9, with 9 being the most severe, and interference on a scale of 0 to 9, with 9 being the worst. 24 Alpha coefficients are 0.72 and 0.78 for the number and severity subscales, respectively.
Patient Reported Outcome Measurement Information System (PROMIS) tools (
Procedures
Protocols were reviewed and approved by the Institutional Review Board at the University and clinic sites. The initial patient screening for eligibility criteria of age and current oral anticancer agent prescription were completed based on medical records at the clinics or prescription records at the specialty pharmacy. The rest of the eligibility criteria, such as having a cell phone and willingness to send and receive text messages, could not be verified through medical or pharmacy records; thus, patients were approached to verify the remainder of eligibility requirements. At the cancer clinics, after the initial screening of medical records, the trained recruiters, who were nurses or physician assistants, approached patients face-to-face, explained the study, and obtained informed consent from eligible patients who were willing to participate. At the specialty pharmacy, after the initial screening of pharmacy records, patients were either called on the phone or were sent a letter. For those called on the phone, the trained recruiter, who were pharmacists or pharmacy technicians, explained the study and obtained informed consent by means of an electronic e-mail signature. For those who had a letter sent to their home, the letter explained the study, and a consent form was enclosed with an addressed and stamped return envelope to mail the signed consent form back to the specialty pharmacy if willing to participate.
Signed consents and completed enrollment forms (name, phone number, drug regimen, oncologist, preferred contact time) were faxed to the University by the recruitment sites. Following consent, trained interviewers at the university contacted patients through phone to conduct the baseline interviews. Enrollment and baseline interview data were compiled in the PROMIS Assessment Center Data Collection Platform. 26
