
Abstract
Background
In the last decade, the development of Web-based applications has expanded dramatically. 1 A concurrent development in medicine is the promotion of patient-centered care and self-management. 2,3 Web-based applications fit in this trend. They are a useful medium for patient education, stimulation of behavior change, and enhancement of self-management. In addition, Web-based interventions can be implemented on a wide scale at low cost and allow for tailoring, interactivity, and interpersonal communication and provide anonymity. 4,5 This renders Web-based interventions suitable to target common healthcare problems with high costs such as cardiovascular disease.
Web-based interventions targeting single cardiovascular risk factors in adult populations have shown to be effective. 6 –9 However, cardiovascular prevention guidelines recommend a comprehensive approach of the total cardiovascular risk profile. 10,11 It is currently unknown whether Web-based interventions targeting multiple risk factors are also effective.
With global aging, older people form an important target population for cardiovascular prevention. Few Web-based applications for cardiovascular risk management focus specifically on older people. 12,13 The number of people aged 65–74 in the European Union using Internet increased from 20% in 2009 to 42% in 2015, illustrating the high potential of Web-based interventions in older populations. Since older people read, use, and understand Web sites differently than young people, a thorough design process is required to ensure that a Web-based application truly fits this older audience. 14 –16 In this article, we describe the full development, from idea to piloting and implementation, of an interactive Internet platform for older people to improve their cardiovascular risk profile through a multicomponent prevention strategy. We describe all development phases to facilitate others in building on our experiences and move the development of Web-based applications further. In addition, we provide recommendations to design senior-friendly Web-based applications for multicomponent cardiovascular prevention. This platform is especially designed for the Healthy Ageing Through Internet Counselling in the Elderly (HATICE) trial. 