
Abstract
Introduction
African Americans (AA) experience lower life expectancy and higher rates of chronic disease morbidity and mortality relative to their representation in the U.S. population. 1 Specifically, AA have the highest mortality rates for heart disease, stroke, and colorectal cancer. 1 They also have one of the highest prevalence of obesity, hypertension, and diabetes, and the highest infection rate of HIV infection. 1 The lower life expectancy and high prevalence of chronic disease morbidity and mortality rates have been attributed to factors such as institutional racism, socioeconomic status, limited access to and utilization of quality healthcare, environmental conditions, unhealthy lifestyle factors, and the cumulative effects of these factors over the life course. 1 –3
AA have historically been underrepresented in clinical trials and interventions. 4,5 This trend has continued despite the National Institutes of Health (NIH) Revitalization Act of 1993 mandate for the inclusion of minorities in all federally-funded research. 6 The inclusion of AA in more quasi-experimental, observational, and randomized clinical trials would generate data that can be translated into more effective programs for health promotion and disease prevention, rehabilitation, chronic disease self-management, and clinical and pharmaceutical treatment. 7
The use of current and emerging communication technologies to improve or enable health and healthcare (e.g., e-Health) has the potential to increase the scope of research and improve the effectiveness of behavioral interventions aimed at reducing health disparities and improving health equity. 8 –11 In particular, mobile health (m-Health) interventions may minimize many of the common challenges seen in community-based and clinical interventions such as low enrollment, attrition, ease of access, geographic proximity, time limitations, inconvenience, and sociocultural attitudes toward research. 7,12 In addition, m-Health technologies may allow many interventions to be delivered with higher fidelity, lower cost, and minimal time demands on patients, researchers, and clinical personnel. 7,12
Nationally representative data suggest that AA are in a unique position to be potential users of mobile technologies and participate in e-Health/m-Health interventions. While AA are less likely than whites to have broadband Internet at home (49% vs. 66%), 13 they are adopting broadband services at a faster rate than the general population. They are also more likely than whites to own smartphones and to use smartphones as their main source of Internet access. 13 Therefore, numerous opportunities exist for researchers to recruit AA to participate in e-Health/m-Health research. This article reviews (1) the participation of AA in e-Health/m-Health interventions, (2) the diseases/health conditions studied, and (3) the recruitment and retention strategies used.
Materials and Methods
