
Abstract
Introduction
Tonsillectomy is one of the most common procedures in ear, nose, and throat (ENT) surgery. 1 It accounts for the largest proportion of major surgery in patients younger than 9 years of age in Korea. 2 Surgical operations such as tonsillectomy can be stressful and cause anxiety for all patients, especially for preschool children, whose cognitive awareness of the threatening situation is not yet fully developed. 3 Severe preoperative anxiety is associated with an increase in negative postoperative sick-role behavior. 3,4 Tonsillectomy patients may experience numerous complications during the early postoperative phase. 1,5,6 Many patients experience pain, nausea, vomiting, decreased fluid and food intake, fever, hemorrhage, dizziness, and constipation. 5 It is therefore important to enhance patients’ and caregivers’ competency to ensure that they engage in their appropriate role during recovery periods.
Since patients who undergo tonsillectomy are hospitalized for a short period of time, the parents assume the role of healthcare provider at home. 7 However, not all parents have the competency to adequately manage their children's postoperative treatment and control any side effects. 8 –10 Lack of postoperative management competency can adversely affect a child's care and may even cause complications. 1,11
Previous studies on pediatric tonsillectomy have suggested that parents, who have been taught pain assessment and management strategies, are better able to manage their children's pain. 10 Follow-up intervention in the form of telephone calls from a nurse has been shown to improve pain management and reduce the occurrence of complications. 5 Studies of preoperative education have presented the positive effects of standardized educational programs for both parents and patients of children who are undergoing inpatient elective surgery. Such programs are designed to improve the parents’ knowledge, attitudes, and behavior in relation to their children's postoperative pain management. This method has been shown to increase the children's well-being and the parents’ satisfaction as well. 8 Research findings have indicated that pain management booklets help parents efficiently manage the pain experienced by their children after tonsillectomy. 12 Information on post-tonsillectomy care in an illustrated book format was also shown to improve the efficiency of pain management and increase patients’ compliance with care. 13
Smartphone combines the functionality of mobile phones with Internet access and the ability to send text messages. 14 Studies have shown that smartphone technology and text messaging enhance both the healthcare provider–patient relationship and the effectiveness of the health education provided for patients. 15 Evidence-based research has shown the positive effects of education for patients or caregivers. However, research exploring the effects of education using smartphone text message for patients with tonsillectomy and their mothers is limited. Therefore, the purpose of this study was conducted to examine the effects of tonsillectomy education using smartphone text message on the following: (1) mother's knowledge on patient care and (2) children's anxiety and sick-role behavior.
Materials and Methods
Study Design and Participants
A randomized pre- and post-test two-group design using smartphone-based education and conventional textual comparison group was used to investigate the influence tonsillectomy education had on mothers’ knowledge, children's anxiety, and sick-role behavior.
The participants comprised preschool inpatients (from 3 to 7 years of age) and their mothers who were recruited from K university hospital in Seoul, Korea. The eligibility of 102 children and their mothers was assessed between May 2013 and January 2014 (Fig. 1). Thirty-four participants did not meet the inclusion criteria because the child was too young (20 participants). One parent declined to participate in the study because he was a health professional and regarded the service as unnecessary, and another parent declined because she was not interested. One participant's operation was cancelled, and five participants missed their appointments for surgery. Six children were excluded for medical reasons. As a result, 68 families were recruited as participants. The follow-up treatment received by the last participant ended on February 2014. Seven families in the experimental group were subsequently excluded from the analysis; three families did not provide care after surgery, two families failed to fill out the questionnaire, and two families were transferred to another hospital. The data for all 34 pairs allocated to the control group were analyzed, but only the data provided by 27 (79.4%) of the families in the experimental group were analyzed (Fig. 1).