17 This is a pragmatic, multinational, multicenter, prospective, randomized, open-label blinded endpoint trial with 18-month intervention and follow-up. The aim of the HATICE trial is to evaluate the effectiveness of the interactive Internet platform to improve the cardiovascular risk profile of older people with elevated cardiovascular risk.
Methods
The concepts of the platform were developed by the HATICE consortium. Close interaction between academic researchers and software builders was key in the development phase. Important spearheads were to design a generic platform that is widely implementable and easily adaptable to different countries and primary care systems. Simultaneously, it should serve as the electronic database for data collection and storage and comply with all security and privacy regulations for good clinical practice. 18 The HATICE trial, including the platform, was approved by the Medical Ethics Committee of the Academic Medical Center in Amsterdam, the Comité de Protection des Personnes Sud Ouest et Outre Mer in France, and the Northern Savo Hospital District Research Ethics Committee in Finland. The platform was developed following five phases as shown in Figure 1.
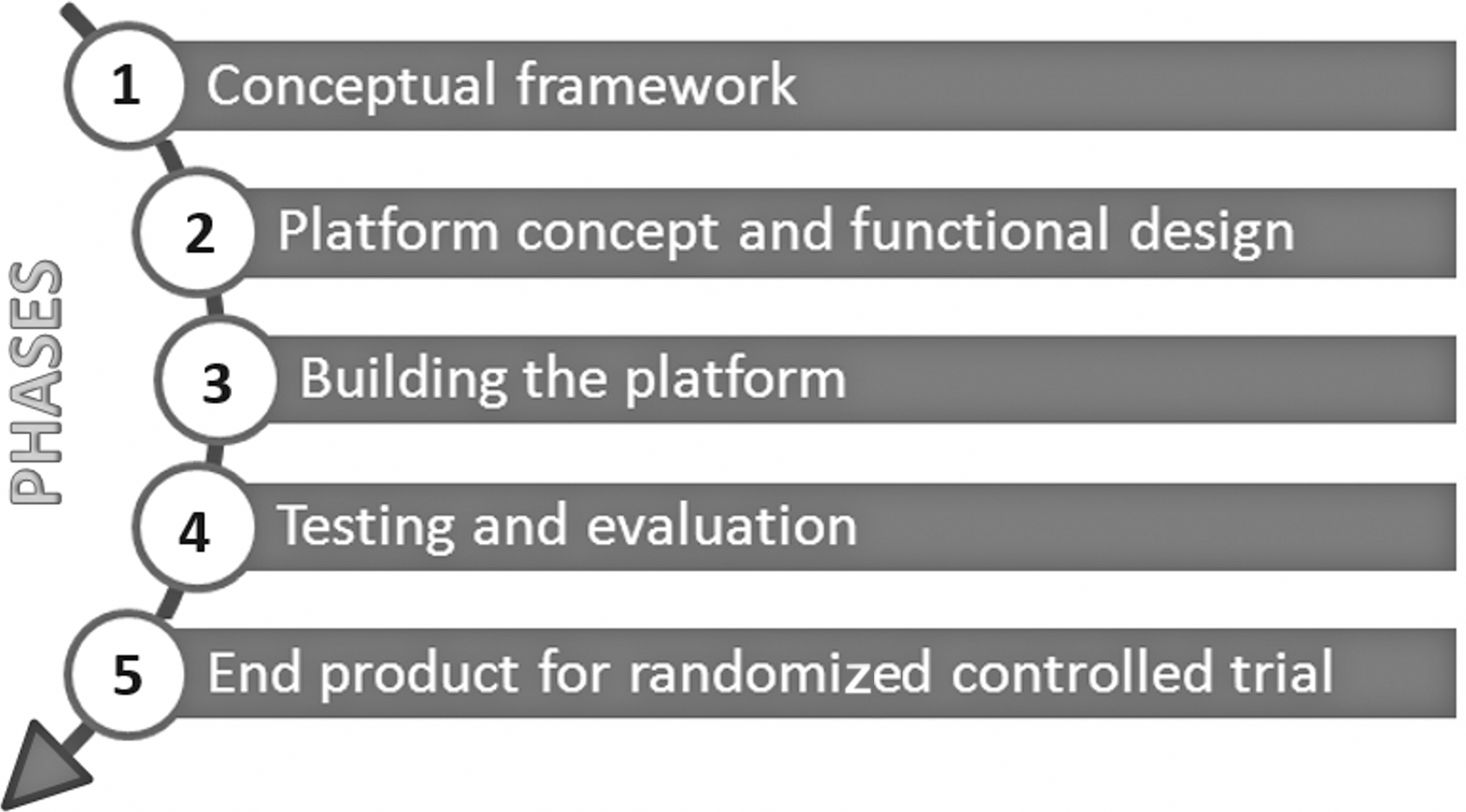
Phases of platform development.
Phase 1: Conceptual Framework
We based the conceptual framework of the interactive Internet platform on Bandura's social-cognitive theory for self-management and behavioral change and its practical elaboration in the computerized self-regulatory system. 19 Successful behavioral change and its maintenance depend on self-efficacy, managing outcome expectations, setting goals, and dealing with barriers. In this system, people are supported in the development of self-regulatory skills in a blended way; by a computer platform and a person serving as online coach. The computer platform can provide an environment for learning, goal setting, action planning, and progress monitoring. The coach evaluates what people are doing within the platform and provides feedback.