Our search, review, and reporting methods (Fig. 1) followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 14 We also used several other nationally and internationally recognized sources to inform the search strategy. 15 –18
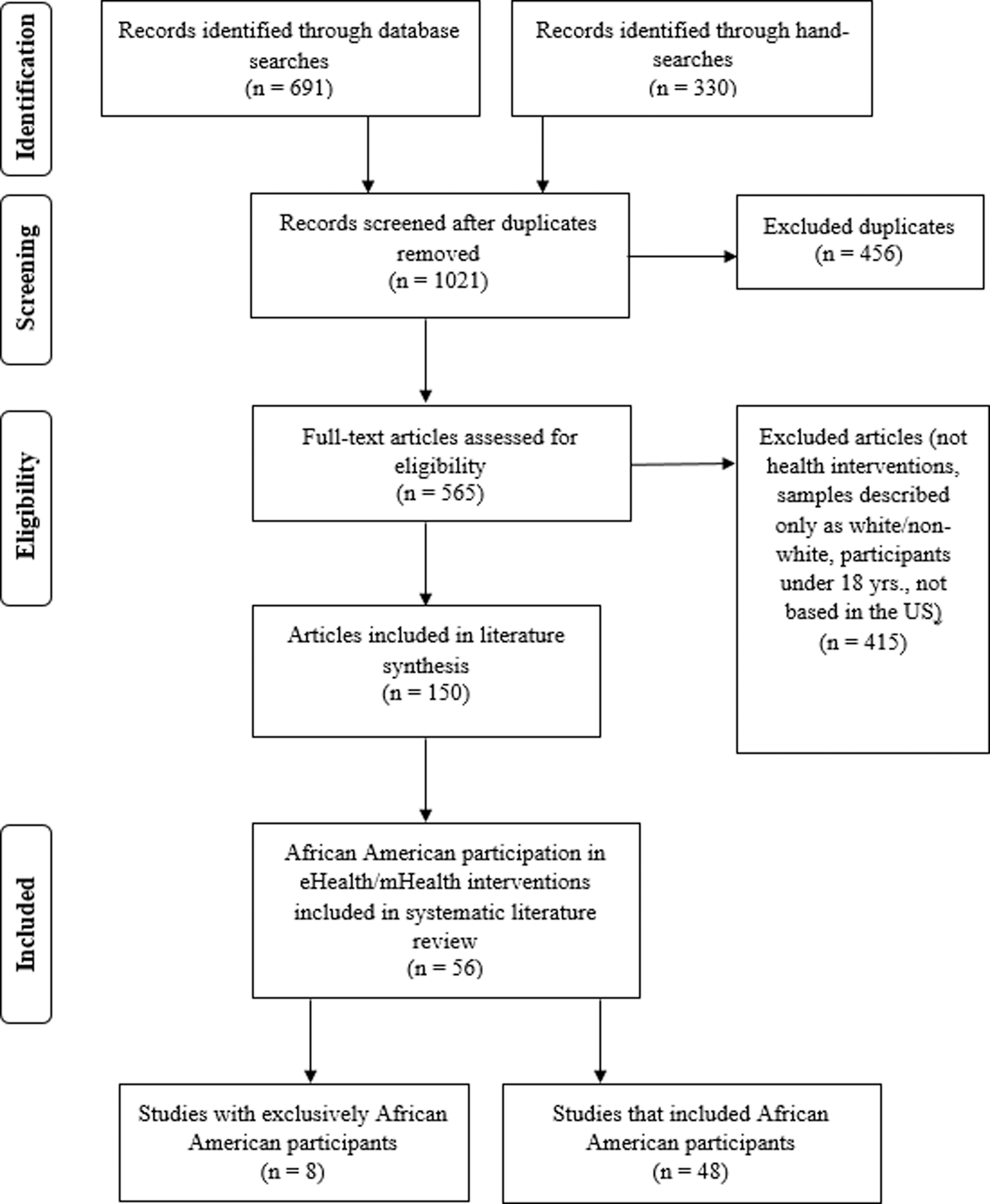
PRISMA flow diagram depicting the search strategy.
Information Sources and Searches
We conducted computerized searches on PubMed, PsycINFO, Web of Science, EBSCOhost, and CINAHL electronic literature databases. In addition, we completed hand searches on 14 journals as shown in Table 1. Searches were done on English language studies published between January 2000 and June 2016. Twenty-three distinct search terms (Table 2) were used alone and in combination in logical sequences using the Boolean operators “AND,” “OR,” “NOT,” and wildcards [* ()?] in the database searches. Boolean operators use wildcard symbols associated to a word to provide for all possible spellings or variations inside a word or word stem.
Search Terms, Journal Hand-Searched, and PubMed and Medline Medical Subject Heading (MESH) Terms
Details of Included Studies
AA, African Americans; BMI, body mass index; COPD, Chronic Obstructive Pulmonary Disorder; IVR, Interactive Voice Response; PTSD, Post-traumatic stress disorder.
represents studies with samples consisting of 100% African Americans
Eligibility Criteria
Only full-text, original e-Health, and/or m-Health interventions conducted as randomized control trials, quasi-experimental designs, mixed methods, and embedded nonexperimental designs were considered. The study's inclusion criteria were as follows: (1) published in English, (2) conducted in the United States, (3) AA adults (≥18 years), and (4) specified the type of technology (e.g., online or text message) used in the studies. Studies were excluded if race/ethnicity was not specified (e.g., nonwhites). We extracted data on sample size, gender, recruitment and retention strategies, and illness/disease studied.
Data Collection, Management, and Analysis
Four graduate students independently extracted and coded the data, and the project supervisor resolved any discrepancies. Full texts of the articles were subsequently analyzed to ensure that the studies in the sample fully met inclusion criteria. Duplicate studies were eliminated using DigitalVolcano 4.0, a duplicate cleaner application (
Studies that met the inclusion criteria were coded into an electronic database using the evaluation rubric developed for this analysis. After the first coding phase, the researchers used a matrix that denoted participants by race/ethnicity, study purpose, e-Health/m-Health intervention type, study, disease/condition studied, and recruitment/retention strategies.
Results
We identified 1,017 studies from the database searches (n = 691) and the hand searches (n = 330). After duplicate removal, 565 full-text studies were screened and assessed for eligibility. Fifty-six studies met the inclusion criteria (Fig. 1) and these studies made up the final sample (Table 2). Fifty-two percent (n = 29) of the studies in the final sample disclosed funding support from NIH.