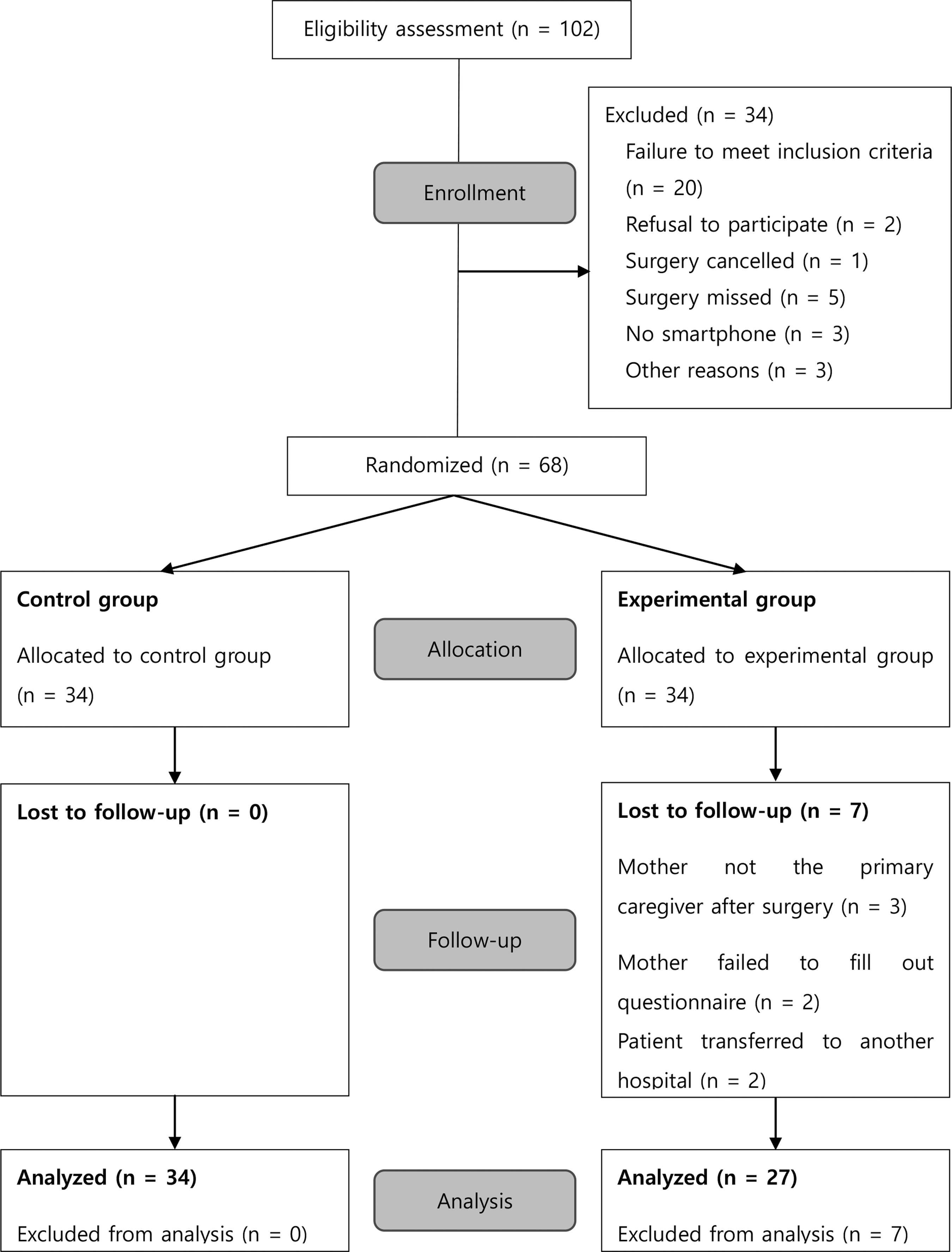
Flowchart for participants through the study.
The criteria for inclusion were as follows: (1) physical status classification 1 or 2 according to the classification system provided by the American Society of Anesthesiologists; (2) a mother who spoke Korean; and (3) guaranteed access to a smartphone to enable text messaging between the mother and a research nurse for the duration of the follow-up treatment. Patients with neurocognitive deficits, patients who had chronic pain, and patients who had undergone another surgery in the month before tonsillectomy were excluded.
