
Abstract
Introduction
Caries (tooth decay) is the second most costly diet-related chronic disease in Australia, ahead of coronary artery disease and diabetes mellitus. 1 Rural or remote populations often have poorer oral health than other groups, primarily due to geographical remoteness and the uneven distribution of the dental workforce. 2 Caries is often not a self-limiting disease, but its impact can be prevented or reduced through regular dental screening, access to fluoridated water, and oral health promotion. 3 A shift from a “treatment” to “prevention” is the key to reducing or preventing dental caries among a population. Reaching rural/remote populations to assess their oral health status is challenging, as this necessitates lengthy travel, time, and funding. Although unaided face-to-face screening has remained the gold standard approach to routine oral examination, this method is inappropriate in large epidemiological surveys as it requires substantial economic and human resources. Searching for an inexpensive and valid alternative that can expedite diagnosis of oral diseases among rural populations, while maintaining a good level of diagnostic accuracy, is essential.
One of the potentially viable solutions to address geographical hurdles and the unavailability of dentists, is mobile teledentistry. 4 Mobile teledentistry is a subset of telemedicine that incorporates cellular phone technology and store-and-forward telemedicine into oral care services. Almost all smartphones have a built-in camera and mobile connectivity and are readily accessible at a low cost. These technologies can be combined to create an effective teledentistry screening alternative. Despite dental photography becoming an integral part of daily dental practice, it has rarely been used as means of diagnosis, consultation, or referral in routine practice. Recent evidence indicates that the diagnostic performance of photographic methods in the detection of oral diseases is comparable to the traditional visual approach. 5 –9 A flash-equipped digital single-lens reflex (DSLR) camera can produce high-quality images even in a low illumination setting. However, its relatively high cost, large size weight, and complexity makes it difficult to use. 10 In contrast, camera-equipped smartphones are readily available, affordable, portable, easy to handle, and can produce good-quality images. 10 The power of cellular technology enables their usage in various tasks such as processing, storing, and subsequent sharing of images. Their introduction into other health disciplines, in particular, tele-audiology and teledermatology, has been shown to be beneficial. 11 –14
A number of teledentistry studies have been conducted using DSLR or intraoral cameras to evaluate the accuracy and reliability of photographic methods in oral screening, 5 –9 However, evidence on the use of smartphone cameras in epidemiological dental research is rare. 4,15 As an initial phase, a validation study was completed to establish and test a robust store-and-forward teledentistry system and smartphone app for use in remote dental screening. 16 In view of the limitations of a face-to-face screening approach and toward finding a valid and inexpensive screening solution, the purpose of this study was to evaluate the efficacy of a mobile teledentistry approach in remote screening for dental caries.
Materials and Methods
Study Sample
Adults or parents/guardians of children visiting the dental clinic were invited to participate in dental screening, including obtaining photographs from their mouth. Information sheets and consent forms were provided to participants. This trial is an observational cross-sectional study carried out in a dental clinic in 2014, where a sample of one hundred (n = 100) participants was recruited. The inclusion criteria for the participation were patients of any age, attending a routine checkup, and providing informed consent. All captured photographs were anonymous and only showed the participant's dentition. The research was completed under ethics approval from the Human Research Ethics Committee, the University of Western Australia (Ref No.: RA/4/1/6647).
Architecture of the Mobile Teledentistry System
A store-and-forward telemedicine server, “Remote-i,” was developed to facilitate the storage, retrieval, and management of the database. 16,17 The Remote-i allows the transmission and storage of photographs online, from either a smartphone or computer through the Internet. Users can access the database from any mobile/desktop Web browser using individual user IDs and passwords. An image acquisition Android app was also created to operate the existing default camera on a Motorola® MotoG smartphone. The new Android app enabled patient information to be entered, dental photographs to be captured, and then allowed subsequent transmission of these records to the server, using Wi-Fi or mobile data networks. 16
Screening (Visual and Photographic) Procedures
Using the screening protocol used in our previous trial, 4,16 the unaided face-to-face oral screenings (without radiography) of all the participants were carried out by a registered dentist to screen for caries visually. This assessment was used as the benchmark standard. The face-to-face assessment scores were recorded on an oral screening form that followed the guidelines for oral health surveys developed by the World Health Organization (WHO), 18 a treatment plan or referral was provided when necessary. In a separate subsequent visit, a trained teledental assistant (dental student or dental assistant) took photographs of each participant's mouth using a smartphone camera (Fig. 1). The teledental assistants were provided with a photography protocol and received hands-on training on how to capture good images. They also had the opportunity to practice using a smartphone camera on volunteers. Only the room lighting and built-in flash of the smartphone camera were used during the photography. Neither cheek retractors nor intraoral mirrors were used for the dental photography. A minimum of five dental images per patient were taken, front, right lateral, left lateral, upper occlusal, and lower occlusal views (Fig. 2). Following the completion of photography and creating a record on the Android app, each participant's set of data was then directly transmitted from the Android app to the Remote-i server through the Internet, for later evaluation by an off-site dentist (charter).