We based the HATICE platform on this theory, by combining a Web-based interactive platform for self-management with a personal coach. This coach uses motivational interviewing techniques 20 and the stages of change model 21 as tools to provide feedback and stimulate behavioral change in a cyclic manner (Fig. 2). We used Michie's taxonomy for standardized definitions of the behavior change aspects in our intervention. 22
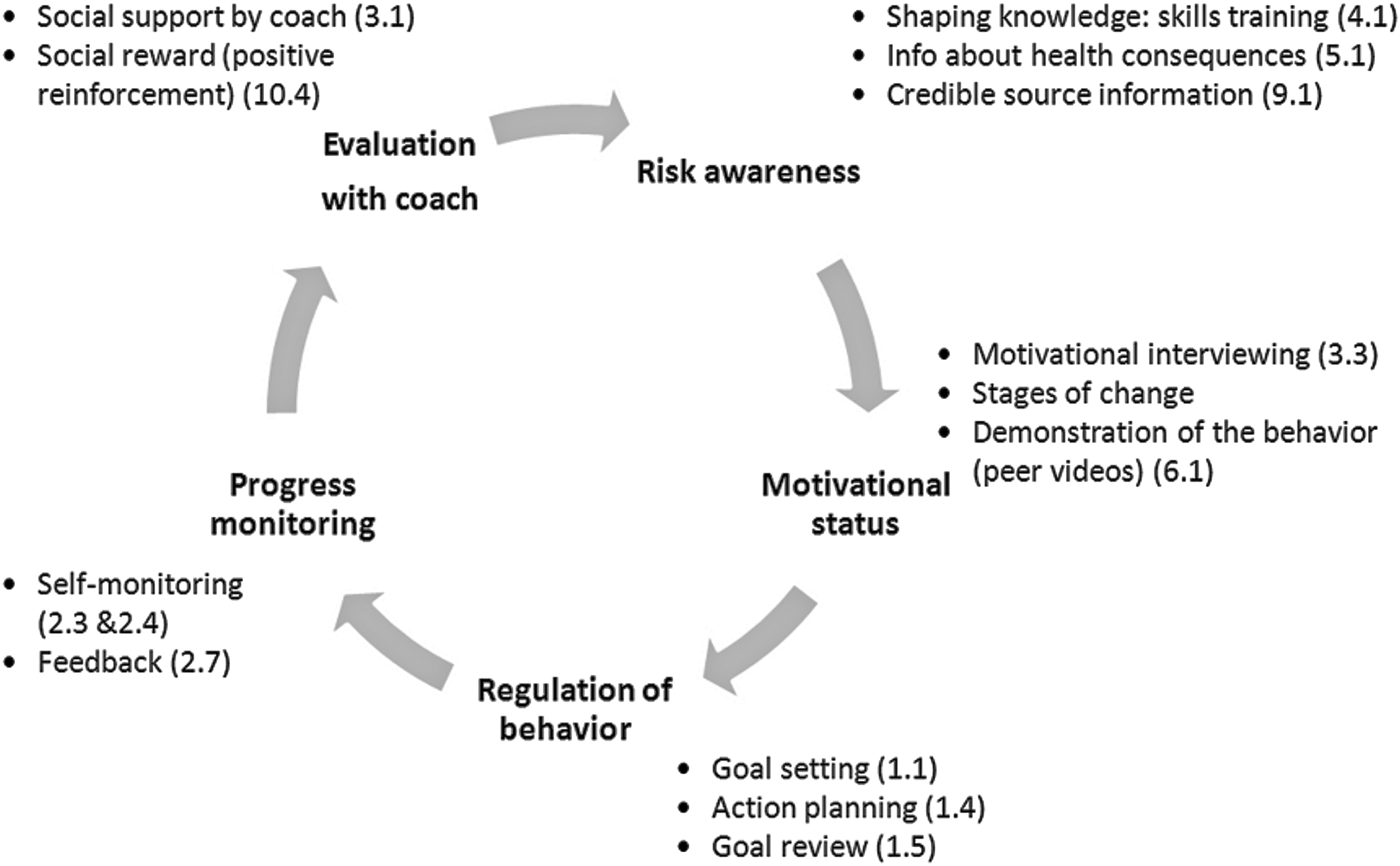
Cycle of self-management supported by the platform and coaching, numbers correspond with the definitions of behavior change techniques from Michie's taxonomy (22).
Phase 2: Platform Concept and Functional Design
We performed a systematic literature review and meta-analysis on the effectiveness of Internet interventions targeting cardiovascular risk factors in older people. 13 In parallel, we conducted fourteen 4-hour brainstorm sessions with academic researchers and software developers to elaborate our concept and the functional design of the platform. We made schematic visualizations of the functionalities and architecture of the platform (wireframes). We discussed this first concept with an expert in health communication among older people, an expert in online lifestyle change, an expert in preventive cardiology, and representatives of patient organizations (Dutch Heart Foundation and the Dutch and Finnish Alzheimer Association).
