
Abstract
Introduction
Fifty percent of patients with chronic illnesses do not take their medications as prescribed, contributing to $290 billion in drug-related problems in the U.S. annually. 1,2 Nonadherence is associated with increased risk of morbidity and mortality. 3,4 National quality improvement organizations demand processes focusing on patient-centered, integrated medication management systems. 5,6 Presently, there is no coordinated system to track medication changes among different systems of care, putting vulnerable patients at risk for adverse drug events. 7,8
Mobile technology is an evolving method for improving patient adherence to medication regimens. Several studies and review articles demonstrate that text messaging can improve adherence to medications for single diseases, including diabetes, human immunodeficiency virus (HIV), and asthma. 9 –14 However, fewer studies assess the impact of smartphone applications for improving medication management. 15,16 While apps are promising, entering medication information manually is cumbersome, and none of the commercially available apps are clinically tested. 17,18 Despite the paucity of evidence-based data on medication adherence apps, studies assessing web-based applications to promote adherence recommend features designed to promote usability among diverse patient populations. 19 –22
We developed a novel medication management app—PresRx optical character recognition (OCR)—by integrating smartphone camera features with OCR technology to auto-populate drug information directly from pictures of patients' medication labels. We beta-tested PresRx OCR to assess the following: (1) accuracy of data entry by OCR, (2) patient acceptance, and (3) patient adherence to chronic medications.
Materials and Methods
Design
Our two-phase feasibility and acceptability study used a single-subject design to evaluate PresRx OCR. After software development and initial testing, selected patients beta-tested the software over a 6-month period in 2014 to identify software issues and inform the first upgrade.
Phase 1. Software Development and Initial Testing
Electronic Medical Office Logistics (EMOL) Health merged their existing medication scheduling system (PresRx) with OCR software to electronically convert medication label text into machine-encoded data fields. The resulting PresRx OCR software captures medication name, dose, route, frequency, and National Drug Code (NDC) information directly from pictures of flat medication labels. Data are transmitted between patients' iPhones and a remote, secure database server rather than maintaining information locally. This method eliminates the risk of data loss if phones are stolen, lost, or damaged. PresRx OCR uses Apple® native controls and incorporates Human Interface Guidelines to achieve maximum population accessibility. EMOL Health refined PresRx by incorporating patient feedback using an iterative development and design approach, thereby informing key design requirements for PresRx OCR, including the following (Fig. 1):