Participant Characteristics
The reported sample sizes ranged from n = 17 to n = 2,318. 19,20 Most studies (n = 29, 52%) had a participant sample of 100 or more. The studies with the smallest sample sizes were pilot studies (n = 8). 19,21 –27 Three studies had sample sizes of n ≥ 1,000. 20,28,29
Only 14% of the studies (n = 8) enrolled exclusively AA participants. Of the remaining (n = 48) studies, more than half (n = 27, 56%) had less than 25% AA participants. Of the 27 studies that had less than 25% AA participation, 12 reported AA participation of 10% or less. 20,24,25,30 –38 The remaining studies (n = 21, 38%) reported samples with 26% or higher AA participation.
Eighty percent of all the studies (n = 45) consisted mostly of females. Fourteen studies (25%) had only female participants. 21,22,26,29,30,38 –47 Two studies focused on prostate cancer, and thus only had men. 29,39 More than half of the eight studies (63%) with exclusively AA participants (n = 5) had only female participants. 21,41 –43,48 Two studies had 96% and 92% female participants. 24,49
Most studies (n = 42, 75%) consisted of adults more than the age of 40, with four samples being exclusively AA. The four studies with exclusively AA included a tailored Web-based physical activity promotion intervention 41 ; a pilot study on a Web-based intervention to promote fruit and vegetable consumption 24 ; a computer-based behavioral intervention to enhance hypertension medication adherence 50 ; and a diabetes e-Health program for AA adults with low diabetes literacy. 51 Two studies had more than 70% AA participation. 52,53 One of which used cell phones for health counseling among smokers with HIV/AIDS and uniquely had 70% male participants, which was one of the few studies in the review with women that had a majority male sample. 52
Seven studies had participants between the ages of 30 and 40. Two of those studies had samples that were exclusively AA. One used interactive voice response (IVR) technology for self-monitoring of weight and the other used a combination of Facebook and texting to increase physical activity. 42,48 Five studies included AA aged 30–40 in the sample and included a Web-based pedometer program to prevent gestational diabetes 22 ; a Web-based intervention to promote physical activity among a disabled population 23 ; a podcast weight loss intervention 54 ; a self-monitoring and remote coaching intervention targeted to multiple behavior change in diet and activity 55 ; and a m-Health physical activity intervention. 39
Seven studies (13%) had participants in their 20 s, and two of those had exclusively AA participants. Of the two studies with exclusively AA, one study used Web-based strategies to address HIV and sexual health, 43 and the other examined physical activity and overweight/obesity. 21 Of the other five studies with participants in their 20s, two used text messaging for pregnant women 30 and prenatal care, 44 one examined Facebook as a platform for an overweight/obesity intervention, 56 while another examined Facebook as a platform for weight loss messages, 36 and the fifth used smartphone apps, self-monitoring, and personal health coaching for weight loss. 57
Recruitment and Retention Strategies
Slightly more than half of participants (n = 29, 52%) were recruited in a clinical setting (private medical practices, public health clinics/community health centers, hospitals, or electronic medical records). Several studies recruited through flyers, newspaper, public service announcements, etc. (n = 14, 25%) and through electronic websites, listserv, email, or postal mailings (n = 8, 15%). Three studies actively recruited participants from churches (n = 2) and a college campus (n = 3, 5%). Several studies used multiple recruitment strategies, notably one cancer study recruited from five different sources including oncology clinics, tumor registry, Facebook, online cancer resources, and other online sources. 58 Two studies did not describe any recruitment strategies. 35,59
Most studies (n = 31, 55%) did not report providing any incentives for recruiting and/or retaining participants. Studies that recruited through medical records did not report using incentives. Forty-five percent of the studies (n = 25) reported giving some type of incentive. Nineteen of those (76%) used monetary incentives (e.g., cash or gift cards). The value of cash/gift card incentives ranged from $10 to $175. One study provided a $175 incentive for meeting the goals for both targeted behaviors during the treatment phase and additional financial incentives ($30–$80) for uploading data during consecutive follow-ups. 55 Notably, one study offered participating churches $1,000 for each assessment phase plus an additional $500 if 95% of participants returned for follow-up assessments. 28 One study reported providing compensation, but did not specify the amount. 40 Six studies (24%) used nonmonetary incentives. The most common nonmonetary incentive was prepaid no contract cell phones. 21,44,60,61 Notably, one study offered free hypertension medication for the duration of the study, 50 and another study provided participants with a free gym membership. 48
