
Abstract
Introduction
Telemedicine is the delivery of healthcare and the exchange of healthcare information between physically distant clinical sites using both information technology and telecommunications. The process assumes an intrinsic didactic relevance, because clinicians skilled or trainees participate through telemedicine with experts at tertiary centers to formulate a diagnosis or plan the best patient management. 1
Telemedicine permits the management of healthcare across distances especially in rural areas of developed and developing countries, where pregnant women live many kilometers from their nearest obstetric unit. As an example in Arkansas, telemedicine is fundamental for pregnant women with medium to high risk who are not accepted in the local obstetric units and cannot move up to the University for routine visits. 2
Telemedicine technology programs are also required over relatively short distances as they could avoid unnecessary referral to tertiary centers, with advantages for the women and their families. In Campania region (Italy), the average population density is about 424 inhab/km2. The largest city is Naples with a reported population density of 2,608 inhab/km2, which reaches a peak of 13,322 inhab/km2 in the “municipality” of Portici. Naples has municipalities that are more similar to submetropolitan areas, districts (and subdistricts) characterized by a decentralization of services. Each of them enjoys organizational and functional autonomy also for health, where Level I and II local centers are connected to few Level III centers (Hospitals). Travel time to reach the tertiary referral hospital often stretches/ extends unpredictably, although distances are relatively short. The time interval between the arrival of a patient at the hospital and his/her entry in the surgery is on an average more than 3 h because of the large number of patients.
In this context, telemedicine becomes crucial in the management of risk pregnancy, which requires an integrated evaluation of the most established and well-known methods of fetal surveillance: Doppler ultrasonography and the electronic fetal heart rate (FHR) monitoring. 3 To improve the assessment of fetal well-being, our region provides a computerized Cardiotocography (cCTG) system, which uses a standardized method to evaluate quantitative parameters of FHR variability. 4,5
The TOCOMAT system for telecardiotocography 6,7 was the first Italian Prenatal Telemedicine network providing five times a week specialty consultations and second opinion to clinicians' sites throughout the Campania region. The project was developed by the “Federico II” University Hospital of Naples in 1998 with the aim of extending the cCTG service to pregnant women with medium to high risk, requiring intensive FHR monitoring.
This “interactive” technology allows the CTG recording “near home,” the transmission of quality clinical data unambiguously, and the quick responses of experts for diagnosis and clinical management of pregnant women, to reduce frequent and often unnecessary travels to Level III center.
From the start date to 2006, TOCOMAT network was supported by the University Federico II of Naples and the Campania Region and was included in several projects always financed by the Campania Region (NEUROMATIC project, 2000; CYBERFETUS project, 2000) and the European Union (European Project of Telemedicine, 2003). 7,8 At first, the system involved nine local Remote Units and one foreign, thanks to a scientific cooperation between the University Federico II of Naples and the Semmelweis University of Budapest—Hungary (EUROTOCOMAT project, 2004). 9 Since 2007, the number of Remote Units involved has gradually reduced to just five units currently operating, despite the addition of new foreign units, including the Instituto Nacional Materno Perinatal in Lima—Peru for the years 2011–2012, due to their high cost.
The aim of the present study was to evaluate the real impact of the TOCOMAT network from its starting date until today in the different areas of Campania region, considering the sociocultural and healthcare inequalities and their changes over time.
Materials and Methods
TOCOMAT network consists of an Operations Center located at the “Federico II” University Hospital of Naples and Remote Units located at Level I and II centers of the Campania region.
CTG monitoring was performed in a controlled clinical environment with the patient lying on a bed or an armchair. According to ACOG guidelines, 10,11 the frequency between assessments ranged from weekly to daily in particular risk conditions, and the standard period of recording was 20 min.
Each Remote Unit is equipped with a cardiotocograph Philips Viridia 50A Antepartum Fetal Monitor that records the FHR trace with the clinical data on the pregnancy and sends it to Operations Center through modem.
The Operations Center has the OB TraceVue Fetal Monitoring System (Philips) that makes it possible to acquire simultaneously as many traces as cardiotocographs are connected, through the identification of the CTG device. The recording is showed on a display, stored on a hard disk, and transmitted to the 2CTG2 system, 12 which perform a complex FHR analysis, using algorithms elaborated by the University of Pavia and the Politecnico di Milano (Italy). 4,13
An Internet or phone conference calling is available to discuss the information transmitted before reporting. The interpretation of cCTG parameters and clinical recommendations are made according to ACOG guidelines and Arduini's tables. 10 –12 At the end, the report is send back to the Remote Units through e-mail.
