
Abstract
Introduction
Fundus photography with nonmydriatic cameras, often used in combination with telemedicine approaches, has become one of the most widely used system for retinal screening worldwide. 1 Screening for diabetic retinopathy (DR) is an important area of application. The ever-increasing diabetic population and the frequent retinal examination these patients require have prompted the development of more efficient methods other than conventional fundus studied by ophthalmologists. Another area of application is age-related macular degeneration (AMD), currently being the first cause of blindness in Europe. 2 A large percentage of the population has early and intermediate forms of this disease and, being asymptomatic, they do not usually visit the ophthalmologist for a fundus examination.
In addition to incipient DR and AMD, retinal examination can detect other eye diseases that may not manifest symptoms such as nevus, hypertensive vasculopathy, retinal dystrophy, macular pucker, and pigment epithelium abnormalities. According to an international poll performed in 2012 3 only 21% of the population had visited an ophthalmologist in the previous 5 years. The main reason why the remainder had not consulted (45% of these individuals) was because their vision seemed fine and they thought they did not need any eye examination.
In our hypothesis, optometry centers could be a good place for a general screening of retinal diseases. In other words, if we perform a retinography to every patient entering an optometry center, more pathology can be detected, especially in early stages.
In Spain all opticians are also optometrists but they do not have any formal training in retinal diseases so they are not supposed to make any formal report at this point. They are allowed to make eye refractions and eye examinations without using any kind of drug, not being allowed to provide any treatment. We began using fundus photography with nonmydriatic cameras in optometry centers in Spain, starting in 2012 Images obtained were then sent for reading by retinal specialists using the OPTretina software (Optretina SL, Barcelona, Spain) and telemedicine network. Our goal was to perform high-quality widespread screening of eye conditions through a web-based platform. The aim of this study is to describe the outcomes of this initiative over the first 3 years it has been applied.
Methods
Examination Protocol
We recommended retinal fundus photography of all patients arriving at the optometry centers. Patients were informed by attending optometrists about the advantages and limitations of the test and were provided with an information sheet. Informed consents were collected to carry out all tests. Fundus photography was performed using several types of nonmydriatic cameras that had been previously approved by a medical committee to guarantee the quality of the images. All cameras evaluated more than 40° of the retina. At the time of writing, the following cameras had been accepted for screening: Topcon NW-200, Topcon NW-300, Topcon NW-400, Topcon NW6S, Topcon NW8, Nidek AF230, Nidek AF330, Zeiss Visucam 200 and 500, I-optics Easy Scan, and all cameras approved by the National Health Service for Diabetic Screening in the United Kingdom.
Optometrists were instructed to perform posterior pole retinal photography, centered on the macula and including the optic disc and vascular arcades. In known diabetic patients, we recommend two fields per eye, one centered on the macula and one on the optic disc. Information on refraction, best corrected visual acuity, the reason for going to the optometrist, and whether the patient had known diabetes were collected in each case in addition to the retinal fundus images. Intraocular pressure measured with an air tonometer was also recorded when available.
Telemedicine Software
Before images were sent to the retinal specialists for reading, the telemedicine software anonymized patient's information by assigning a unique identification number to each case so that readers only had access to patients' reference number not to their personal information. Each reader was assigned a secure login and password to sign the reports.
Ophthalmological Examination
At the time of writing, five ophthalmologists specialized in retinal pathology comprised the medical team. Cases were randomly assigned to each specialist. Diagnostic impressions and recommendations for referrals to ophthalmological consultations were included at the report but not recommendations for treatment or further testing as these aspects were left to the criteria of the ophthalmologist performing the referral consultation.
Patients with no symptoms and normal findings on retinal study were advised to have annual fundus photography at the optometry center. All acute, symptomatic patients (e.g., those with floaters, metamorphopsia, acute decrease in visual acuity, or diplopia) were referred to the ophthalmologist, including those with no abnormal retinal features. All patients with findings departing from strict normality were referred to the ophthalmologist, included those with features that may not be pathological in some cases, such as small nevi, drusen, or pigment abnormalities. All patients with high myopia retinal signs (e.g., large disc crescents, posterior staphyloma, lacquer cracks, chorioretinal atrophy) were referred to the ophthalmologist.