Intervention
The smartphone-based tonsillectomy education was developed for children experiencing tonsillectomy and their mothers. Both groups were provided with information on the pre- and postoperation care of tonsillectomy. The control group received this information by conventional textual and verbal means only, whereas the experimental group received the information in the form of 10 text messages between the initial hospitalization and the first visit to an outpatient clinic. The content of text message was developed based on a literature review and an assessment of patients’ knowledge by a committee of clinical experts. The committee comprised two ENT specialists, four nurses with more than 7 years’ clinical experience in the ENT wards, and one professor of college of nursing. The essential information on the tonsillectomy education was divided into 10 parts covering the following areas: (1) preoperative orientation, examination, and precautions; (2) recovery after surgery; (3) postoperative precautions; (4) wound healing after discharge; (5) pain management; (6) diet management; (7) hemorrhage prevention; (8) administration of medication; (9) monitoring for excessive bleeding; and (10) follow-up guidance provided by the outpatient clinic. The 10 text messages were delivered at the following intervals: on the day of hospitalization; on the day of the operation; on the day of discharge; and every day from discharge to attendance at the outpatient clinic.
Sample Size
G*Power 3.1 16 was used to calculate the sample size required for repeated measures analysis of variance (ANOVA). With two groups and two measures, a sample size of 56 (28 per group) would yield 70% power to detect an effect size of 0.05. We assumed an attrition rate of 20%. Therefore, the final sample size was set at 68.
Randomization
The children were allocated to the intervention group or the control group by means of a pre-established randomization procedure by a nurse who was not involved in the study. The children who met the inclusion criteria and whose parent(s) agreed to participate were enrolled consecutively by the research nurse.
Outcomes
The outcomes for the mothers were the knowledge score on the day of hospitalization and the knowledge score on the postoperative day 7. The outcomes for the children were the anxiety level on the day of hospitalization and just before operation, and the score for their sick-role behavior upon visiting the outpatient department (postoperative day 7).
Mothers’ knowledge
A self-reported survey administered on the day of hospitalization was used to measure the mothers’ knowledge on tonsillectomy care. For this, researchers and ENT specialists developed a measurement with 20 questions. Then, a committee of clinical experts measured the content validity of the tool and reduced it to 16 questions with content validity indices of 0.8 or higher. The final version of the questionnaire that was used in the study was a 16-item dichotomously scored questionnaire with a Kuder–Richardson Formula 20 value of 0.63 and possible scores from 0 to 16.
Children's anxiety
A modified version of an eight-item self-report instrument 17 was used to measure the children's anxiety. The original scale was developed by Lebaron and Zeltzer 18 as a behavioral checklist to measure acute pain and anxiety in children and adolescents. Lim and Shin modified this checklist to obtain a 4-point scale with responses ranging from 1 to 4, and total scores ranging from 8 to 32, with higher scores indicating greater anxiety. 17 According to the researchers, this measurement of patient anxiety has a reliability score of 0.83. 17 In our study, the Cronbach's alpha was 0.79.
Children's sick-role behavior
A questionnaire developed by Cho 19 was used to evaluate the patients’ sick-role behavior. The questionnaire comprised nine items with a 3-point Likert scale (1, very well; 2, fairly well; 3, not well). The mothers were asked to indicate how well their children implemented measures to relieve their symptoms at home. The Cronbach's alpha for this questionnaire was 0.70.
Ethical Considerations
To ensure that the participants were protected, we obtained approval from the institutional review board [KHSIRB-12–025(RA)] before collecting the data.
Statistical Analysis
The data were analyzed using SPSS for Windows 19.0. A chi-square test, Fisher's exact test, and a t-test were used to measure the homogeneity between the two groups. A mixed-model repeated-measures analysis was conducted to test and compare education effects between intervention and comparison groups.