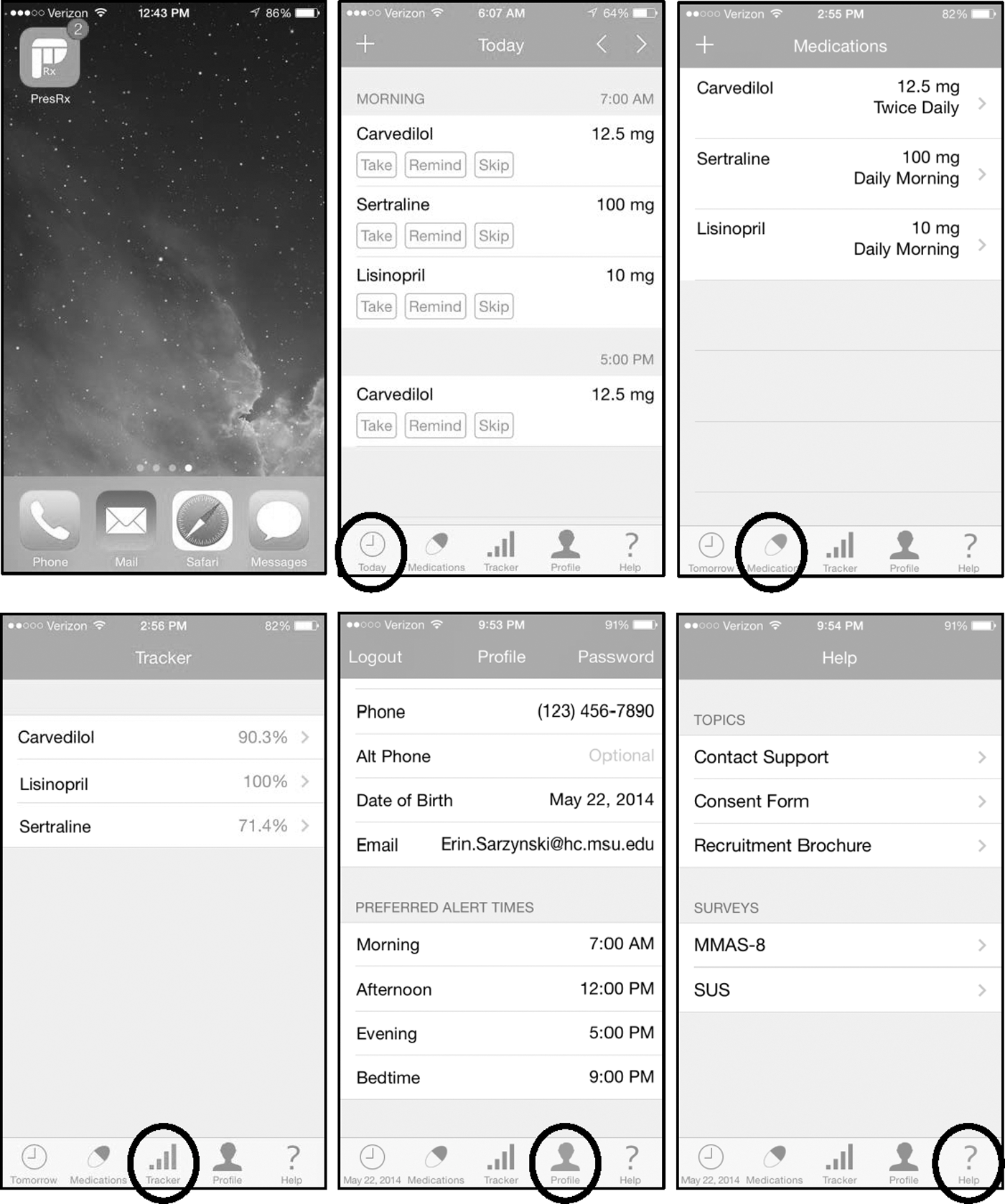
Screen shots of PresRx OCR iPhone application. Circles indicate tab selection, which specifies screen. Top panel left to right: app icon with two pending dosing reminders; daily calendar screen for responding to dosing reminders (patient-centered list); condensed medication list (clinician-centered list). Bottom panel left to right: real-time adherence tracker; patient profile screen (specify preferred dosing times); help screen. MMAS-8, Morisky Medication Adherence Scale; OCR, optical character recognition; SUS, system usability scale.
1. Intuitive layout and navigation.
2. Three data entry options: (i) imaging prescription medication labels, (ii) scanning Universal Product Code (UPC) barcodes for over-the-counter (OTC) medications, or (iii) manual entry.
3. Patient-centered medication list organized by standard dosing periods (morning, noon, evening, and bedtime), endorsed as the Universal Medication Schedule (UMS). 23,24
4. Audio and visual dosing reminders sent as push notifications to patients' lock screens (Supplementary Fig. S1; Supplementary Data are available online at
5. Each medication dose correlated with a unique reminder; patients' responses become a proxy for their medication-taking behavior.
6. Patients respond to dosing reminders by specifying one of the following three options:
A. “take” = patient administered dose
B. “remind” = reschedules dosing reminder in 15-min increments up to 4 h in the future (but not after next scheduled dose)
C. “skip” = patient did not administer dose
• If no response within 24 h, coded as “ignore”
7. Real-time adherence “tracker.”
8. Help screen.
9. Integrated satisfaction surveys to assess usability (System Usability Scale, SUS). 25
10. Integrated NDC database—to ensure accuracy of information auto-populated by OCR.
11. Integrated UPC database—to auto-populate OTC drug information by scanning UPC barcodes.
Initial testing
We previewed the prototype by testing accuracy of auto-populating medication entries by taking pictures of thirty mock medication labels (Fig. 2). We defined accuracy as the percentage of unique data field entries entered correctly (medication name, dose, route, frequency, and NDC) by OCR technology. We also previewed data entry for OTC medications by scanning their UPC codes (Fig. 2).