Only 10 studies (18%) addressed retention of participants. One study reported higher retention rates (81%) among breast cancer patients in the treatment group that provided a peer advocate in the use of an e-Health application compared to those that did not receive peer support. 47 A weight loss study reported a retention rate of 87% for the intervention group; however, no analyses were provided about those that dropped out. 45 One study of an online diabetes prevention program used a unique approach where coaches texted or called participants who did not log in for 21 consecutive days. 33 Nonrespondents were considered “inactive” until they logged in again. 33 One study used a single reminder to utilize the system after a 48-h period with no interaction. 49 Another study staged incentives as part of the retention strategy by providing incremental incentives for each assessment phase. 28 The researchers also leveraged positive social pressure by offering an additional $500 to churches that had ≥95% of their participating congregation return for follow-up assessments. 28 Incremental incentives were used by another study, but all the incentives earned were provided at the end of the study. 55
Finally, although not reporting retention/attrition rates, three studies oversampled in anticipation of higher attrition, 62 –64 whereas another study described that increased human interaction with regards to e-Health studies could reduce attrition. 65 Only four studies reported attrition or retention rates. 20,35 A HIV/AIDS study lost overall 27% from the intervention group and 17% from the control, however, found no significant effects due to attrition on the baseline measures. 66 A smoking cessation study reported an attrition rate of 80%, 20 and another study reported a significant difference in retention rates between the three study groups: (1) standard treatment (53%), (2) standard treatment + technology (100%), and (3) technology only (77%). 35 Another study reported an attrition rate of 37.8% and found that those that completed the study were more likely to be Caucasian, female, and educated compared to noncompleters. 67
Health Conditions
Most interventions (n = 33, 59%) were delivered online. Other interventions were delivered through text 19,27,30,37,42,44,56,67 or email messages, 67 IVR, 26,47,48,68 Facebook, 36,42,56 podcast, 54,69 telemedicine, 70 and by phone using motivational interviewing 71 as shown in Table 2. The diseases/health conditions represented in the sample are shown in Figure 2. Nine studies (16%) examined two or more health conditions. Studies that focused on multiple health conditions included: HIV prevention behaviors among AA women seeking sexual health services at a Planned Parenthood clinic 43 ; posttraumatic stress disorder (PTSD), depression, and chronic pain among female veterans 46 ; physical activity and type 2 diabetes patients 22 ; diabetes prevention and obesity 72 ; chronic pain and physical inactivity 73 ; physical activity and overweight/obese female college students 21 ; decreasing cardiovascular risk among overweight/obese patients 31 ; and reducing blood pressure in obese patients taking antihypertensive medication. 68

Frequency of health conditions in study sample.
Discussion
There is a gap in the literature regarding the participation of AA in e-Health/m-Health research. In this systematic literature review, we sought to identify the participation of AA in these types of interventions, diseases/health conditions studied, and recruitment and retention strategies used. Examining AA participation in this accelerating branch of health behavior research is critical to advancing the nation's health disparity research and achieving the letter and spirit of the 1993 NIH Revitalization Act. 6
There was a low representation of AA in the studies in this review. In addition, several studies were excluded from the review because the racial/ethnic demographic data of the participant pool were either not disclosed or separated only into “white” and “nonwhite” categories. The low representation of AA in research may be more a reflection of ineffective, culturally inappropriate recruitment and retention strategies rather than a lack of interest by AA. 74
While mistrust and skepticism of research may still exist among many AA, it may be less pervasive than in previous decades. Indeed, results from two recent studies found that most of AA surveyed expressed willingness to participate in e-Health/m-Health research. 75,76
The rapid pace of AA adoption of mobile technology, specifically the use of smartphones as the primary mode for Internet access, suggests a need for more innovative recruitment and retention strategies. In addition to being culturally appropriate, these strategies may also need to be tailored by gender and age group. 75,76 Younger AA are more likely to own smartphones and have different health concerns than their older counterparts. Our results suggest that the lag of AA male participation in traditional public health research has been carried forward into e-Health and m-Health research.
Efforts to engage AA males in research using e-Health/m-Health technology deserve further study. Studies have shown that AA women are generally more interested than their male counterparts in improving their health habits 77 and have reported willingness to participate in e-Health/m-Health research as a factor of personal interest in the study topic, opportunity to become more educated about the topic, and to generally contribute to the greater good. 76 More effective recruitment and retention strategies should focus on leveraging the influence of AA women within their families and communities.