Results
Demographics and Baseline Characteristics
There were no significant differences between the two groups in demographic or baseline characteristics. Table 1 shows the participants’ demographic characteristics. The groups were similar in terms of mothers’ age, education, religion, and children's gender, age, and birth order. No significant differences were observed between the groups in the mean scores awarded for the mothers’ knowledge (t = 0.578; p = 0.565) or the children's anxiety (t = −0.175; p = 0.862).
Demographics and Baseline Characteristics
Interaction Effects Between Time and Group
Results of mixed-design, two-way ANOVA indicated significant interaction effects between time points and groups for mother's knowledge (F = 4.26, p = 0.043) and children's anxiety (F = 3.32; p = 0.037). Thus, the results do support the effectiveness of tonsillectomy education using smartphone text messaging in increasing mothers’ knowledge and reducing children's anxiety.
Differences of Mothers’ Knowledge and Children's Anxiety in Each Group
Table 2 presents the pre- and postoperative mean scores of mothers’ knowledge and children's anxiety. In both groups and at both measurement points, mothers’ knowledge scores were increased, respectively (t = 5.51, p < 0.001 and t = 4.3, p < 0.001). A Student's t-test demonstrated that mothers who received information using smartphone text messaging showed significantly higher scores than the control group. In both groups and at both measurement points, children's anxiety was increased, respectively (t = 2.99, p = 0.004 and t = 3.2, p = 0.002). Children in the experimental group were less anxious than those in the control group.
Differences of Mothers’ Knowledge and Children's Anxiety in Each Group
Children's Sick-Role Behavior
The children's sick-role behavior differed significantly between the two groups (t = 1.86, p = 0.034) (Table 3). Analyses of the children's sick-role behavior revealed significant differences in three in nine categories. The children who were provided with information by text message received higher scores for “ice pack application” (M = 1.44) than the patients who received information by conventional means only (M = 1.09) (t = −1.96, p = 0.028). The scores for “chewing gum” were higher in the experimental group (M = 1.56) than in the control group (M = 1.24) (t = −2.00, p = 0.025). The patients who received information by text message received higher scores for “eating ice cream in response to pain” (M = 1.85) than the patients who did not receive text messages (M = 1.47) (t = −2.43, p = 0.009).
Differences of Children's Sick-Role Behavior
one-tailed test p < .05.
one-tailed test p < .01.
POD, postoperative day.
Discussion
The purpose of the study was to determine the effectiveness of providing the mothers of tonsillectomy patients with information about the tonsillectomy education by means of smartphone text message. Our findings show that the delivery of education improved the mothers’ knowledge in both the control and experimental groups. In previous studies, a standardized educational intervention protocol has been found to improve parents’ knowledge, attitudes, and behavior with regard to postoperative pain management and to ultimately reduce the children's postoperative pain. 8,20 Huth et al. 20 suggested that the use of educational booklets increases parents’ understanding of the required medication and improves their ability to administer this medication. Educational interventions have been shown to improve parents’ attitudes toward and increase their understanding of their children's perioperative management and improve their anxiety relief strategies, thereby helping them to provide the perioperative care necessary for their children's physical recovery and well-being. 8 In short, education is helpful to mothers.
In this study, the knowledge scores achieved by the mothers who were provided with information by smartphone text message were significantly higher than the scores of the mothers who received information by conventional means only. Smartphone technology has emerged as an adjunct means of helping patients manage their own healthcare. 15 Smartphone provides easy and rapid access to information and allows their users to move freely while accessing this information, unlike desktop personal computers. 21 They thus improve the efficiency of specialized healthcare consultation, ultimately improving the care given to patients.
The findings of previous studies on the uses of smartphone with teenage sufferers of asthma indicated that smartphone enables the patients not only to receive health information but also to communicate with nurses by text message. Smartphone has also been shown to help nurses provide continuous and immediate feedback to enhance the nurse–patient relationship. 15 These findings are corroborated by the results of this study, which suggest that the use of smartphone to provide education enhances the nurse–patient relationship and enables patients to communicate and interact with healthcare providers in real time.
