
Abstract
Introduction
Teleophthalmology has been gaining acceptance worldwide as an effective eye care delivery model, especially for extending the reach of specialty eye care to medically underserved populations and rural areas. 1 One of the most established well-validated teleophthalmology programs is diabetic teleretinal screening, utilized across the world to address the growing epidemic of diabetes and to lower the rate of blindness from diabetic retinopathy (DR). 2 –4 Given the success of diabetic teleretinal screening and the improvement in imaging techniques and technology infrastructure, many other teleophthalmology programs evaluating for other ocular diseases have been developed. For example, pediatric teleophthalmology (retinopathy of prematurity [ROP] screening), 5 –7 focused glaucoma screening programs, 8 –10 and macular degeneration screening. 11,12 Data on all of these programs suggest that teleophthalmology is effective, safe, and well accepted by patients. 13,14 Given the safety and success of teleophthalmology to detect eye disease other than DR, the Veterans Health Administration (VA) is contemplating utilizing more teleophthalmology to help address access issues and provide care for its growing population of geriatric (age 65+) and rural Veterans; projected to grow 66–132% in the next 10–15 years. 15
The VA is the largest integrated healthcare system in the United States, serving millions of Veterans, many of whom have diabetes. The most thoroughly developed teleophthalmology program at the VA is the national diabetic teleretinal screening program in the community-based outpatient clinics. This program, initiated in 2006, screens Veterans for DR. Fundus cameras capture retinal images, which are then stored on a server and forwarded remotely for interpretation by an eye care professional. Patients are referred for evaluation if there is DR, but also if there are other abnormalities detected, including suspicious optic nerve findings, age-related macular degeneration changes (AMD), or poor image quality (as a marker for media opacity). There is substantial literature on the accuracy and cost-effectiveness of fundus photos for the detection of DR. 16 –20 However, less data is available about the use of these photos to simultaneously detect other common ocular diseases, although many teleretinal screening programs for diabetes will also refer patients for other ocular conditions. 16,17,21,22 It is difficult to obtain both sensitivity and specificity calculations for other ocular disease in a teleretinal program as those patients with a “normal” diabetic image examination may not receive a face-to-face examination for comparison. 23 –25
There are only a few articles regarding the accuracy of a diabetic teleretinal screening program to detect nondiabetic eye disease. Chow et al. compared stereoscopic photographs in 280 patients with an eye examination for nondiabetic eye disease and found high agreement; however, this study utilized stereoscopic photographs and the ophthalmologic examinations were performed about a month later. 26 Information about the accuracy of diabetic teleretinal protocols to detect nondiabetic disease is important to obtain, especially if the VA is contemplating expansion of the teleretinal screening concept to encompass additional ocular disease screening. To our knowledge, a direct prospective comparison of a diabetic teleretinal imaging protocol versus a face-to-face examination performed on the same day to detect several nondiabetic ocular diseases has not been done. Before conducting a lengthy prospective trial, however, it would be useful to add to the existing literature by conducting a preliminary assessment of the ability of diabetic teleretinal images to detect multiple nondiabetic ocular diseases in a large cohort of patients. Therefore, this study was conducted to retrospectively analyze the ability of the VA diabetic teleretinal screening protocol to detect common sight threatening ocular diseases other than diabetic-related eye disease, for example, glaucoma, AMD, and cataract.
Materials and Methods
This study received Institutional Review Board (IRB) approval from the Atlanta VA and Emory University and conformed to the tenets of the Declaration of Helsinki. All investigators were compliant with the U.S. Health Insurance Portability and Privacy Act (HIPPA).