A variety of strategies were used to recruit participants into the studies. Most studies were recruited through clinical settings and electronic medical records, which may be a viable approach for healthcare-based research. Studies recruiting from these settings may want to consider using an “opt-out” letter approach, which has been shown in traditional studies to shorten recruitment time and increase the participant pool compared to the “opt-in” letter approach. 78 Studies were also more likely to use a single recruitment strategy even though research suggests that a multilevel recruitment approach that considers culture, learning styles, and personal engagement may result in a larger more diverse participant pool. 78,79
The efficacy of church-based health promotion programs has been well established in the literature, 80,81 but only two studies in this sample used church congregation recruitment strategies. 24,28 AA churches have well-established social networks that can facilitate the successful recruitment into research studies. 80,81 Furthermore, a community-based recruitment approach fosters trust and identifies individuals who are likely to be interested and motivated to participate in research. 78 In addition, studies have shown that recruitment strategies that involved some degree of interpersonal engagement or community outreach may increase enrollment rate. 78,79 This fact should not be lost on researchers conducting e-Health/m-Health studies. Whether the intervention exclusively uses Telehealth or mobile technology tools or uses them as a component, it appears that some personal engagement at the recruitment stage may be vital for a high enrollment and retention rate. 78
Ten studies mentioned retention strategies, with some providing more details than others. The studies that described retention strategies were different in so many ways that comparisons could not be made. Studies that provided incentives periodically or at the end of the study appeared to have a better retention rate. Retention strategies that are usually recommended in the literature with traditional studies include providing accessible locations, frequent reminders, and timely payment of incentives. 78,82 The latter two strategies are especially relevant to e-Health/m-Health studies, but funded research should make more effort to publish the strategies used. Study protocols should also require research staff to record the number of participants approached and the number that refused to participate.
The heterogeneity of the sample in the present study and the variety of incentives used prevented a reliable meaningful comparison of incentive strategies. One systematic review that compared the use of incentives in psychology, economics, and health behavior research reported that behaviors and incentive schemes differ greatly in moderating behavioral characteristics. This study also stated that uncertainty remains about the type and structure of financial incentives that would work for specific groups, communities, and targeted health behaviors, which would lead to sustained behavioral change. 83 Thus, researchers must continue to seek innovative ways to incentivize participation in e-Health/m-Health studies. They also must go beyond the traditional one-size-fits-all approach to determine what mixture of incentives and recruitment/retention strategies would work best for a particular health condition, population group, or community.
Most of the studies in this review addressed diseases and conditions that are of public health importance. 2 Specifically, more than half of the studies focused on overweight/obesity, physical activity, cardiovascular disease, and diabetes. Other opportunities also exist to design and implement more e-Health/m-Health studies that target young tech savvy AA who are engaged in social media (e.g., HIV, smoking cessation, alcohol and drug abuse, unplanned pregnancy, and breastfeeding). 75,76 Recruiting a diverse pool of AA in more e-Health/m-Health studies will provide data that can be translated into more effective programs and treatment that may ultimately impact healthcare cost, health outcomes, healthcare quality, health equity, and overall quality of life. 2
Limitations
There are some limitations to this study. We used specific search terms, which may not have captured all the articles on the topic. Publication bias, or selective publication of studies, is an ever-present limitation in the existing world of academic publishing. We did not seek out unpublished studies to include in the literature review. We included randomized control trials (RCTs), quasi-experimental designs, mixed methods, and embedded nonexperimental designs; most of the studies in our sample were RCTs, but no quality appraisal was performed. Five of the studies in the sample were pilot studies, and there was a high degree of variability in the objectives and outcomes. Many of the studies included in the systematic review enrolled relatively small patient populations; future studies should assess the sample size required to have an adequately powered design and allow for a more generalizable population to assess the effectiveness of e-Health and m-Health research among AA.
Conclusion
This systematic review of the literature found a limited representation of AA in e-Health/m-Health research even though they continue to experience high rates of health disparities for many diseases. E-health/m-Health research interventions have great promise for public health impact by delivering evidence-based interventions to a wide audience at relatively low cost. However, if we are to achieve reduced health disparities and achieve health equity through designing and implementing effective e-Health/m-Health clinical and community-based research and interventions, the traditional ineffective methods used to recruit and retain AA in traditional research cannot be used.
Researchers must acknowledge the critical role of culture, attempt to explore the cultural appropriateness of these interventions with AA, and engage community members in recruitment and retention efforts, even while they explore and leverage recent and emerging technological advances. The ubiquity of no-contract mobile phones, unlimited talk/text/data mobile plans, and access to low-cost smartphones has resulted in an increasing democratization of technology and the Internet. By addressing these issues, researchers will be better able to evaluate the efficacy and effectiveness of long-term e-Health/m-Health interventions and translate these findings to improve the health outcomes in ethnic minority populations.
Footnotes
Acknowledgment
The research leading to this publication was supported by an internal seed grant from the University of Florida.
Disclosure Statement
No competing financial interests exist.