
Abstract
Introduction
Tele-stroke is the use of telemedicine to provide acute stroke care on an emergent basis, specifically for administering intravenous tissue plasminogen activator (IVtPA). 1 Although the adoption of tele-stroke is known to increase the rates of IVtPA, 2,3 the effects on timeliness of IVtPA delivery is less clear.
Methods
The Rush tele-stroke program began in March 2011 and consists of an academic comprehensive stroke center hub that serves a regional network of 10 community spoke hospital emergency rooms (ERs) (Fig. 1). Rush tele-stroke program includes stroke consultation through bidirectional audiovisual communications provided by In Touch Health, Santa Barbara, California, standardized acute protocols shared with all spoke ERs, and formal feedback on quality assurance performance measures. A patient identified with stroke symptoms in the ERs leads to a “stroke code” activation. Once CT brain excludes intracerebral hemorrhage, the Rush tele-stroke phone line is called to initiate the consultation. The tele-stroke physician is an attending board-certified vascular neurologist and is privileged at all hospital spoke sites, with access to the local hospital's electronic medical charting and picture archiving and communication system neuroimaging. If a recommendation is made for treatment, IVtPA is administered at the spoke hospital according to the local institutional IVtPA protocol.
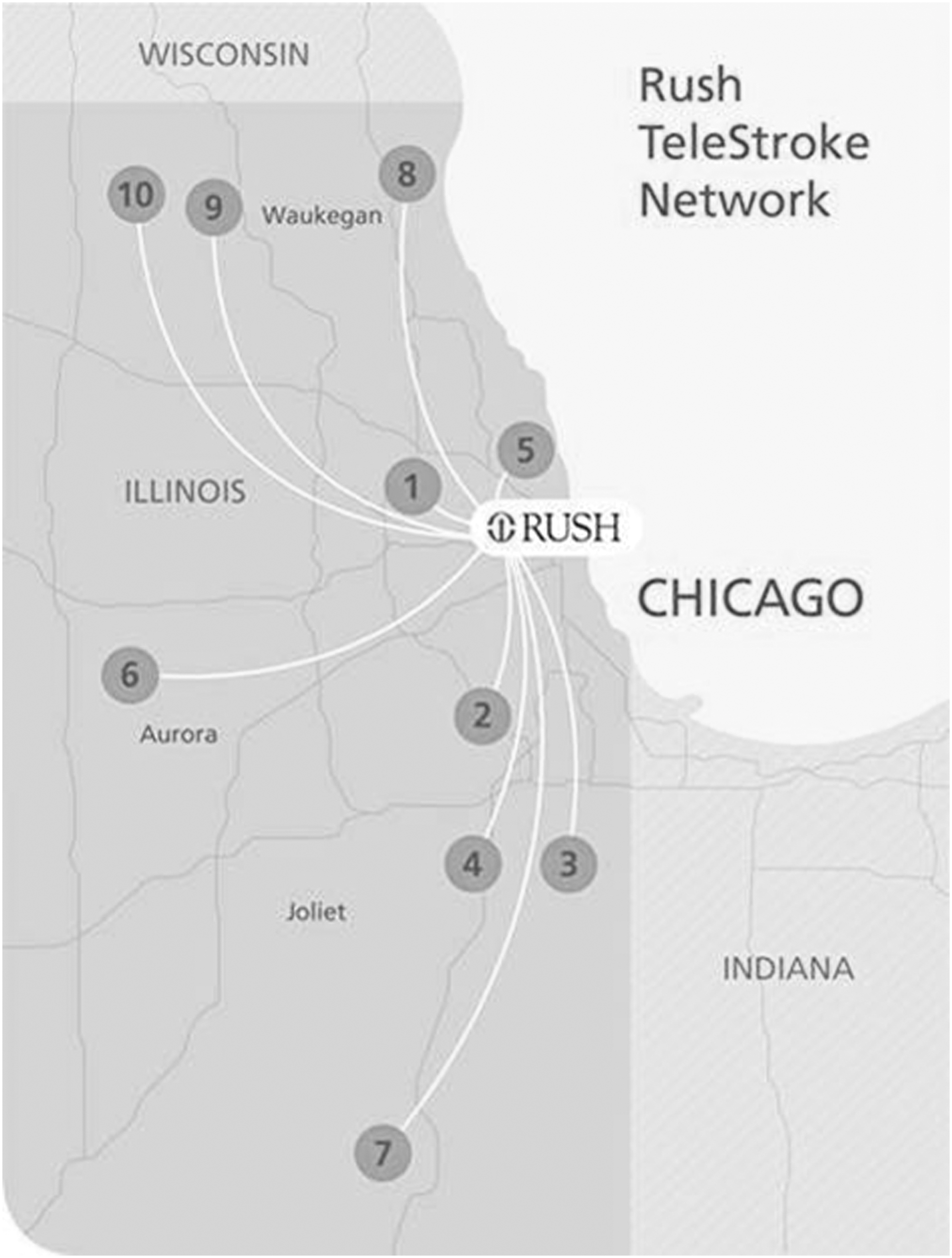
Map of Rush tele-stroke program. The distances of the hospital spoke sites range from 7.8 miles (hospital 1) to 61.8 miles (hospital 7).