Novel options for entering drug and dosing information into the PresRx OCR app. In addition to manually entering data, patients can take pictures of medication labels (left) or scan UPC barcodes (right) to automate data entry. UPC, Universal Product Code.
Phase 2. Beta-Test By Single-Subject Design Study
Patients beta-tested PresRx OCR to assess the following outcomes: 1. Accuracy of data entry by OCR 2. Acceptance of the software 3. Adherence to prescription medications for chronic conditions
Study population
Eligible patients were employed by and received primary care services through a large Michigan-based healthcare system (7,500 employees; single pharmacy system).
Inclusion criteria
Age ≥18 years old, taking ≥3 chronic prescription medications, and using an Apple iPhone 4S generation or beyond.
Exclusion criteria
Minor children, incapacitated adults, and those unwilling to transfer prescriptions to the participating pharmacy.
Recruitment
All health system employees received a recruitment e-mail. Respondents met with our study coordinator who screened for inclusion/exclusion criteria, obtained informed consent, and scheduled an index appointment.
Index appointment
Physician-researchers conducted appointments as follows: 1. Review study, answer questions, confirm consent 2. Perform a Best Possible Medication History
26
3. e-Prescribe medications to participating pharmacy 4. Download PresRx OCR application 5. Demonstrate app use 6. Administer adherence survey (Morisky Medication Adherence Scale [MMAS-8])
27
7. Obtain duplicate (flat) medication labels from participating pharmacy 8. Photograph medication labels for OCR-automated data entry 9. Scan UPC barcodes of OTC medications 10. Confirm accuracy of medication regimen auto-populated by PresRx OCR, including UMS dosing periods, and reconcile discrepancies 11. Assess patient proficiency using PresRx OCR by observing patient's independent performance of #8–10 (“teach back”) 12. Advise patients to complete integrated satisfaction surveys
Patients began the 6-month beta-testing period after completing their index appointment (May–June 2014) and received a $25 iTunes gift card for participating. Researchers tracked patient responses to dosing reminders through December 31, 2014.
Measures
Patient characteristics
Baseline demographic and healthcare variables (e.g., comorbidities and chronic medications) were assessed by chart abstraction. We defined chronic medications as prescription medication(s) for conditions present ≥3 months. The complexity of patients' medication regimens was quantified using the Medication Regimen Complexity Index (MRCI), which assigns weights to dosage forms, frequencies, and additional instructions. 28 The MRCI is a validated tool with a minimum score of 1.5 (representing a single tablet taken once daily as needed); there is no established maximum because scores increase with additional medications.
Accuracy of auto-populated medication dosing information
We assessed accuracy of auto-populated medication information, defined as the percentage of unique data field entries entered correctly by OCR technology.
Patient acceptance
We assessed patient acceptance of PresRx OCR using the SUS 25 and semistructured exit interviews. The SUS includes 10 statements rated on a five-item Likert scale (Supplementary Fig. S2). Scores range from 10 to 100, with scores ≥70 indicating acceptable user interfaces. The SUS is highly reliable (α = 0.91) and useful over a wide range of interface types. 29 PresRx OCR prompted patients to complete SUS surveys every 2 weeks. We conducted exit interviews among patients who completed ≥6 months to identify ideas for improvement.
Adherence
We compared adherence rates 6 months before app use (pretest) and 6 months during app use (post-test). We calculated adherence to medication regimens using objective and subjective measures to balance their respective strengths and weaknesses, 30,31 and to triangulate results with PresRx OCR-measured adherence rates.
Objective adherence measure
We used pharmacy fill histories to calculate the proportion of days covered (PDC) over the two 6-month time periods. The PDC assesses how many days in a specified time period patients had access to their medications. 32
Subjective adherence measures
We assessed patient-reported adherence by two methods: (1) pre- and post-app validated adherence surveys: MMAS-8 (α = 0.83) 27 and (2) patient responses to PresRx OCR-generated dosing reminders. We calculated app adherence by dividing the number of doses taken by the number of scheduled dosing reminders, as reported by patient attestations and compiled by the software (i.e., #taken/#reminders).