Suspicion of glaucoma in retinographies was done following international recommendations: Increased cup to disc (C:D) ratio (>6), vertical elongation with vertical C:D >0.4, rim notching, asymmetry of C:D (>2), disk or disk edge hemorrhages. 4 The specialist readers' evaluation included the image quality. Readers did not judge or comment on poor-quality retinal images in which macula, vessels, or optic disc evaluation was not unreliable. In addition to eye-specific diseases, retinal lesions with systemic implications were also described and referral to the appropriate specialist was recommended: a neurologist in suspected papilledema and a general practitioner in cases showing hypertensive vasculopathy or DR signs.
All reports were sent back to the optometrist within the first 48 h following the retinal photography. All reports were signed by the ophthalmologist and included his/her name and identification number in the official Spanish association of physicians. To avoid potential referral bias, the report makes no mention of a selected referral medical center.
Statistical Analysis
Patient data were analyzed in SPSS 15.0 (LEAD Technologies 2006). Descriptive information for the entire series examined over the last 3 years was included.
Before performing the comparisons of means, the Kolmogorov–Smirnov test was applied to confirm data distribution normality. The Student's test was use to compare the mean age and spherical equivalent value between patients who showed normal findings and those with retinal abnormalities. The chi-square test and odds ratios (ORs) were used to evaluate associations between qualitative variables.
Ethics
Before undergoing fundus photography, all patients received an information sheet that explained the objectives and limitations of the test and signed an informed consent form. Institutional Review Board (IRB)/Ethics Committee approval from Hospital Vall d'Hebron in Barcelona was obtained for the data review and the study design.
Results
Patient Characteristics
The descriptive data are summarized in Table 1. A total of 50,384 patients were included. Patient age ranged from 3 to 99 years, with a mean age of 52.3 years.
Descriptive Data of Broad Population Screening with Nonmydriatic Retinal Photography
AMD, age-related macular degeneration; NPDR, nonproliferative diabetic retinopathy; PDR, proliferative diabetic retinopathy.
The main reason for consulting at the optometry center was routine review of eyeglasses in 35,772 patients (71.5%). Other causes were a subjective decrease in visual acuity in 6,197 patients (12.3%), acute onset of floaters in 639 patients (1.3%), and headache in 201 patients (0.4%).
Mean visual acuity was 20/25 in the right eye and 20/25 in the left eye. Refractive errors ranged from −29 to +24.8. Mean spherical equivalent error was −0.36 in the right eye and −0.34 in the left eye.
Among the total of patients seen, 3,627 had been diagnosed of diabetes (7.2%).
Retinal Abnormalities
Main retinal abnormalities are presented in Figure 1. Among the total of patients examined, 75% (37,697 patients [p]) showed normal findings, and 21.5% (10,820 p) presented abnormal retinal findings. Due to the presence of acute floaters or other acute symptoms, 1.4% (703 p) and 1.1% (578 p) were referred to the ophthalmologist, respectively. Finally, 1.1% (586 p) were not evaluable because of poor-quality photographs (Fig. 2).

Main retinal abnormalities observed in the nonmydriatic fundus camera examination. AMD, age-related macular degeneration; BRVO, branch retinal vein occlusion; CNV, choroidal neovascularization; DR, diabetic retinopathy; ERM, epiretinal membrane.

Pie chart. Percentage of normal patients, patients referred to the ophthalmologist and timing of their referral, and cases that could not be assessed.
In total, 12,634 patients were referred to an ophthalmologist with the following recommendations: an urgent visit in 9%, a preferential visit (within 2–3 weeks) in 11%, and an ordinary scheduled visit in 80%. Hence, in the overall series, 19% of patients screened were referred for an ordinary visit, 2% for a preferential one, and 1% for an urgent visit (Fig. 2).
AMD was the most common abnormal feature observed, documented in 2,456 patients (4.8%): 1,081 patients were referred under suspicion of early AMD, 841 patients with intermediate AMD, and 534 patients with suspected advanced stage. Acute choroidal neovascularization was suspected in 144 patients (2,318 eyes with suspected early AMD, 1,618 eyes with suspected intermediate AMD, and 858 eyes with suspected advanced AMD). High myopia was the second common abnormality observed (1,099 p). Epiretinal membrane was also a common detected abnormality with a total of 764 cases (1.5%).