As further equipment, inside the Operations Center there are four cardiotocograph Philips Viridia 50A Antepartum Fetal Monitors connected to the network directly and four portable Corometrics 170 (General Electric). The latter used a wireless connection to perform the trace at bedside and to transmit it, with pregnancy related data, to a Smart Phone using a Bluetooth wireless port. The Operations Center has the Trium CTG Online system to receive, display, and store the traces and patient data recorded by portable cardiotocograph and to send them to the 2CTG2-Trium option software for the computerized analysis. Finally, Operations Center sends to the Smart Phone, through e-mail, the report of computerized analysis (Fig. 1).
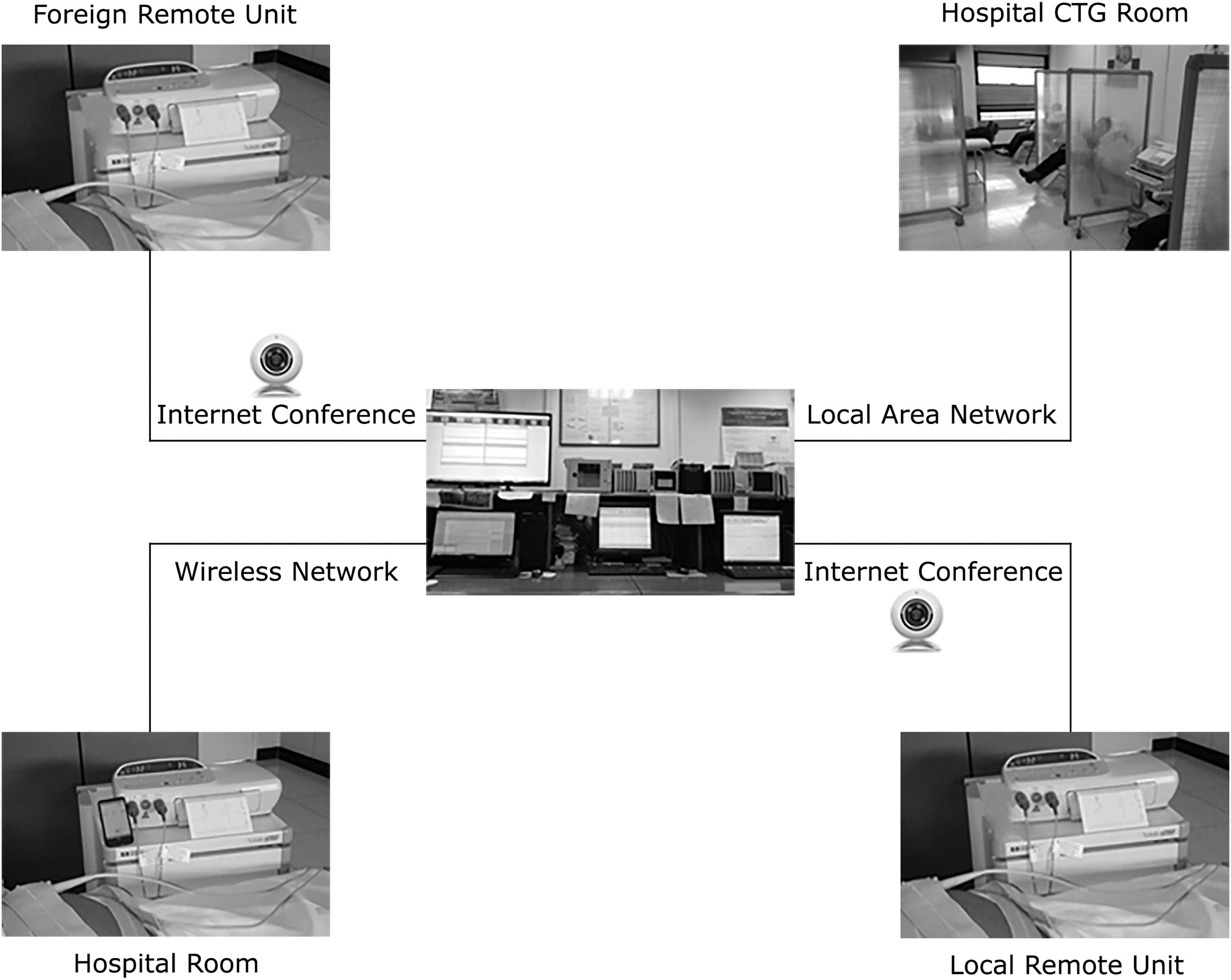
Operations Center is shown in the center of the figure. Hospital CTG Room: located inside the Operations Center and equipped with four cardiotocographs connected to the network directly. Hospital Room: located inside the University Hospital and equipped with portable cardiotocographs connected to the Operations Center with a wireless connection to perform the trace at bedside. Local Remote Unit: located at Level I and II centers of the Campania region and equipped with a cardiotocograph that records the FHR trace with the clinical data on the pregnancy and sends it to the Operations Center through the modem. Foreign Remote Unit: located in a foreign country and working as a Local Remote Unit. CTG, Cardiotocography; FHR, fetal heart rate.