We retrospectively reviewed acute ischemic stroke patients treated with IVtPA through the Rush tele-stroke program. Only eight ERs were included in the analysis, as hospital sites 9 and 10 recently joined the network (Fig. 1). We compared two cohorts of patients: Period 1 (July 2011 to June 2013) and Period 2 (July 2013 to July 2014). We collected data on demographics (age, gender), National Institutes of Health Stroke Scale (NIHSS), time of last known normal (LKN), time of initiation of tele-stroke consult, time IVtPA advised by tele-stroke attending, and time of IVtPA administration. Tele-stroke start was defined as the time from initiation of tele-stroke consult (call received from the ER). Univariate analysis with Chi-square or Fisher's exact test for categorical variables and t-test for continuous variables was performed using commercially available statistical software (JMP 6).
Results
Among 259 consecutive stroke patients treated with IVtPA through the Rush tele-stroke program, the mean age was 69.6 years, 56% were female, the mean NIHSS was 11.8, and 41.7% patients were transferred to the hub institution. The mean time from tele-stroke start to IVtPA given was 42.2 min, and this varied by spoke hospital site (range, 29.6–54.9 min, p 0.0001). The mean time from tele-stroke start to IVtPA advised was 14.7 min, and this did not vary significantly among hospital spoke sites (ranged, 12.9–20.2 min, p 0.09). The mean time from IVtPA advised to IVtPA given was 27.1 min (range, 17.2–34.7 min, p 0.001). The mean time from LKN to IVtPA given was 155 min (range, 36–300 min).
Period 1 included 129 patients and Period 2 included 130 patients, and the patients did not differ by age (p 0.2), gender (p 0.3), or NIHSS (p 0.3) (Table 1). Comparing Period 2 with Period 1, there was faster mean time from initiation of tele-stroke consult to IVtPA advised (17.4 min vs. 12.5 min, p < 0.0001) and faster mean time from IVtPA advised to administration (33.1 min vs. 22.5 min, p < 0.0001). The time from initiation of tele-stroke consult to IVtPA administration also improved from Period 1 to Period 2 (49.9 min vs. 35 min, p < 0.0001). The mean time from LKN to IVtPA given improved from Period 1 to Period 2 (148.6 min vs. 160.9 min, p 0.045). All individual spoke sites showed improvement in times from tele-stroke start to IVtPA administration (Fig. 2).
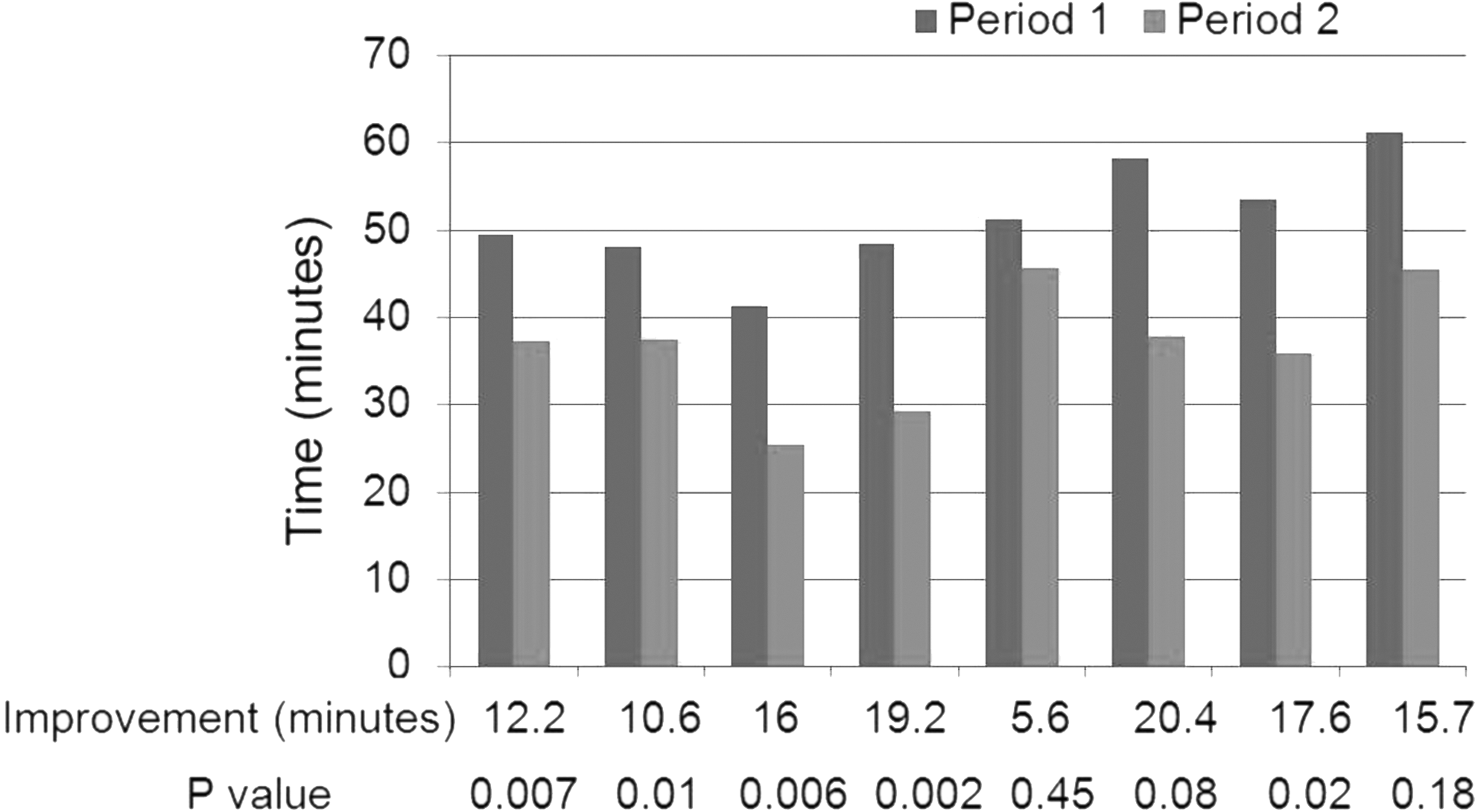
Mean time from tele-stroke start to IVtPA administration per individual hospital spoke sites. The hospital spoke ERs are displayed in random order. ER, emergency room; IVtPA, intravenous tissue plasminogen activator.
Period 1 Versus Period 2
Time+ = mean time (min).
IVtPA, intravenous tissue plasminogen activator; LKN, last known normal; NIHSS, National Institutes of Health Stroke Scale.
Discussion