When planning the study, we intended that the nurses would deliver the intervention (i.e., send 10 text messages to the patients’ mothers) in one direction. However, a feedback loop occurred. At the end of the experiment, the number of messages sent and received was found to have been three times greater than planned. In addition, the parents requested more detailed and specific information. Previous researchers have found that parents often ask for additional information, guidance, and support from health professionals, especially regarding their children's pain management. 8,22 The nature and amount of information delivered were determined according to an assessment of the mothers’ information needs and the results of a pilot study. However, the mothers’ needs were more varied than we anticipated. Therefore, the nurses were required to deliver more specialized knowledge throughout the recovery period to meet the needs of specific patients and their parents.
We also found that the increase in anxiety experienced by the patients who received text messages by smartphone was significantly lower than that experienced by the patients who received information by conventional means only. Preoperative anxiety is common among children and has been associated with negative preoperative behavior such as muscle stiffness, shouting, agitation, crying, and the need for physical restraint. Preoperative anxiety has also been associated with maladaptive postoperative behavior such as postoperative pain, parent–child conflict, and negative sick-role behavior. 23
Various prevention strategies have been proposed to reduce the incidence of preoperative anxiety in children. Both pharmacological methods such as sedatives and nonpharmacological approaches such as parental presence, preparatory behavioral programs, music, and acupuncture have been shown to be useful. Similarly, educational interventions may help to reduce the anxiety of children who face tonsillectomy. 23 He et al. suggested that therapeutic play intervention helps to reduce perioperative anxiety, negative emotional manifestations, and postoperative pain. 9 In this study, the children in the experimental group were found to be less anxious than those in the control group. The additional information provided to the mothers in the experimental group probably encouraged them to soothe their children, thereby reducing their anxiety. Therefore, we suggest that the delivery of information to mothers by text message may reduce their children's preoperative anxiety and the likelihood of developing negative postoperative behavior.
Third, the patients who received text messages by smartphone achieved significantly higher scores for sick-role behavior than the patients who did not receive text messages. In one study, the members of the experimental group, who were provided with information on the tonsillectomy procedure in the form of an illustrated children`s book, were more compliant with treatment than the patients in the control group. 13 The provision of information on tonsillectomy was thus found to be an effective intervention for preschool tonsillectomy patients.
The patients’ sick-role behavior differed significantly between the two groups with respect to three variables: “ice pack application,” “chewing gum,” and “eating ice cream in response to pain.” These findings may reflect the greater knowledge of the mothers in the experimental group, who were informed by text message that “it is helpful to eat ice-cream or drink cold milk when the throat is painful or swollen,” and that “it is helpful to swallow one's saliva, despite the pain.” The mothers who were provided with this information were probably better equipped to supervise their children's sick-role behavior.
Limitations
There are many limitations to this exploratory study. Limitations included small size of sample, lack of tonsillectomy home care standards, and validity of questionnaire. Thus, generalizability of the results of this study is limited. In this study, the contents delivered by smartphone text message were developed by the clinical experts committee. However, the standardization of tonsillectomy home care was not tested. Measurement tools used in this study need to be verified further, but open questions may have helped to limit this bias.
Conclusion
The results of our study suggest that providing information by smartphone text message helps to increase the knowledge of mothers of tonsillectomy patients to relieve patients’ anxiety and to improve patients’ sick-role behavior. These findings offer guidelines for the development of preoperative nursing interventions for children who face various types of surgery, not just tonsillectomy.
Based on the results of our study, we make the following recommendations. (1) More studies should be conducted to confirm the positive effects of providing information by smartphone text message. (2) A preoperative educational program delivered in instant message format should be developed to reduce anxiety and improve the sick-role behavior of patients who undergo operations. (3) Various informational programs delivered in text message format are needed to aid patients’ management of postoperative pain and anxiety.
Footnotes
Disclosure Statement
No competing financial interests exist.