In the last 5 years, we tuned up an improved algorithm to allocate pregnant women with indication to computerized FHR analysis and to establish when the examination should be repeated, to prevent an inappropriate use of telemedicine.
Figure 2 shows the type of interaction between Remote Units and Operations Center for pregnancy management. All low-risk pregnant women performed a weekly CTG monitoring from the 37th week of gestation. In case the trace was not reassuring, the gynecologist of the Remote Unit send the recording to the Operations Center to perform the computerized analysis. If the computerized analysis is not reassuring, the pregnant woman repeats the cCTG monitoring later in the same day or the next day and if it is still not reassuring the gynecologist plans a check to the Operations Center in a few days. All medium to high-risk pregnant women performed the cCTG monitoring weekly. 10 In case of trace not reassuring, the gynecologist extends the monitoring period and plans a complete check to the Operations Center for further investigations or interventions. If the trace is still not reassuring, the woman is admitted in hospital after counseling on clinical management and that she will perform the cCTG monitoring daily until delivery. On the contrary, if the check is reassuring the patient returns to the Remote Unit for weekly to daily monitoring. In case of pathological cCTG trace, the pregnant woman is quickly sent to the nearest hospital to perform an urgent or elective cesarean section according to pregnancy risk conditions.
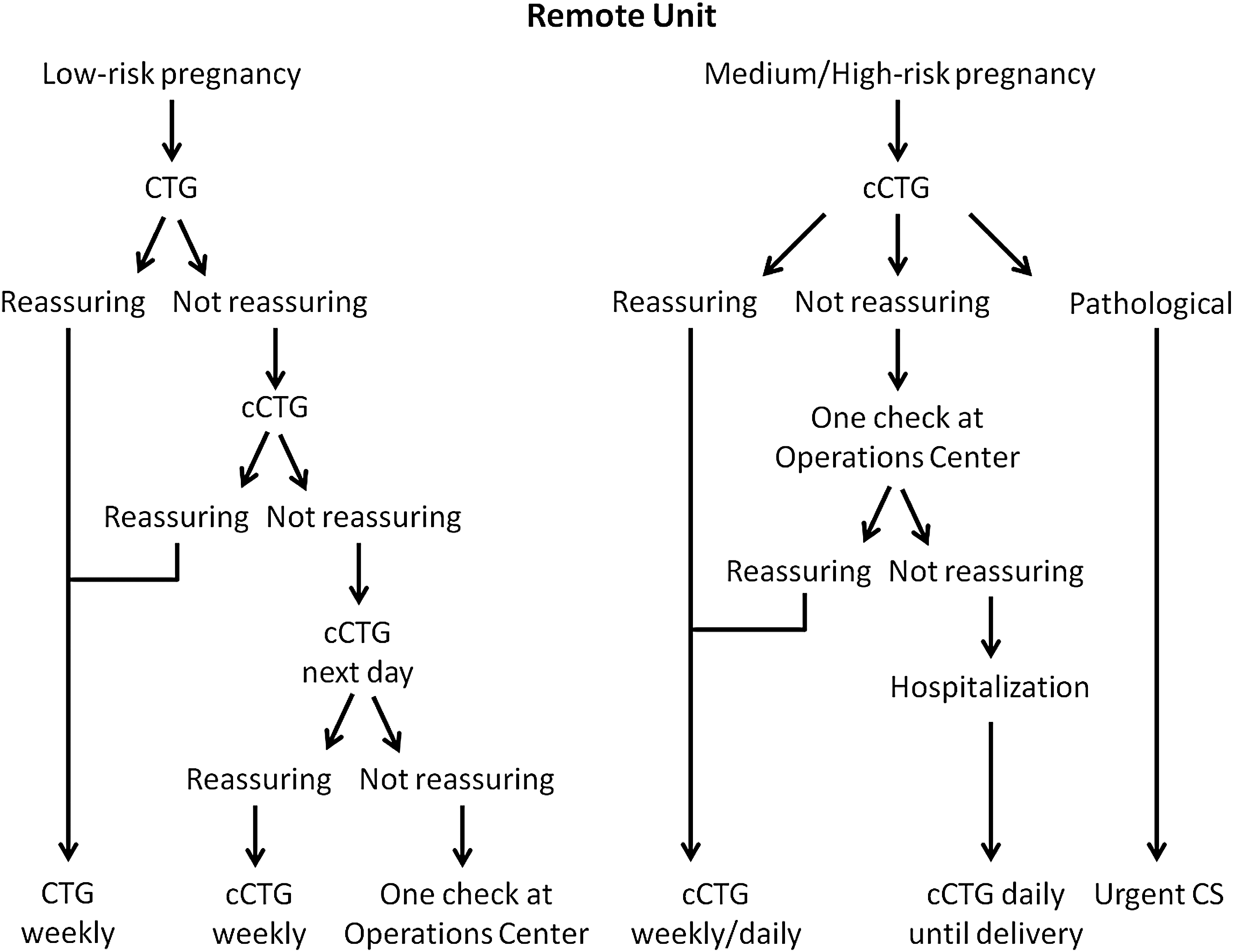
The classification of the cCTG traces in “reassuring,” “not reassuring,” and “pathological” was made according to ACOG 12 guidelines on antepartum fetal surveillance. cCTG, computerized Cardiotocography; CS, Cesarean Section.
Cardiotocographic Measures