The Veterans Health Information Systems and Technology Architecture (VISTA) database was used to identify all patients who underwent teleretinal screening from October 1, 2008 through March 31, 2009. Patients were excluded from the study if they did not have adequate images (technical failure) obtained. The VA protocol utilizes three wide-field photographs of the disc, disc-macula, and superotemporal periphery. No stereoscopic images are obtained. Photos are taken by licensed practical nurses or telehealth technicians after dilation with one drop of 2.5% phenylephrine and 1% tropicamide. Other ocular parameters such as vision and eye pressure are not assessed. The Atlanta VA reading center was staffed by licensed and credentialed medical doctors in their fourth year of postgraduate ophthalmology training. The readers also passed the Ophthalmic Knowledge and Assessment Program test and all successfully completed teleretinal training. Reader accuracy was ensured through quarterly random audits by the Chief of Ophthalmology. Readers followed a strict protocol of referral guidelines based on the Preferred Practice Patterns of the American Academy of Ophthalmology. 27
Patient charts from teleretinal screening were divided into two groups–“Abnormal” and “Normal.” “Abnormal” represented patients who were referred to the eye clinic because of an abnormal imaging examination. “Normal” represented patients who had a normal imaging examination, but came to the eye clinic subsequently to have a clinical examination. The normal patients came to the eye clinic either by self-referral, primary care referral to receive other screening (e.g., glaucoma), or desiring eyeglasses.
The Computerized Patient Record System (CPRS), the VA electronic medical record, was retrospectively reviewed on all of these patients. The record review was used to determine if the findings on the teleretinal imaging examination matched the findings on the face-to-face clinical examination. The same database of patients was used to study the resources needed by the local eye clinic to care for patient referrals; this resource allocation study was previously published. 28
Chart Review for “Abnormals”
Demographic data such as age and sex were documented. Teleretinal imaging notes were reviewed for the referring diagnoses, which were categorized as: nerve-related disease (including glaucoma suspect, disk edema, and nerve pallor), AMD, lens or media opacity, DR, diabetic macular edema (DME), and others (e.g., vascular events and choroidal nevus). Patients could be included in multiple categories if the teleretinal interpretation note contained more than one referring diagnosis. The CPRS notes were then reviewed for the patients who attended their follow-up appointments, and the diagnoses that were made by the face-to-face physician were grouped in the same manner as the teleretinal diagnoses.
Not every patient who was referred for an ophthalmic examination kept their clinic appointment. For those patients who were not seen at the Atlanta VA Eye Clinic, CPRS was searched for the presence of an outside community physician note. If such a note was available, the diagnoses were collected and compared to the teleretinal diagnoses.
Chart Review for “Normals”
The CPRS medical record was reviewed for each patient who had a normal teleretinal examination. Any eye examination recorded in the system was utilized, as long as it was done after the teleretinal screening. If an ophthalmic note was present in CPRS either by the Atlanta VA eye clinic or an outside provider, the diagnoses made at the clinical examination were documented following the same categories above.
Only visually significant and/or sight-threatening diagnoses were included in the study. For example, dry eye not affecting vision, dermatochalasis, and blepharitis without effect on vision were excluded. Cataract was included only if the media opacity precluded effective teleretinal screening or if the patient was subsequently referred for cataract surgery after seeing the face-to-face provider.
Teleretinal screening ability was assessed by the percent agreement between the teleretinal reader and the clinical examination. The clinical examination, comprising at minimum, of a slit lamp biomicroscopy and an indirect peripheral retinal examination, served as the reference diagnostic gold standard for all patients. An ocular coherence tomography (OCT) image might have been ordered to evaluate for glaucoma or macular changes depending on the discretion of the examining physician.
Data Analysis
Most of the information was summarized qualitatively. Any statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS). 29 Calculations for sensitivity, specificity, and negative and positive predictive values for the major referral categories were completed.
Results
A total of 1,774 patients were imaged through the diabetic teleretinal screening program between October 1, 2008 and March 31, 2009 (Fig. 1). Ninety four image sets (5.3%) were unreadable due to technical issues (not related to media opacity) and excluded from the study, resulting in 1,680 unique patient image sets that were interpreted by the reading center. The images for 465 patients (27.7%) were categorized as “abnormal” and referred for a clinical examination. Two hundred sixty-two of these 465 patients (56.3%) actually had an examination. The images for 1,215 patients were read as “normal” and received a recommendation to repeat teleretinal screening in 1 to 2 years. Six hundred forty-one of the 1,215 (52.8%) patients with a normal image received a clinical examination. In the “normal” category, 387 patients had an examination within 2 years of the teleretinal screening and 254 had an examination two or more years after teleretinal imaging.