Data Transmission
Pictures of medication labels were transmitted through a secure application programming interface (API) to the remote database. Our API includes a secure messaging protocol with image compression and metadata (send) and structured data response (receive). We deployed a representational state transfer service to communicate between the mobile application and our remote, secure database using secure socket layer communication with the API to ensure data security. A remote, secure SQL server stored updated medication entries as auto-populated by OCR. All research personnel had access to this password-protected database.
Data Analysis
We generated descriptive statistics and graphic displays for all study outcomes to identify patients by salient characteristics of medication adherence over time. We compared patients who used the upgrade with those who did not. We accounted for missing data by listwise deletion and assessed the influence of baseline demographic characteristics using appropriate nonparametric univariate statistical procedures. We conducted all quantitative analyses using SAS 9.3 (SAS Institute, Inc., Cary, NC). Michigan State University and Sparrow Health System Institutional Review Boards approved the protocol.
Results
Phase 1. Software Development and Initial Testing
PresRx OCR is a medication management application with five screen tabs: daily calendar, condensed medication list, adherence tracker, patient profile, and help screen (Fig. 1).
Initial Testing
Medication information was auto-populated frequently and accurately (≥95%) from mock prescription labels using OCR technology.
Phase 2. Beta-Test By Single-Subject Design Study
Twelve patients responded to our recruitment e-mail. We excluded three patients and one patient withdrew due to factors unrelated to study participation (Fig. 3). Overall, eight patients beta-tested PresRx OCR; five used the software for ≥6 months, of which four completed exit interviews (n = 4 completers). Average age was 43 (range 28–54); patients had a range of comorbidities, took an average of 3.4 chronic medications, and used the app for 3–8 months (Table 1).

Flow diagram of recruitment, enrollment, and participation in the PresRx OCR medication management study (beta-test).
Baseline Characteristics of Study Participants
AVG, average; DM, diabetes mellitus; F, female; GERD, gastroesophageal reflux disease; HCTZ, hydrochlorothiazide; HTN, hypertension; IBD, inflammatory bowel disease; M, male; MDD, major depressive disorder; MRCI, Medication Regimen Complexity Index (minimum score 1.5; no maximum score; higher scores indicate more complex medication regimens).
Accuracy of auto-populated medication dosing information
Medication name was auto-populated from 97% of patient labels, while NDC auto-populated only half of the time (Fig. 4). Accuracy of auto-populated medication information was 95%, 98%, and 96% for drug name, dose, and frequency, respectively.

Phase 2–Accuracy of auto-populated medication label information (patient labels). Results indicate whether medication information was auto-populated; shading indicates accuracy of auto-populated fields. NDC, national drug code.
Patient acceptance
Researchers used patient survey responses to identify areas for improvement, which developers incorporated into the September 2014 software upgrade (Table 2). All eight beta-testers experienced random, unintentional logouts resulting from interrupted internet connectivity when their phones negotiated between Wi-Fi and LTE environments. Only three patients (all completers) arranged for researchers to download the software upgrade that resolved this issue. SUS response rate was low despite automated reminders, regardless of whether patients completed the study. Among completers, the average SUS score was 74.3, indicating that PresRx OCR is an acceptable user interface (Table 3). Older patients reported greater satisfaction with PresRx OCR than younger patients. However, patient satisfaction did not correlate with study duration or completion, or whether patients received the software upgrade.
Features Included in PresRx Optical Character Recognition Software Upgrade Based on Patient Feedback from Initial Beta-Testing
NDC, national drug code; OCR, optical character recognition.
Summary of Participants' App Use, Including Reminders, Software Updates, Acceptance, and Adherence Rates During App Use
MMAS-8 scores range 0–8: high = 8, medium = 6–8, low = <6.
PDC is proportion of days covered (patient has access to medications); >80% indicates high adherence.