Statistical Methods
SAS 9.4 was used for analysis. Descriptive statistics were computed to evaluate the distributions of data collected at screening and baseline. Chi-square or Fisher's exact tests were used to examine the differences according to the recruitment setting for categorical variables and t-tests were used to examine differences for continuous variables. To further investigate the differences observed in recruitment setting, generalized multivariable linear models were used.
Results
The numbers of screened, eligible, and consented participants, reasons for ineligibility and nonenrollment, and attrition at baseline interview at the specialty pharmacy are shown in Figure 1 and in Figure 2 for the cancer clinics. The specialty pharmacy screened 169 individuals, while the cancer clinics screened 293. Of those screened, 72% at the specialty pharmacy were eligible compared to 43% at cancer clinics. Of those eligible for the trials, 74% at the specialty pharmacy and 56% at the cancer clinics chose to participate and consented. Ineligibility rates due to the lack of cell phone ownership or inability to send and receive TMs were more than two times higher among patients approached in cancer clinics compared to patients approached by the specialty pharmacy.
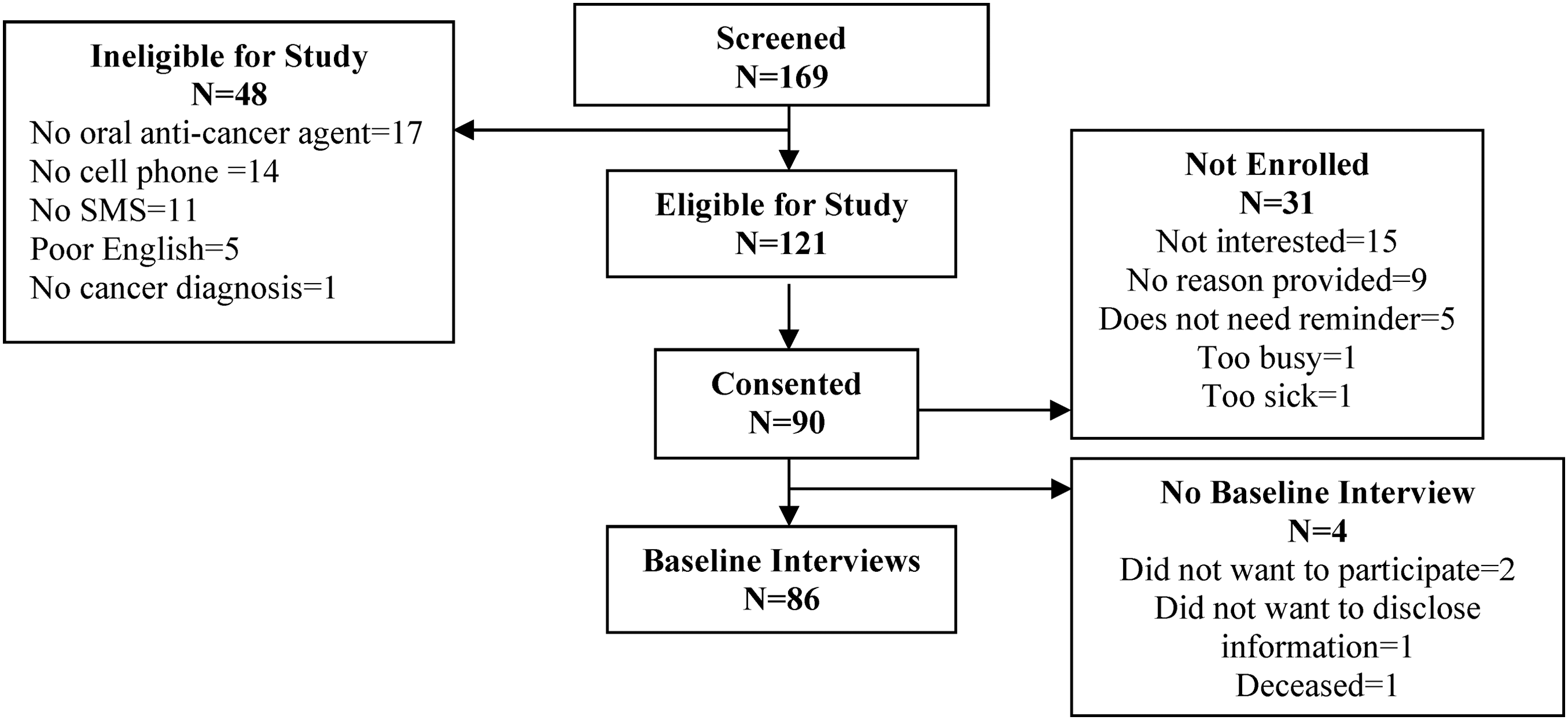
CONSORT chart of patients screened, eligible, and enrolled at the specialty pharmacy.
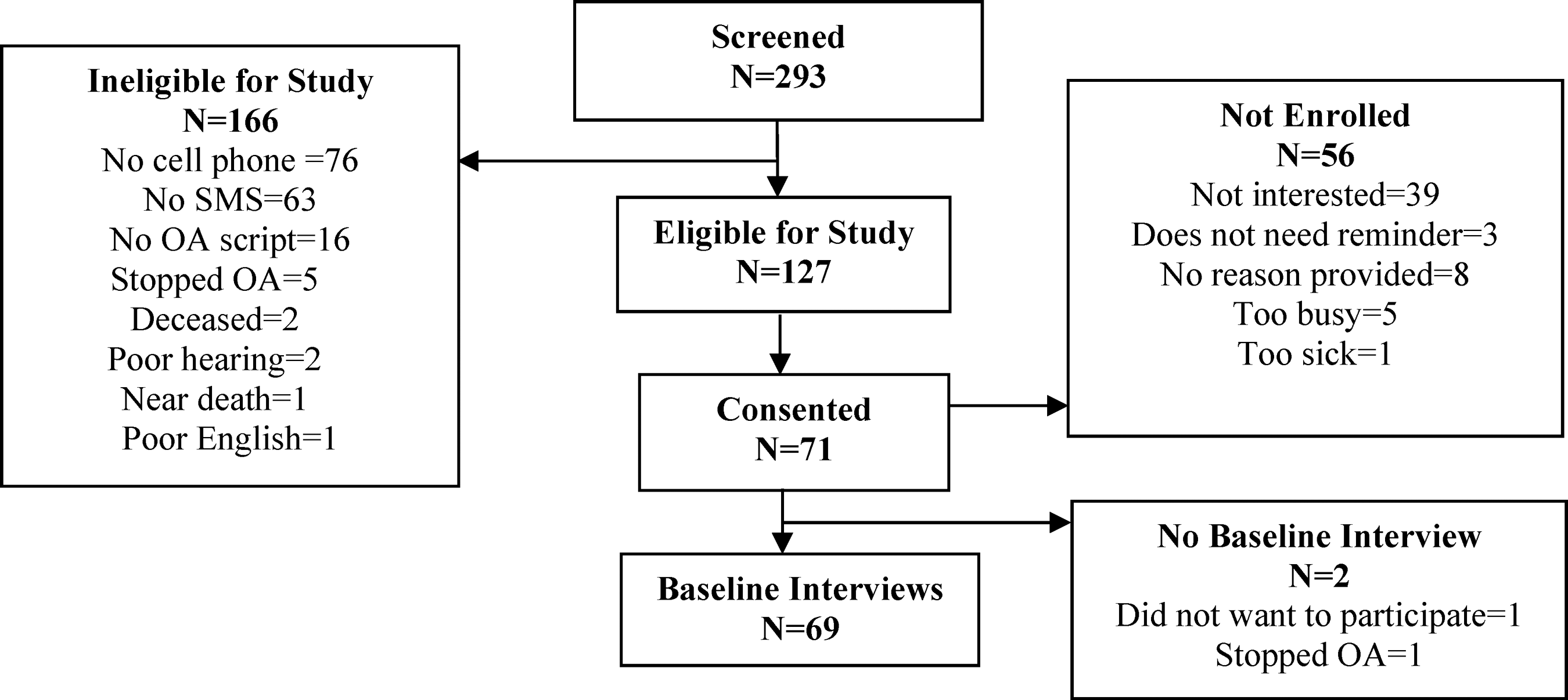
CONSORT chart of patients screened, eligible, and enrolled at the National Comprehensive Cancer Center and the Community Cancer Centers.
Reasons for not enrolling in the trials are shown in the figures. Lack of interest in the study was cited as reason for not enrolling by 23% of the eligible patients at the cancer clinics compared to 12% at the specialty pharmacy. In both recruitment settings, less than 5% of eligible patients refused participation due to being too sick or too busy. Also, less than 5% stated they did not need medication reminders.