We organized a total of 10 focus groups with people resembling the target population for the HATICE trial and nurses with experience in cardiovascular risk management in the three countries where the trial will take place (The Netherlands, Finland, and France). To resemble the target population, people had to be older and have elevated cardiovascular risk and basic computer skills. The participants and nurses were recruited from centers that participated in previous randomized controlled trials (RCTs) on cardiovascular risk prevention. During these focus groups, we discussed how an Internet platform could help people improve their lifestyle and which functions the platform should offer. We incorporated the results of the meta-analysis, expert meetings, and focus groups into the final version of the functional design.
Phase 3: Building
Generating the platform content
A prerequisite for platform content was that all information had to be evidence based. We evaluated the European, French, Finnish, and Dutch clinical guidelines on cardiovascular prevention and risk management 10,23 –27 and developed generic modules for cardiovascular risk profile evaluation, lifestyle support, and pharmacological recommendations. To address the complete cardiovascular risk profile, the intervention focused on seven modifiable cardiovascular risk factors (hypertension, dyslipidemia, diabetes mellitus, overweight, lack of physical exercise, smoking, and unhealthy nutrition). 10 We aimed to combine interactive modules with static information, both with a strong focus on self-management.
Building the platform software
The final version of the functional design served as the basis to build the platform software. Software was built using Scrum, an agile software development method, in which small parts of the software are built in iterations. 28 We worked in semimonthly planning cycles in which functionalities of the platform were agreed on, developed by the software developers, tested by both developers and researchers and, subsequently, released. A secure hosting environment was created that complied with strict Good Clinical Practice 18 privacy regulations covered within the local NEN 7510 standard. 29
Building the platform for the control condition of the HATICE trial
In the HATICE RCT, the interactive Internet platform will be compared to a control condition. Therefore, we built a separate control platform. This platform only contains static information modules on the seven cardiovascular risk factors and lacks all (inter)active and self-management features of the interactive Internet platform. There will be no coach support for the control group.
Phase 4: Testing and Evaluation
Prior to the pilot, we performed two testing sessions with Dutch older people representative for the target population. Using the thinking aloud principle, 30 assignments were given to the participants. Tasks included for example: (1) find the Web site using the Uniform Resource Locator and log on and (2) prioritize a risk factor and make a related healthy lifestyle goal. Problems discovered during the test sessions were solved and improvements were incorporated in the platform.
Pilot methodology
The pilot took place in the three countries to test acceptability and feasibility of the intervention and control platforms and the complete study logistics. Detailed study logistics and complete inclusion criteria of the HATICE trial are published elsewhere. 17 Participants were aged ≥65 years and had an elevated risk for cardiovascular disease and basic computer skills.
After eligibility screening, the participants visited the research nurse. They received a welcome email with their sign in details, a short explanation of the platform, and a paper manual. Randomization took place during the visit in a 2:1 ratio. We chose to oversample the intervention group because the main aim was to test the interactive intervention platform. After randomization, participants assigned to the intervention group, made lifestyle improvement goals and received coach support. Participants assigned to the control group received access to the static control platform. Follow-up was 8 weeks. After all participants had completed the pilot, an evaluation session was held in each participating country. Participants completed an evaluation questionnaire (Supplementary Appendix S1a, S1b; Supplementary Data are available online at
Phase 5: End Product ror RCT
After incorporation of the adaptations identified during the pilot, the platform was considered ready for the RCT.
Results
Phase 1, 2, and 3 (Development)
The results from the meta-analysis showed that only few Web-based applications are specifically designed for, and tested in, older people. 13 In addition, Web-based applications can induce small improvements in the cardiovascular risk profile, with larger effects for blended (computer/coach) interventions.
The brainstorm sessions and expert consultations yielded important insight into specific requirements for a platform for older people, including adaptation of font size and the need for a simple and consistent layout with large buttons. To easily absorb information, older people need the platform to be well organized, which can be enhanced by using basic distinctive colors and simple illustrations. Adaptation of default audio settings to people with hearing impairments is required. A concise site map and a limited number of Web pages can facilitate navigation. To prevent loss of motivation, people need to be kept allied to the platform. If people do not login for ∼3 weeks, their motivation might already be disappearing. The experts also advised that a memory training game and other interactive features might stimulate motivation to log on.