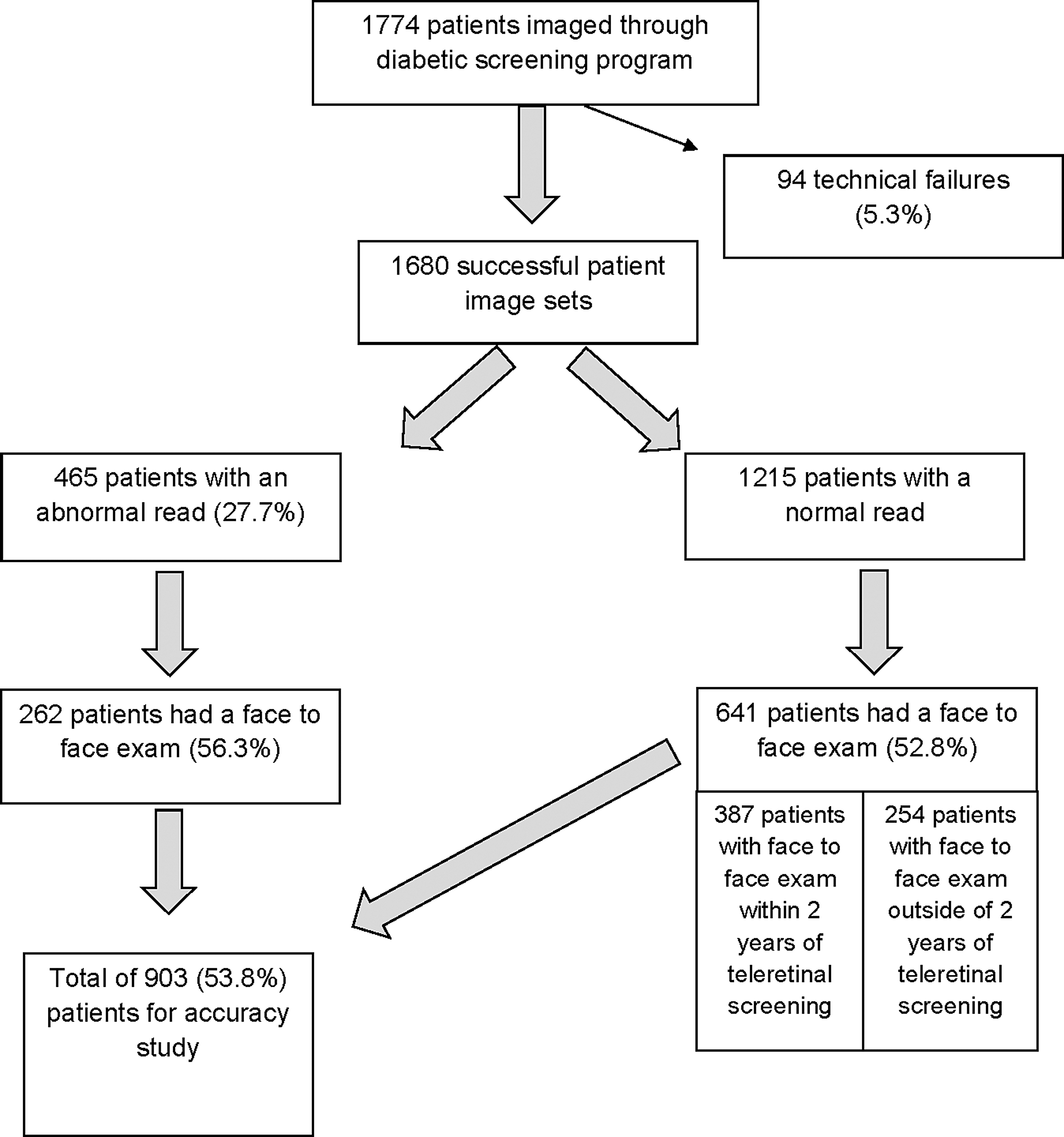
Study design and patient flow.