Group differences were examined between the specialty pharmacy and cancer clinics. Table 1 summarizes the characteristics of those who completed baseline interviews. Average age was 60.25 ± 10.68 in the specialty pharmacy group and 57.85 ± 10.44 in the cancer clinics, with no difference found between recruitment settings (p = 0.17). There were also no differences by sex, ethnicity, or employment status. A higher percentage of African Americans were recruited at the specialty pharmacy, 16.47% compared to 2.94% in the cancer clinics (p = 0.02). The specialty pharmacy group was more educated (some college/bachelor degree 60–44.12%; p = 0.02). No differences in the prevalence of specific comorbid conditions were found between recruitment settings nor when the total number of comorbidities for each patient was counted (p = 0.91).
Sociodemographic Characteristics and Factors Examined in Study
Due to small numbers, comparisons of proportions among category were carried out using Fisher's exact test.
Data are presented as mean ± SD, n (%).
BMQ, Beliefs about Medication Questionnaire; COPD, chronic obstructive pulmonary disease; MASES-R, Medication Adherence Self-efficacy Scale; PROMIS, Patient Reported Outcome Measurement Information System.
Over 20 types of cancer were represented in the sample, reflective of broad use of oral anticancer agents. A higher frequency of renal, pancreatic, and prostate cancer (p = 0.01) and later stage (IV) cancer (p = 0.01) was found among patients recruited at the specialty pharmacy. Twenty-eight different oral anticancer agents were prescribed, with no difference in regimen complexity (simple daily doses: 42.35% compared to 47.76%; and twice a day, cycling, or multiple complex doses: 57.65% compared to 52.24%) among the cancer clinics and the specialty pharmacy. Days since start of the medication to date of baseline interview were higher in the cancer clinic group, but due to high variability, the difference was not statistically significant (p = 0.12).