Ignore indicates one of two behaviors: (1) patient ignored the dosing reminder, or (2) patient was logged out of the system (no push notification for dosing reminder). The software did not track individual logout events, thus we cleaned the raw data by removing all “ignore” responses spanning ≥5 days, presuming patients were logged out of the system for that duration of time.
SUS scores range 0–100; higher scores indicate greater satisfaction; ≥70 is acceptable.
RR is response rate for SUS surveys (app sent automated reminders every 2 weeks).
MMAS-8, Morisky Medication Adherence Scale; PDC, proportion of days covered; RR, response rate; SUS, system usability scale.
Exit interviews: Four patients completed audio-recorded exit interviews. Patients thought the app was easy to use and mitigated forgetfulness. Interviewees reported that the software upgrade improved sync speed and resolved logout issues, but caused some medications to “fall off” their lists. Regardless, all interviewees provided high overall ratings and two asked if they could continue using the application despite completing the study.
Adherence
Pretest: Among completers, average preapp PDC was 92%, indicating highly adherent medication-taking behavior at baseline (Table 3). By contrast, baseline MMAS-8 scores (6.1) indicated medium adherence, demonstrating moderate correlation between PDC (objective) and MMAS-8 (subjective) adherence measures.
Post-test: Similarly, the PDC estimated greater adherence than the MMAS-8, and both measures decreased marginally from pretest to post-test (Table 3).
Adherence based on patients' responses to dosing reminders: Completers received 2,545 dosing reminders and responded “take” to 2,050 (82% adherence). Hence, PresRx OCR-measured adherence rates marginally underestimated adherence rates compared with PDC calculations (85% vs. 82%, respectively), indicating that app-measured adherence correlates well with objective measures. By contrast, PresRx OCR overestimated adherence compared with MMAS-8 assessments and among noncompleters (Table 3). Reported adherence rates were higher during initial app use than midway during the study when patients reported unintentional logouts, which limited data collection before upgrade installation (Fig. 5). Since logout events could not be tracked, we cleaned the raw data by removing “ignore” responses that spanned ≥5 days, presuming patients were logged out of the system for those days. Of the four completers, only one (P5) did not receive the app upgrade to resolve the logout issue. Subject P5 demonstrated continuously declining adherence over time (Fig. 5) despite data cleaning and a high PDC estimate of adherence (90%, Table 3). Conversely, completers who received the software upgrade demonstrated more consistent adherence rates over time.
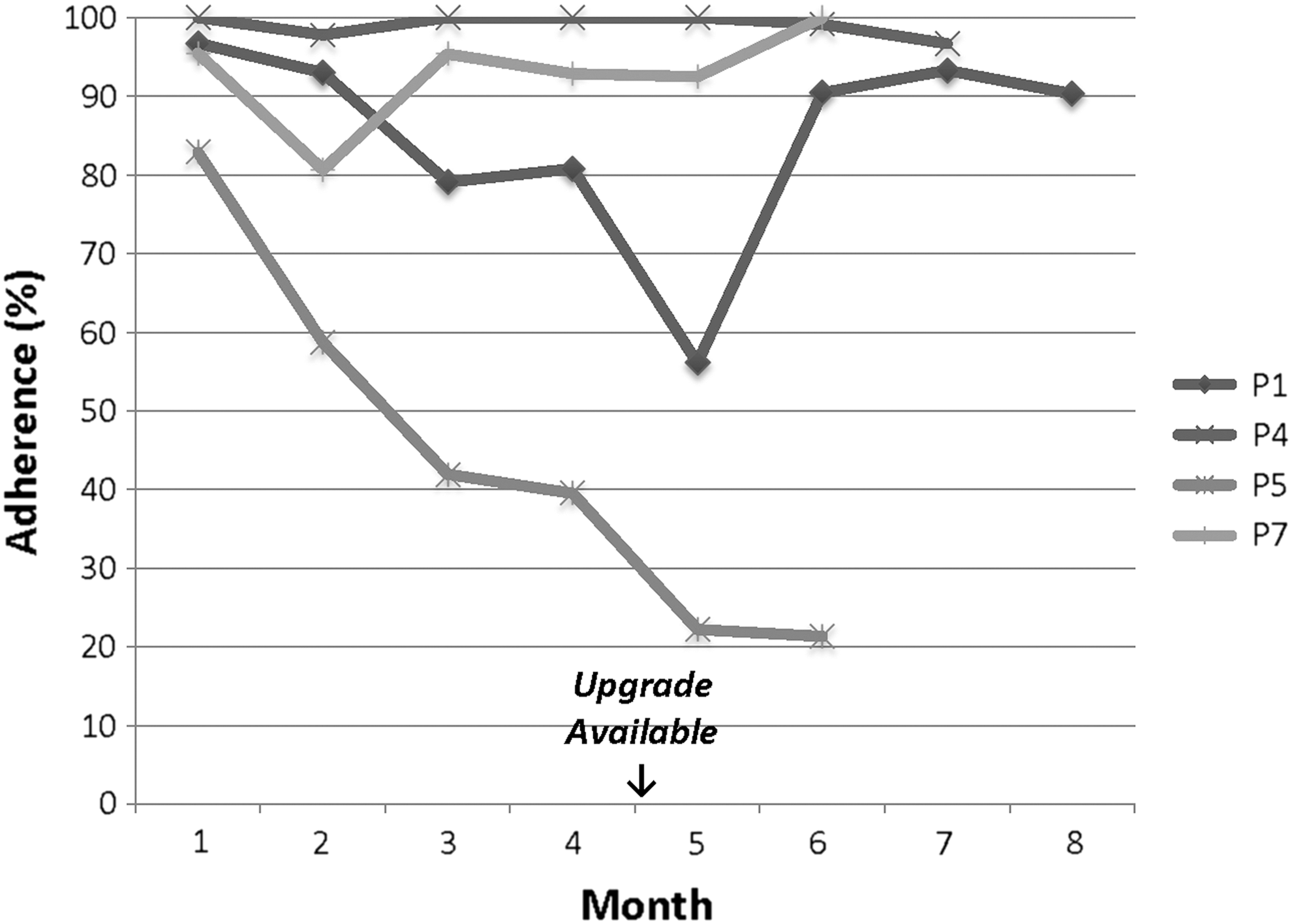
Adherence to chronic medications per patient per month as measured by PresRx OCR.
Discussion