Out of the 1,680 patients who had successful teleretinal imaging, 903 (53.8%) eventually underwent a clinical examination at the VA or there was a non-VA note documented in the medical record. Demographic data are presented in Table 1.
Demographic Data
Table 2 illustrates qualitatively the discrepancies between the “normal” teleretinal reads and the clinical examination conducted after the imaging test. One hundred twenty-three (19.2%) of the 641 “normal” teleretinal reads did not completely agree with the “normal” teleretinal read (Table 2). Sixteen patients (2.5%) had an eventual intervention (medication or surgery) after a “normal” teleretinal read.
Qualitative Summary of Discrepancies from Normal Teleretinal Examinations (n = 641)
ARMD, age related macular degeneration.
Using the 903 total patients who had a clinical examination, percent agreement, sensitivity, specificity, positive predictive value, and negative predictive value were calculated for the following ocular conditions: nerve (i.e., glaucoma suspect or glaucoma), cataract, AMD, DR, and DME. These conditions were chosen because they are the most common causes of visual impairment in the veteran and elderly population in the United States. The percent agreement, specificity, and negative predictive value were over 90% for each disease category. Sensitivity ranged between 71 and 83%. Teleretinal imaging had the lowest positive predictive value for DME (Table 3).
Accuracy of Teleretinal Imaging to Detect Multiple Eye Diseases (n = 903)
Discussion
The current study is one of the first to evaluate the ability of the VA teleretinal screening protocol to detect multiple ocular conditions other than DR. The results from this retrospective evaluation were encouraging, demonstrating favorable negative and positive predictive values for glaucoma suspect, AMD, and cataract. For example, if 100 patients are screened through teleretinal imaging, 88 would have normal reads for the optic nerve and that result has a 95% accuracy. Furthermore, of the 12 patients who had an abnormal optic nerve read, there is a 93% accuracy that imaging provided the correct diagnosis. Teleretinal screening for AMD and cataract had similarly high positive and negative predictive values. Data from this article are consistent with Chow et al. 26 and also consistent with a previously reported prospective comparative pilot study comparing teleretinal imaging with a clinical examination that showed comparable results. 30
Teleretinal imaging for DR showed a high-negative predictive value, but moderately low-positive predictive value. While the data from this study were within the range of sensitivities and specificities reported in a large meta-analysis of DR screening methods, 31 one reason for the lower positive predictive value might be that in the current study, the clinical examination was considered the gold standard. It is possible that ophthalmoscopy may not be the best way to detect DR. 32 –38
There are several limitations of the study based on the nature of the retrospective review. Because this was a retrospective study, there was no possibility to contact patients that were screened and encourage them to return for follow-up. Thus, data on a high percentage of patients were not available. It is possible that the characteristics of the patients who did not return are different from the sample that we assessed and inclusion of these individuals would affect the results. Selection bias also exists for the “normal” patient group because they sought eye care even after having a normal diabetic teleretinal screen. The authors believe many of these patients desired eyeglasses (which they cannot receive during teleretinal screening), especially since Veterans receive spectacles at no cost through the VA. Moreover, for many Veterans, the eye clinic is the only way to access eye care (they lack other health insurance coverage) or Veterans may have been instructed by their primary care provider to have their eyes checked for other ocular disease and then referred to the eye clinic.