Studies have shown that improved clinical outcomes after IVtPA are time dependent. 4 This urgency of treatment coupled with the shortage of onsite stroke expertise contributes to a situation where many hospitals have difficulty with timely administration of IVtPA. 5 Tele-stroke allows the safe and reliable administration of IVtPA at remote sites, 6,7 and participation in a tele-stroke system is associated with a significant increase in the rates of IVtPA utilization at the spoke hospitals. 2,3 Telemedicine is uniquely situated to offer a practical solution to providing rapid acute stroke evaluation, and telemedicine has been recommended as a strategy to increase access to acute stroke care by the American Stroke Association and American Academy of Neurology. 8,9 Although the use of tele-stroke has become widespread, it is still a relatively new and growing practice model, and as of 2012 tele-stroke programs were only in operation for a mean of 2.4 years. 10
Although participation in a tele-stroke system is associated with a significant increase in the rates of IVtPA utilization at the spoke hospitals, 2,3 the effects on quality measures such as timeliness of IVtPA delivery are uncertain. Our data show that participation in a tele-stroke network is associated with continued improvement in quality assessment measures, with improved performance at both the hub site and the spoke ERs in IVtPA delivery. This effect is likely multifactorial and is a result of programmatic benefits associated with being part of a tele-stroke system and learning effect from increased IVtPA volumes and maturation of the program. Participation in a tele-stroke network not only allows the spoke hospitals access to a vascular fellowship trained neurologist for an immediate audio–visual consult, but also offers the opportunity of an educational partnership with an academic hub site that allows a formal process for ongoing clinical improvement. We have demonstrated that the benefits of participation in a tele-stroke program for a spoke ER continue beyond the initial increase in IVtPA utilization rate.
Conclusions
Participation in a tele-stroke program not only increases rate of IVtPA but is also associated with improvement in the timeliness of IVtPA delivery. This improvement is due to faster responses in both the hub site (recommending IVtPA earlier) and spoke site (administering IVtPA faster). Further studies aimed at improving delivery of IVtPA in the tele-stroke program are warranted.
Footnotes
Acknowledgments
Dr. Lee received funding from an institutional neurology department grant. She was involved in design, analysis of data, and drafting the article. Dr. Cutting was involved in revising the article for intellectual content. Dr. Song. was involved in revising the article for intellectual content. Dr. Cherian was involved in revising the article for intellectual content. Ms. Diebolt was involved in analysis of data and revising the article for intellectual content. Mr. Bock was involved in revising the article for intellectual content. Dr. Conners was involved in revising the article for intellectual content.
Disclosure Statement
No competing financial interests exist.