We developed and beta-tested a medication management application—PresRx OCR—using novel methods to auto-populate drug and dosing information: taking pictures of medication labels or scanning UPC barcodes of OTC medications. We also integrated an NDC database to verify the accuracy of auto-populated information. Our study is one of few testing the impact of m-health applications on adherence to multiple chronic medications rather than adherence to single drugs for single diseases. 15,16 Above all, we learned several lessons relevant to medication management apps specifically and interoperability in general.
First, using OCR to convert medication label images into machine-encoded text is important because it is not pharmacy centric. This feature allows for system generalizability when patients use multiple pharmacies or have multiple providers. Alternative solutions may automate data entry through a Substitutable Medical Applications and Reusable Technology (SMART) API, using the Fast Healthcare Interoperability Resources (FHIR) framework. 33 SMART on FHIR is a standard-based open platform that enables plug-and-play interoperability, including app integration with electronic health records (EHRs). Thus, apps developed using SMART on FHIR could leverage an EHR-tethered patient portal to auto-populate medication dosing information. Extending functionality to include adherence prompts aligns with feedback from patients who access their portals to view their medication lists and request prescription refills. 34
Second, patient feedback informed a software upgrade and underscored the importance of iterative, patient-centered design. A study by Mira et al. recruited priority populations in the software design phase to ensure relevant easy-to-use technology. 35 They targeted older adults without prior smartphone experience to refine a medication management app, which improved adherence. 35 Another way to engage older adults is to include reliable drug information (e.g., common side effects), an extension possible by leveraging our integrated NDC database. 21,34
Third, demonstrating m-health success depends on targeting particular patients. While our cohort was appropriate for a feasibility study, we acknowledge limitations due to small sample size, single-site design, and patient selection (e.g., age range, healthcare employees, and iPhone users), which limit generalizability. Moreover, baseline adherence rates were high, limiting our ability to detect improvements in adherence during app use. Clinicians who recommend m-health tools will need to consider various patient characteristics to target groups most likely to experience clinical improvement. For example, patients may benefit if they unintentionally forget their medications and use their smartphones frequently in their daily routines. Future work must also confirm whether app-measured adherence rates are a reliable proxy for patients' actual medication-taking behavior.