For many patients, the clinical examination was conducted several months after teleretinal imaging, and it is possible that clinical findings changed in the intervening time frame. For example, most of the patients with an “abnormal” result through DR screening had only mild disease with a few microaneurysms (MAs) and the evanescent nature of these MAs could explain their absence on imaging and the difficulty of detection during a clinical examination. Another example is the patient who was found to have a Hollenhorst plaque on clinical examination. The particular patient underwent cardiac catheterization after teleretinal imaging and this was believed to be the source for the embolism. Furthermore, the clinicians seeing these patients were not masked to the results of the diabetic teleretinal examinations, which could have influenced their clinical decisions during the face-to-face encounter. Despite these limitations, the current study provides some early qualitative and quantitative data to assess the utility of diabetic teleretinal imaging for the detection of multiple nondiabetic ocular conditions. Data from this study suggests that a true prospective comparison accuracy trial should be done to confirm the findings in this retrospective analysis.
In the current socioeconomic climate of healthcare with a rapidly aging population, there is an increased interest in expanding healthcare delivery in a cost-effective manner. The findings from this study may be used to guide the development of additional protocols that would screen patients for sight-threatening ocular conditions in a primary care setting. For example, the condition that required an intervention in 14 of the 16 patients (88%) might have been detected with a targeted ocular history, intraocular pressure (IOP), and/or a vision at the time of screening. The current study also confirms some of the known limitations of teleretinal screening, which cannot detect peripheral retinal pathology.
The most common reason for a discrepancy between teleretinal imaging and the clinical examination involved patients with increased cupping of the optic nerve. Twenty seven of these patients were found to have a large optic disc and a normal nerve fiber layer, suggestive of physiologic cupping. Combination cameras are now available that can simultaneously obtain both a photograph and an OCT image of the nerve fiber layer. A normal nerve fiber layer on OCT along with a visual field screen such as frequency doubling technique (FDT) may help inform a remote reader whether or not a patient needs a clinical evaluation for glaucoma. The same technology could be used for patients with diabetes to help ascertain the presence of DME—an area where 2D fundus photos are less accurate than the face-to-face examination. For example, assessing vision and/or an OCT of the macula during a remote teleretinal session might help determine if the patient needs to be referred for a clinical examination. “Intermediate clinics” for macular edema using OCT and photography are being developed by the National Health Service in the United Kingdom (P. Scanlon, MD, personal communication). Intermediate screening would allow for more precise triaging of patients who require a clinical examination.
Teleretinal imaging has enhanced the care of patients with diabetes by improving access to eye care, resulting in earlier detection of retinopathy and prevention of visual disability. This study suggests that these same diabetic teleretinal photos, specifically the VA's protocol, may be useful to screen for other sight-threatening diseases such as glaucoma, AMD, and cataract. Adding elements to the current diabetic protocol such as history, vision, and IOP may increase the detection of nondiabetic ocular diseases. Other groups, including this author group, 30,39 have already begun to develop more comprehensive tele-eye assessments. 40,41 For example, a diabetic teleretinal program could add distance vision screening through an eye chart, a method of eye pressure measurement, for example, a handheld tonometer, or both elements to better screen for glaucoma. Several glaucoma screening programs utilize FDT, as well as nerve photographs, pressure measurement, or OCT. 42,43
Finally, as imaging technology advances, it may be possible to utilize teleretinal imaging in combination with OCT to perform follow-up of patients with stable disease. 44,45 Follow-up of patients with stable disease helps to improve patient compliance with visits while simultaneously reduce cost and travel burden. 10,44,45
Conclusion
Diabetic teleretinal imaging has enhanced the detection of sight-threatening DR with improved access to eye care resulting in more individuals being screened for the disease. The same technology appears capable, in this preliminary analysis, to screen for other sight-threatening diseases such as glaucoma, macular degeneration, and cataract. Adding elements to the current photography-only protocol such as history, vision, and IOP may increase the detection rate of these other ocular diseases.
Any comprehensive ophthalmic remote care initiative requires further study to ensure patient safety and to establish accuracy. However, the literature on quality outcomes, patient satisfaction, and the diversity of successful tele-eye programs indicates that teleophthalmology is a viable tool in the fight against visual impairment.
Footnotes
Acknowledgment
The authors wish to acknowledge the staff of VA R&D who helped administratively with this study.
Disclosure Statement
No conflict of interest for any of the authors. The views expressed in this study are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.