Patients recruited at the specialty pharmacy reported a higher total number of symptoms (6.23 ± 3.51 to 4.68 ± 2.92; p ≤ .01) as well as summed symptom severity (32.75 ± 24.66 to 24.05 ± 16.94; p = 0.02) and summed symptom interference (25.1 ± 22.59 to 17.43 ± 15.78; p = 0.01). The difference in the number of symptoms remained significant in the general linear model that controlled for age, number of comorbid conditions, days since medication start, and oral agent regimen complexity. The differences in symptom severity and interference between recruitment settings were no longer significant after adjusting for the above covariates. No group differences were found for depression, physical function, or cognition nor were differences found in the beliefs about medications, self-efficacy, or social support.
Discussion
Our findings indicate that adults (mean age older than 50 years) of both sexes with multiple comorbid conditions were willing to enroll in an intervention using m-health cell phone TM technology to promote medication adherence when prescribed an oral anticancer agent. A novel recruitment method through the specialty pharmacy reached a more diverse population with higher percentage of African Americans compared to the traditional recruitment in the cancer clinics. The specialty pharmacy sample was also more educated compared to the sample enrolled in cancer clinics, possibly because patients with a lower level of education responded better to face-to-face recruitment. Through the specialty pharmacy, the study was also able to reach the population with higher use of cell phones and TMs and with greater interest for the trials using TM interventions. For the most part, a low percent of those who stated that they did not need medication reminders points to the need of interventions to promote adherence to treatment regimens. TM may be a particularly significant way to deliver such interventions in the multimorbid population of adult cancer patients.
Healthcare professionals often have difficulty helping patients change their behaviors, specifically with regard to medication adherence. Literature indicates that health behavior change interventions may be more successful if initiated earlier in treatment. 27 In the case of oral anticancer medications, TM reminder interventions may potentially improve medication adherence and would be most beneficial if initiated close to the start date of a new medication regimen. At the specialty pharmacy, we were able to enroll patients closer to the start date of the medication, which may be an important factor for the success in behavior change to promote adherence. Also, through timely initiation of supportive care interventions, symptoms and side-effects from oral anticancer medications can be managed closer to their onset, which would improve the patient's quality of life during treatment. However, it is possible that those recruited at the specialty pharmacy were not representative of the larger population of adults with cancer.
Limitations
Our study has several limitations. In the most part, self-reported data were used, which have known accuracy limitations. Furthermore, we focused our work in cancer patients, and other populations may have different rates of use of TMs. Future research should examine recruitment setting differences across various populations. Recruitment at the cancer clinics was in person, while recruitment at the specialty pharmacy was by phone or letter, which may have introduced a confounding factor. We acknowledge this limitation as no opportunity exists for face-to-face recruitment in clinical trials at large national specialty pharmacies.
Nonadherence to treatment and medication regimens is a global problem, 28 and innovative means of addressing this significant clinical problem are needed to improve population health outcomes. If future studies replicate our findings, a question of pressing concern will be whether TM interventions focused on adherence to treatment regimens enhance self-efficacy, reduce depressive symptoms, and improve individual actions to adhere with lasting habit formation. Results from such studies may reveal innovative ways of improving health behaviors and the health of the aging society.
Footnotes
Acknowledgments
The authors acknowledge and thank the cancer patients who participated in their study and the clinicians at the specialty pharmacy and community cancer centers for their support of the study and assistance during participant recruitment. This research was supported by grants entitled Text Messaging to Improve Symptom Management and Adherence to Oral Chemotherapy Agents from the McKesson Foundation, Inc., Mobilizing for Health Grant Program, in San Francisco, California, and Text Messaging to Improve Adherence to Oral Chemotherapy Agents from the National Cancer Institute (Grant Number 1R15CA176595).
Contribution to Science Advancing Research
This article reports on recruitment of cancer patients from different settings into m-health cell phone text message intervention trials to inform the efforts of reaching diverse patient populations in future research studies.
Disclosure Statement
No competing financial interests exist.