Fourth, adherence was high during initial app use, but waned midway through the 6-month study. This “wow factor” phenomenon is characterized by frequent use of new technology that wanes as users lose interest over time. 36 Patients who received the app upgrade demonstrated a boost in adherence immediately following the upgrade, which may reflect reengagement with the software. Thus, our study demonstrates the challenge of continuously engaging patients in healthy behaviors as an adjunct to using technology alone.
Finally, our study highlights concern about data integrity during remote transfer. Applications reliant on internet connectivity can introduce data reconciliation errors when networks are unreliable. Among PresRx OCR users, connectivity issues caused unintentional logouts and slow synchronization speeds. Upon resolving these bugs in our upgrade, we noticed that medications randomly “fell off” patients' lists, which testers mitigated by reentering medication information. We believe that this issue resulted from failed partial synchronization between the remote server database and the application. We could reproduce the error by launching and closing the app in rapid succession, while medications were synchronizing, but only when internet connectivity was poor. Any m-health application that synchronizes data between server databases and personal devices in real time may face similar obstacles. One solution may be apps that work locally, but frequently synchronize to a source with reliable verification of completion and forced retry if unsuccessful.
Additional limitations include our approach to cleaning data for patients who were inadvertently logged out of the system. We arbitrarily chose to remove “ignore” responses spanning more than 5 days, presuming patients were logged out of the system those days, rather than consciously ignoring dosing reminders. We believe this strategy was appropriate for three reasons. First, when study completers were logged out of PresRx OCR, they followed researchers' instructions to log back into the system and resumed responding to dosing alerts. By contrast, three of the four noncompleters abandoned the software after experiencing random logouts. Second, despite cleaning the data, app-measured adherence rates were less than estimates based on PDC calculations, most notably for P5 (the only completer who did not receive the app upgrade, which resolved the logout issue). Third, we attempted to triangulate adherence measures using both subjective and objective measures of adherence. Nevertheless, we acknowledge the limitations of each measure, including concerns about PDC overestimating adherence because it evaluates access to medications, rather than actual medication-taking behavior.
Finally, PresRx OCR auto-populated information from patients' medication labels incorrectly for <5% of data fields, a risk we attempted to mitigate in two ways. First, we programmed PresRx OCR to force manual entry of information that was difficult to parse out using OCR technology. Second, we incorporated an NDC database to confirm accuracy of auto-populated information. Regardless, patients retained the ability to modify any information that was auto-populated incorrectly.
In summary, we developed a medication management application for iPhone users—PresRx OCR—that automates data entry by extracting key drug and dosing information from medication labels using OCR technology. Importantly, app-measured adherence rates correlated well with objective measures. Future studies should target patients most likely to benefit from medication management apps and test among patients prescribed complex medication regimens by multiple providers using different EHR systems. Ideally, these applications will leverage an API approach, such as SMART on FHIR, to consolidate data from multiple locations into a single, patient-centric application.
Footnotes
Acknowledgments
This work was supported by the Michigan State University (MSU)/Sparrow Health System Center for Innovation and Research (Grant No. #130741). We thank professionals at MSU and Sparrow Health System for their time and effort implementing this work. We also thank colleagues at the Institute for Health Policy and the College of Nursing at MSU for reviewing drafts and providing editorial assistance of our article.
Disclosure Statement
No funding source had any role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. Dr. Sarzynski reports income from the Center for Medical Education for her role as a commentator in Continuing Medical Education audio publications. Mr. Decker is President and Chief Executive Officer at EMOL Health. Mr. Thul is employed by EMOL Health. All remaining authors report no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.