DR was suspected in 543 patients (1.07%). Nonproliferative DR signs were seen in 1,007 eyes. Proliferative DR signs were seen in 56 eyes. Diabetic macular edema was suspected in 163 cases. Retinal screening identified 46 patients with DR signs who were unaware of their condition.
Stage II or higher hypertensive vasculopathy signs were detected in 193 patients. A hypertensive emergency was identified in two patients, one of them completely asymptomatic and the other one with a frontal headache.
Signs of the following additional diseases were observed: nonspecific maculopathy (central pigment epithelium abnormalities) (494 p), suspected glaucoma (480 p), branch retinal vein occlusion (121 p), central serous corioretinopathy (101 p), suspected macular dystrophies (98 p), retinal detachment (26 p), optic disc drusen (43 p), unknown retinitis pigmentosa (22 p), optic disc pit (12 p), bear tracks (13 p), suspected papilledema in 28 patients (21 asymptomatic, 5 headache, 2 flashes and visual field abnormalities), chorioretinal coloboma (5 p), angioid streaks (5 p), intraocular tumors (3 p), and one suspected orbital tumor, proven to be a glioma.
All 703 patients with acute floaters were urgently sent to the ophthalmologist for a peripheral retina assessment. A total of 578 patients with acute symptoms were also referred to the ophthalmologist for evaluation.
Associations Between Retinal Abnormalities and The Patients' Characteristics
Patients with retinal abnormalities were older than the group with normal findings (mean age 62.2 vs. 49.3 years; p < 0.0001). A considerably higher percentage of patients older than 50 years showed abnormalities on retinal photography than younger patients: 31.5% vs. 11.1% (p < 0.0001; OR 2.47 confidence interval [CI] 2.37–2.57) (Fig. 3). Main reasons for referring younger patients (<50 years) to the ophthalmologist were high myopia signs (312 p), high intraocular pressure (214 p), acute floaters (153 p), DR signs (117 p), nevus (113 p), glaucoma at optic discs suspected signs (108 p), nonspecific maculopathy (107 p), epiretinal membrane (83 p), central serous corioretinopathy (62 p), and suspected macular dystrophies (27 p).
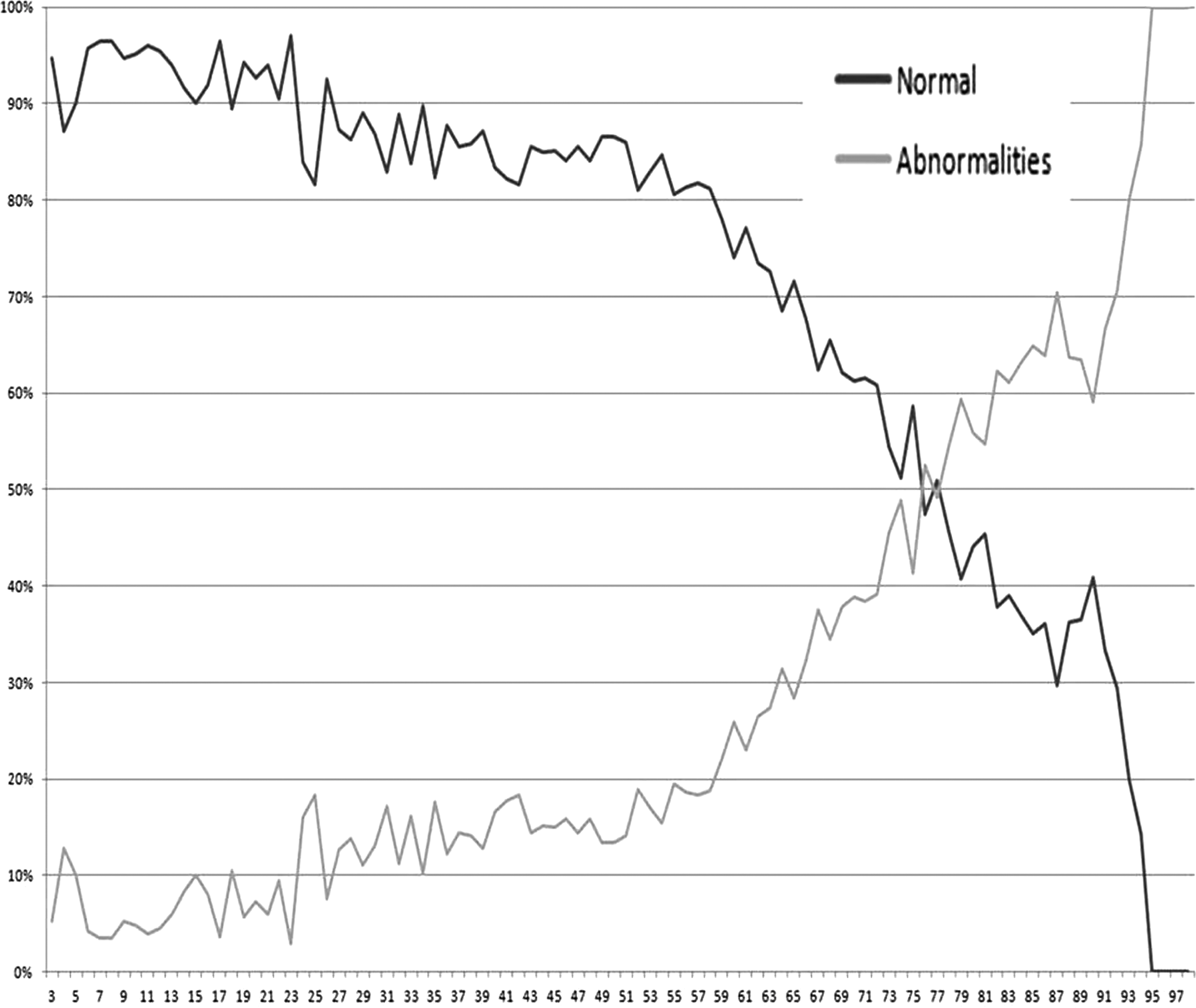
Presence and absence of retinal abnormalities detected by nonmydriatic fundus photography according to age.