From all three countries, 40 older people with elevated cardiovascular risk and Internet skills participated in the focus group sessions. In addition, seven Dutch nurses experienced in cardiovascular risk management participated in two sessions. The target population indicated that older people like to be able to ask questions to a coach through Internet. The platform should have a positive appearance, focusing on health rather than disease, and provide practical and reliable information that is often difficult to find on Web sites. The nurses felt that, to provide adequate support, some face-to-face contact would be indispensable, and also that the platform had potentially added value in providing continuous support on lifestyle change (article currently being prepared by the HATICE consortium).
Content of the intervention
In line with the suggestion to focus on health rather than disease, we renamed risk factors “health factors.” The intervention starts with an evaluation of the personal cardiovascular risk profile, which is generated by the platform from information provided during the study visit. Together with the coach, the participant decides which health factor(s) to prioritize. By doing so, the platform adapts the content of the platform to these health factors and becomes tailored. For each health factor, participants can: (1) set and monitor lifestyle goals; (2) enter health factor-related measurements (e.g., blood pressure, weight, etcetera); and (3) view informative contents. We created a step-by-step procedure that guides the participant to the process of setting goals (Supplementary Appendix S2). The participant sets a target date for the goal and can choose to receive automated reminders. The participant can write messages to the coach using a secured mailbox within the platform. Apart from the virtual presence of the coach, several other aspects of the intervention stimulate (inter)active participation such as interactive information videos and lifestyle groups (Table 1). The lifestyle groups provide an opportunity to connect with other participants and perform healthy activities together in real life.
Features that Stimulate (Inter)Active Platform Use
To keep participants allied to the platform, the coach is automatically alerted if participants refrain from logging on for more than 3 weeks. The coach will then contact the participant to stimulate motivation.
Phase 4 (Pilot Results)
Study population