The 2CTG2 software computes a set of standard parameters in time domain, frequency domain, and index from nonlinear analysis. Results in a large population of fetuses with normal development and affected by pregnancy complications confirmed the usefulness of this multiparametric analysis of FHR. 4,13
Results for the Population: Impact on Healthcare System
In the recent years, there was a strong reduction of teleconsultation service with only four Remote Units currently active, while the number of cCTG traces performed at the Level III center was constantly increasing, arriving at a total of 5,478 performances in 2015 with an increase of +550% since 1998 (Fig. 3).
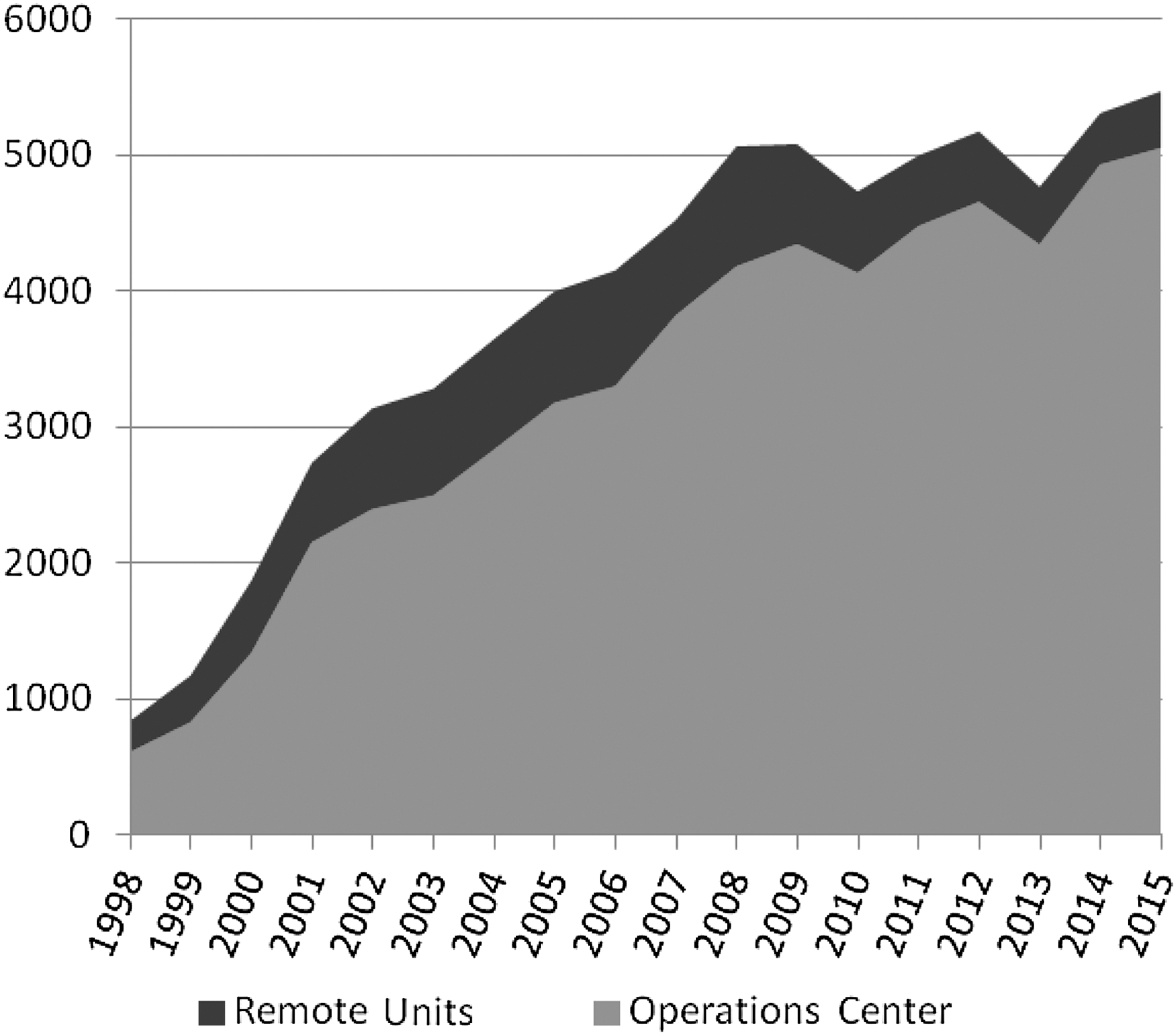
Remote Units was the sum of the cCTG traces performed in the Local and Foreign Remote Units, from 1998 to 2015 divided for years. Operations Center was the sum of the cCTG traces performed in the Operations Center, from 1998 to 2015 divided for years.
Our experience of more than 70,000 cCTG traces allowed to analyze the prevalence of the most common obstetric complications, the socioeconomic context in which they developed, and their trends over time. Table 1 summarizes the characteristics of pregnant women in Operations Center and Remote Unit groups.
Revision: Maternal Characteristics Based on the Location of Pregnant Women
Values above are expressed as mean value ± standard deviation.
Physiologic: low-risk pregnant women; others: previous stillbirth, severe Rh isoimmunization, oligohydramnios, hyperthyroidism, and cyanotic heart disease.
Proportion (%) of persons below the national poverty level.
Respect to their geographical distribution in the Campania region.
The municipalities of the Campania region were subdivided in quintiles with respect to the value of the DI (the first represents the most wealthy, the fifth the most deprived). We reported the proportion (%) of the fifth quintile of the DI. DI includes five socioeconomic variables showing the strongest association with mortality: proportion of population with only primary education; proportion of unemployed among active population; proportion of population not owning its dwelling; proportion of monoparental families; and average surface of dwellings.