Patients with nonassessable images were older than patients with gradable images (66.7 years vs. 50.7 years; p < 0.001).
Patients referred to the ophthalmologist had a higher negative spherical equivalent than normal patients (abnormalities group: right eye mean −0.66 DD, left eye −0.62 DD vs. normal group: right eye −0.28DD, left eye −0.26DD).
Patients with high myopic defects (>−5DD in one or both eyes) were referred more often to the ophthalmologist attending to retinal abnormalities (p < 0.001; OR 1.04; CI 1.03–1.05).
Discussion
It is a common goal in all branches of medicine to develop affordable, quick, and easy methods to detect disease and nonmydriatic fundus photography conforms to this idea. The essential role of nonmydriatic cameras in screening programs for DR is well recognized 1,5 –8 and there is also evidence of the benefits in other diseases screening such as AMD 9 –13 and neurological diseases. 14,15 Nonmydriatic cameras have been used successfully in the general population in the emergency department 16 and as pilot tests in ocular disease screenings. 17,18
Answering our first hypothesis, more than 20% of the population assessed with this technology presented retinal abnormalities. We recognize that there may be some bias in our cohort since the individuals included were consulting with an optometrist and only those accepting fundus photography were included. Nonetheless, this percentage represents a large number of patients who were unaware that they should undergo ophthalmological evaluation.
The reasons why patients do not visit the ophthalmologist are mentioned in the Bausch and Lomb Barometer: 44% believe that “I don't need an eye test unless there is a problem,” 42% believe that “If I can see, my eyes must be healthy,” 4 in 10 believe that “The only reason to visit an eye doctor is for vision correction,” and one-third believe that “If it doesn't hurt, it's not serious.” 2 To our mind, the extensive screening provided by the system described here has three main objectives: (1) to detect all asymptomatic retinal abnormalities in the posterior pole; (2) to refer more and better-filtered pathologies to ophthalmologists; and (3) to make the population aware of the importance of checking their retinas even though they have no symptoms.