Recruitment for the pilot started in September 2014 and follow-up lasted until February 2015. In total, 41 participants were randomized (29 to the intervention group and 12 to the control group Fig. 3). Baseline characteristics of the participants are presented in Table 2. The mean age (standard deviation [SD]) of the participants was 69 (4.6) years and 44% were male. Almost half of the participants had a history of cardiovascular disease, including myocardial infarction, stroke, transient ischemic attack, peripheral artery disease, or angina pectoris. The mean number (SD) of cardiovascular risk factors was 2.4 (1.1) per participant.
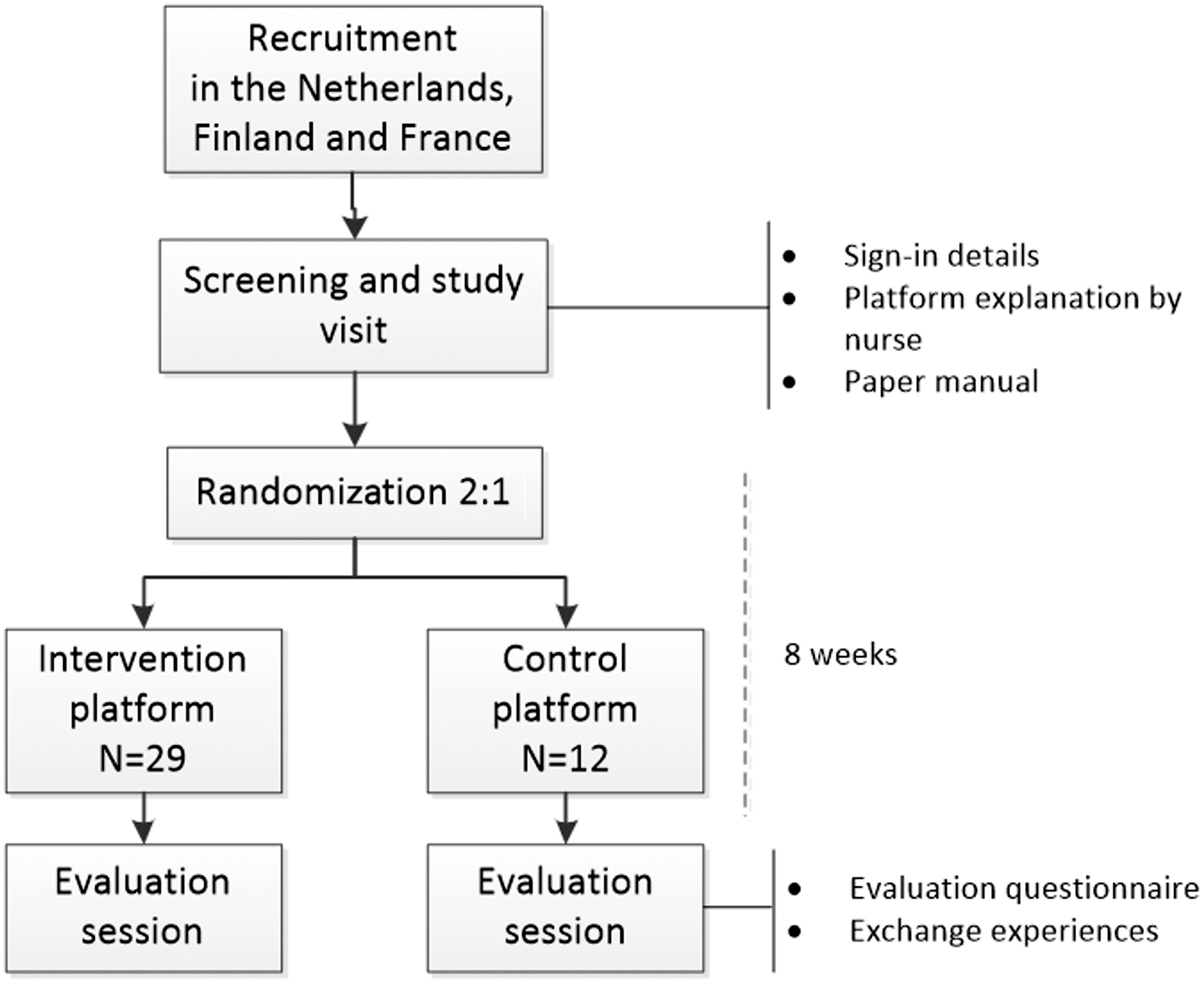
Pilot flowchart.
Baseline Characteristics of All Pilot Study Participants
Two missing values for this variable.
Hypertension: ≥140/90 mmHg for participants <80 years, ≥160/90 for participants ≥80 years, or on blood pressure-lowering agents.
Smoking: any kind of tobacco.
Diabetes: diagnosed by a general practitioner/specialist or on antidiabetic medication.
Dyslipidemia: total cholesterol ≥5.0 mM, LDL-cholesterol ≥2.5 mM, or on lipid-lowering agents
Overweight: body mass index ≥30 kg/m2 or waist circumference men ≥102 cm, women ≥88 cm.
Lack of physical exercise: below the World Health Organization norm of 150 min of intermediate exercise a week.
CVD, cardiovascular disease; SD, standard deviation.
Intervention group (n = 29) and control group (n = 12) combined.
Patterns of use of the Web site
Log-ins: The characteristics of platform use are given in Table 3. Participants logged in 357 times in total, of which 282 times by the intervention group and 75 times by the control group.
Feasibility Parameters of the Pilot Study
Intervention group only.
The coaches logged in 383 times over a total study period of 12 weeks.
Messages: The participants sent in total 74 messages to their coach through the platform. The average content of the messages was about their personal goals and how to achieve them. Participants received a total of 162 messages, including tailored messages sent by the coaches and automatic reminders. The average content of the messages from the coaches was an answer to participants' questions and coaching/motivating the participants in their lifestyle goal.
Goals and measurements: In total, 30 lifestyle improvement goals were set. The majority of the goals were related to improvement of exercise and weight.
A total number of 212 new measurements were entered, mostly pertaining to blood pressure (78), exercise (68), and weight (55). A mean (SD) number of 5.2 (10.3) measurements was entered per participant.