cCTG, computerized Cardiotocography; DI, Deprivation index; IUGR, intrauterine growth restriction.
Source: Fazzo et al. 19
t-Test revealed a significant difference for maternal age, body mass index, and weight gain between the two groups (p < 0.05). In fact, pregnant women in Remote Units were younger and overweight than Operations Center ones. No differences were found for gravidity, parity, gestational age at cCTG recording, and duration of cCTG recording (p < 0.05). Chi-square test showed significant differences for all ethnicities, educational levels, and poverty level between the two groups, with higher rate of African migrant women and lower educational, socioeconomic, and cultural standards in Remote Unit group. In addition, the proportion of toxic dump sites around Remote Units was higher than Operations Center ones. Finally, two clinical indications such as diabetes and malformations were more frequent in Remote Unit group (p < 0.05).
Discussion
Obtained Results
The constant reduction of Remote Units is the effect of the global economic recession, 14 which has had a significant impact on the Italian regional healthcare system. The high public debt and the subsequent cost-cutting strategy have involved the investments for health information systems, limiting the maintenance and replacement of the obsolete equipment in Remote Units. This phenomenon has resulted in the isolation of a large area of Campania region, first reached by the network, and the subsequent convergence of the cardiotocographic service in the Operations Center. Despite the organizational difficulties linked to overcrowding, the University Hospital was able to ensure a waiting time of few days for all pregnant women.