In our series, the risk of having retinal abnormalities was higher in individuals older than 50 years, making the screening highly recommended over this age; nevertheless, we found retinal abnormalities also in young people. In this age group, high myopia signs, suspected retinal dystrophies, the worst cases of proliferative DR, and acute floaters were detected and required ophthalmological control. Although retinal examination may be more difficult in children, fundus study with nonmydriatic cameras has proven to be an easy and reliable test in these young patients. 19
It is well recognized that retinal disease early detection improves the visual and anatomical outcomes of DR. 20,21 According to the American Telemedicine Association our screening of DR could be consider as a Category 1 program; Category 1 validation allows identification of patients who have no or minimal DR and those who have more than minimal DR. 22 All pivotal studies with anti-VEGF drugs demonstrate better functional outcome in patients with higher baseline visual acuity and early detection of the neovascular disease. 23,24 ) Recent studies have also concluded that patients in whom AMD is promptly detected have better preserved visual acuity than other AMD patients. 25,26 Other diseases in which early detection has a beneficial impact on outcome include epiretinal membrane, 27 retinal detachment, 28 and, of course, glaucoma.
In Spain only DR screening is performed by the national health system, so our screening was supported by the own patients. Au and Gupta 5 have reported data on the economic burden of screening programs using teleophthalmology. The authors found that this measure is highly cost-effective in DR and prematurity retinopathy and they suggested that the initial results of screening in other diseases such as macular degeneration are promising but require further investigation. The total cost of screening with the system implemented here is less than €15 per patient (including the cost of the camera and the retinal specialist evaluation), a figure that compares well with the cost (over €20) reported by Gomez-Ulla 29 and the experience in Canada (over $100). 30 Furthermore, these other systems did not have retinal specialists performing the readings. The lower cost with our method is attributable to the fast and easy software used and to the short time needed to generate each report.
In some countries, DR screening is performed by professionals other than ophthalmologists although under ophthalmological supervision; for example, optometrists evaluate the images in the United Kingdom and general practitioners in Spain. In this type of screening for a specific disease, the readers are trained to detect a small number of signs and follow a simple referral protocol when abnormalities are noted. We believe that general retina screening (of apparently healthy individuals) should be led by retinal specialists. The large number of possible abnormalities and the complexity of some diseases make it difficult for other professionals or much difficult for software to perform this task. No one is better than an ophthalmologist specialized in retinal disease to assess retinal findings and determine the need and timing of referral. Other authors, such as Ruamviboonsuk et al. share this impression. 31
Telemedicine is changing our way of working and the way patients seek healthcare in ophthalmology and other medical areas. Broad access to information (not always accurate) using the Internet, high-resolution cameras on cellular phones, and easy access to supposedly qualified second opinions are examples of these trends. In our opinion, the community of ophthalmologic professionals should try to lead these changes to preserve the standards of quality in our field and avoid intrusion by other professionals.
The main limitations of the screening results presented here are related to patient selection bias (individuals going to the optometrist and consenting to fundus photography). We had a small percentage of nonassessable images compared to other screenings, we believed optometrist did not send images they thought weren't good enough for the evaluation and directly send the patient to the ophthalmologist for conventional examination. The difficulty of having new feedback from all patients referred for examination is another limitation in our case. Conventional fundus examination outcomes in our patients are also difficult to track because all participants are dispersed all around Spain. We have only oral feedback about some of the more serious conditions such as tumors, malignant hypertension, papilledema, proliferative DR, retinal detachment, retinitis pigmentosa, and some other retinal dystrophies.
Nonetheless, nonmydriatic camera performance has been well documented: a one-field fundus image examination has a sensitivity of 71% and specificity of 96% for identifying DR and is considered valid for detecting this condition and macular edema. 32 Lin et al. reported highly significant agreement (kappa = 0.97, p = 0.0001) between the degree of retinopathy detected in a single nonmydriatic monochromatic digital photograph and that seen in seven standard 35 mm color stereoscopic mydriatic fields. 33 Similar results of high sensitivity and specificity, and high interobserver and intraobserver reliability have been reported in AMD, 11 –13 and have led the authors to conclude that single-field nonmydriatic retinography is reliable for screening of this disease. In conclusion, our results indicate that broad population screening is justified because of the high rate of asymptomatic retinal abnormalities detected especially after age 50. A large volume of patients visit optometrists in Spain and many are unaware that they have retinal conditions that should be controlled by an ophthalmologist. The ophthalmic community should lead initiatives such as the one presented here to preserve and guarantee the quality standards of retinal screening.
Footnotes
Disclosure Statement
The corresponding author M.A.Z. is co-founder and medical director of Optretina. G.A., A.F., M.A., A.O., and E.G. are retina consultants in Optretina and they have received payments for their job evaluating retinal images. J.G.-A. has no conflict of interest.