Evaluation session
All pilot participants were invited to the evaluation session and 27 (66%) participants attended. They liked the idea of the platform, but were uncertain what to expect from it. Passwords provided to login for the first time were too difficult. The majority of the participants considered an instruction video necessary. Setting a goal was difficult for participants, although most succeeded with guidance from the coach. Participants appreciated the interactive features of the platform, including goal setting with associated measurement entries and the interactive videos. The information about a healthy lifestyle was appreciated, but the participants liked to print the texts on paper, so an icon to facilitate printing would be useful. The platform did not work optimally with relatively old software and/or hardware. Communication with the coach was very much appreciated and felt very personal to everybody, even though there was no face-to-face contact after the study visit.
Phase 5 (Final Version of the Platform)
The final version of the platform is a secured Web-based platform with personalized secured accounts, where participants can find seven key pages and functionalities as described in Table 4. We have been simplifying the randomly generated passwords. To limit the chances of getting lost on the platform, the navigation structure has been kept as flat as possible. The seven key pages contain functionality that may open a pop-up, but there is no navigation deeper into the platform. The self-monitoring tools and the goal diary have also been simplified.
Key Pages and Functionalities of the Healthy Ageing Through Internet Counselling in the Elderly Intervention Platform
We have been creating an introduction video to provide more guidance on use of the platform. The platform is now accessible on all computer devices (desktop computer, laptop, and tablet) with all major operating systems (Windows®, Mac OS®) and all major browser softwares (Internet Explorer®, Edge®, Safari®, Chrome®, and Firefox®), including older versions. The final platform has a simple and consistent layout style with large font size, limited use of (different) colors, a static main menu that is visible on every page, and clear “return” buttons. The layout of one of the pages of the platform is shown in Figure 4.
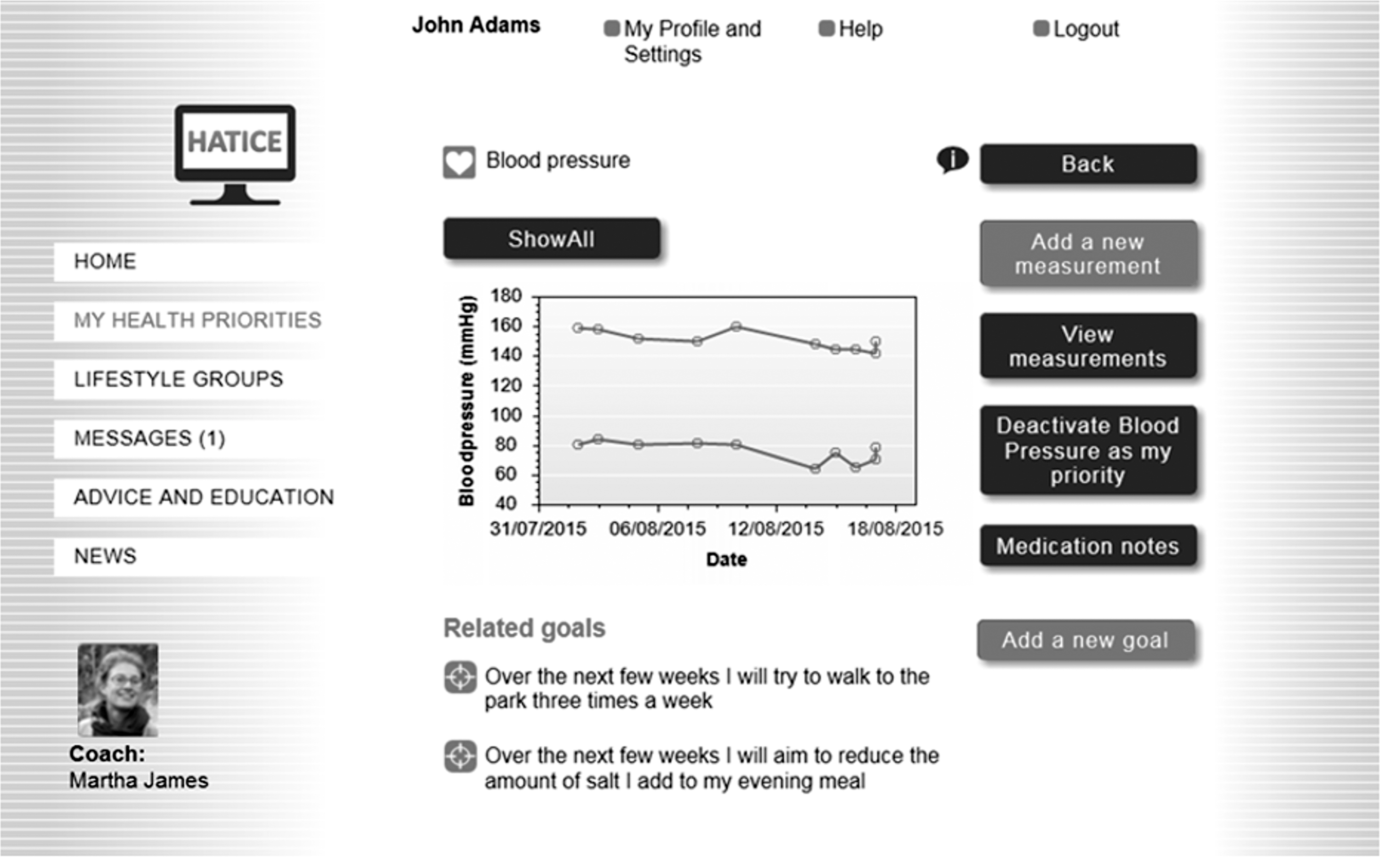
Final version of platform: my health priorities/blood pressure–page.
Discussion
In this article, we described the 2 years of designing, developing, and piloting of an Internet intervention platform to improve the cardiovascular risk profile in older people using a multicomponent intervention strategy. The pilot showed that this platform is acceptable and feasible for use by older people. Literature review and the meta-analysis 13 revealed that blended Web-based applications are associated with larger treatment effects than Internet-only applications. Because of that we enhanced the platform with a coach who could communicate with the intervention group by secure interactive messaging in the platform. We think that this