The clinical data collection of all monitored patients showed the wide variety of socioeconomic cultural differences between women, which belong to the Operations Center with respect to the Remote Units' ones. In fact, even if pregnant women who live in peripheral areas were younger, they showed lower attention to food control appropriate diet and a lower body weight control both before and during pregnancy and put themselves and their babies at risk for health problems, such as preeclampsia and fetal growth restriction. 15,16 Obesity also puts women at higher risk of diabetes that it generally strikes about 5% of all pregnant women, increasing the chances of congenital abnormalities and pregnancy-related complications. 17
A further problem of these areas is the environmental pollution, because the illegal practices of dumping hazardous waste and setting fire to mismanaged waste have made this territory the so called “land of fires.”
Toxic Waste and Socioeconomic Deprivation
According to several studies, 18,19 our findings showed an increased prevalence of congenital malformations in peripheral areas, especially around landfill sites. In particular, increased rates of sonographic findings for cardiovascular, urogenital, and limb malformations and central nervous system anomalies were detected between the territory of Naples and Caserta provinces, where most of the illegal waste treatment activities are known to take place. Currently, it is not yet known about the real impact of toxic waste on the health of newborns, so it is fundamental to monitor the pregnant women who live in these areas.
The strong reduction of teleconsultation or “second opinion” function has occurred especially in the Municipality of Castel Volturno, where the lack of services, social degradation, and the state of abandonment are greater. Castel Volturno is a special case for the high proportion of foreigners, which constitute 15.3% of the population with 3,854 regular residents according to ISTAT data 2015 and an estimate of about 8,500 irregular, composed of Africans, coming mainly from the sub-Saharan region. 20 The TOCOMAT system was connected to Level I center of Castel Volturno for the years 2008–2012, promoting the process of integration, social inclusion, and first orientation to healthcare services for foreign pregnant women both regular and irregular undocumented, in collaboration with nonprofit organizations (Médecins Sans Frontières and Emergency).
Recently, the international crisis and the exponential phenomenon of migration from North Africa to Europe have greatly increased the number of irregular undocumented foreigners in our country, especially in the southern regions by generating a situation of real “social emergency.”
The concentration of families and pregnant women who live conditions of social disadvantage is high in many peripheral areas of Campania region, where complex processes of impoverishment, vulnerability, and new and old poverty coexist.
Therefore, the existing TOCOMAT project could help to improve the prevention and control of obstetric problems in areas where migration and social deprivation make it hard to monitor the obstetric complications responsible for the highest regional health system costs.
Economic Impact on Healthcare Organization
Previous studies on TOCOMAT system 21,22 had showed an economic advantage maintaining a network composed by Remote Units connected to an Operations Center compared to independent Remote Units. The network has avoided unnecessary transfer of patients to the Operations center for expert evaluation and the overcrowding of emergency rooms only to perform the CTG monitoring. It has decreased the number of unnecessary hospitalizations and the average of hospital stay days for risk pregnancies, reducing the psychological stress for logistical and organizational problems.
Moreover, the algorithm used to select pregnant women to cCTG monitoring has further improved the efficiency of the network allowing the use of computerized analysis in Remote Units located far from the University Hospital and provided with modest resources, with a consequence of economic and management cost saving. According to other investigations, 23,24 a threshold of minimum volume of use of the telemedicine service must be reached to obtain a cost effective service, because with a higher number of consultations, greater savings are made.
Finally, the possibility to perform the computerized analysis of FHR gives reassurance to clinicians and women about the real actual fetal well-being, with positive effects on the quality of care provided. Whenever the midwife or the clinician located in the Remote Units has doubt about the interpretation of the trace, it is sent to the Operations Center for computerized analysis, also in case of physiological pregnancies.
Conclusions
Our experience confirms that telemedicine could enable a gradual decentralization of obstetrical surveillance, allowing equal access to medical expertise irrespective of the geographical location of the person in need. Internet consultation provides a source of fast medical information for second opinion in more developed areas of Campania region and bridges the healthcare gap in situations where no or limited service is available. Therefore, the improvement in quality of care is encouraging in contrast to the progressive decline of the network and to promote the distribution of wireless technologies in peripheral areas.
The development of new information and solidarity networks and the strengthening of the existing ones have a fundamental role in supporting the development of human and social capital in all peripheral areas of a country.
Footnotes
Disclosure Statement
No competing financial interests exist.