personal touch could strengthen motivation and adherence. The expert consultations and focus groups helped us to understand the barriers older people encounter when using the Internet. Some barriers, such as readability of the Web site and privacy concerns, were already known from previous research. Other barriers, like difficulty with Web site navigation and the preference for a positive tone, were new. The pilot enabled us to determine whether our platform had overcome those barriers and revealed new issues such as difficulties with the login procedure. Simplifying the login procedure seems trivial, but for older people, this can make a huge difference in accessibility.
Over the coming years, the platform described in this article will be tested for efficacy in the HATICE RCT. 17 It is crucial to not only design an evidence-based Internet platform but to test it in a controlled setting as well. In this time of vast digital expansion, technical developments may outpace the research needed to evaluate them. Therefore, some researchers advocate the use of adaptive trial designs for more flexible form of testing. 31 Although this seems appealing, we think that ultimately randomized controlled study designs are required to evaluate clinical effectiveness and utility.
Thorough communication between software developers, researchers, and end users is crucial in understanding each other's visions and needs. The final platform needs a synthesis of the three different viewpoints (clinical trial setting, software capabilities, and senior friendliness). To accomplish acceptability for older people, we recommend starting with a theoretical backbone, involving the end users in the entire process of development and enhancing the application with human support.
If proven effective, the pragmatic design of the HATICE intervention, independent of existing healthcare structures, will facilitate easy and wide implementation throughout Europe. The tailor-made character of the platform is specifically suited to the needs of older individuals and fits with the current trend toward a more personalized and digital approach in medicine.
Footnotes
Acknowledgments
The authors thank the HATICE consortium, Julia van Weert, professor of health communication, Ron Peters, professor of cardiology, Pim Happel, software developer, all participants of the focus groups and testing sessions, and the coaches from the pilot study for their contributions to the development of the platform. The research leading to these results has received funding from the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement No. 305374.
Disclosure Statement
A.S. reports grants from EU-FP7, grants from EU-JPND, grants from Beaufour Ipsen, and grants from France Alzheimer Association during the conduct of the study; personal fees from Beaufour Ipsen Pharma, Pierre Fabre, Lilly, Nestlé, Sanofi, Servier; nonfinancial support from Biogen, Nutrition Santé, Pfizer, Icon; and other from AMPA Association, outside the submitted work. All other authors have nothing to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.