Illustration showing the relationship between a smartphone camera and the mouth during the dental photography.
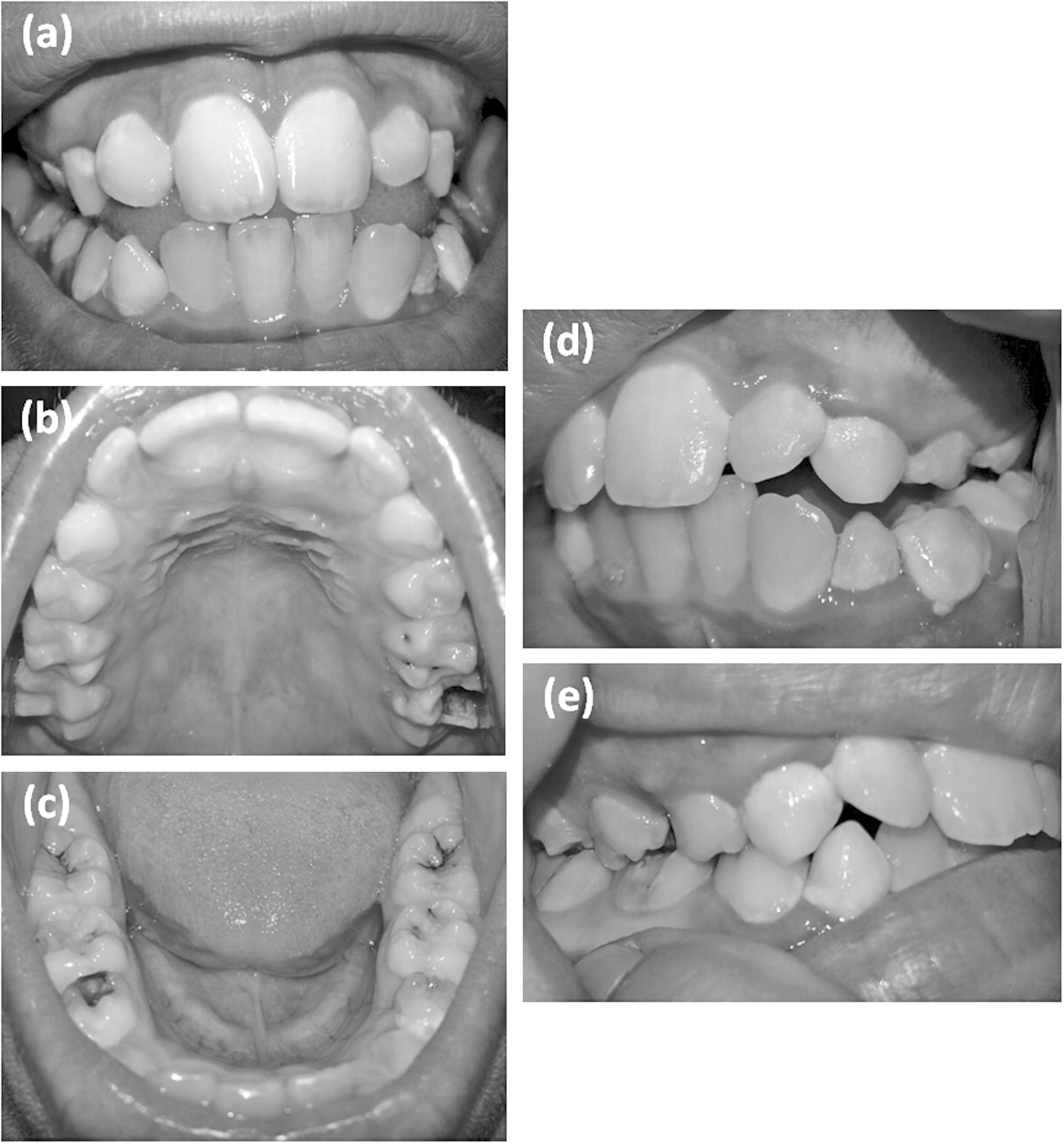
Examples of smartphone camera shots showing five dental views.
Outcome Assessment
The charting of the photographs was conducted independently by two dentists (charters) using a separate image-viewing app built upon the Remote-i system. Dental photographs were charted without any knowledge of the results of the benchmark standard. Both charters received instructions about how to use the database, review photographs, insert findings, and submit their reports into the system. Charters accessed the database using user IDs and passwords. After selecting a record, each charter reviewed images and commented on the dentition status for each tooth on a predefined assessment chart. The external reviewers (screeners/charter) also had access to other personal information about the participants such as date of birth, gender, and postcode, as well as Indigenous status. These independent assessments by charters formulated the database, which was compared to the benchmark face-to-face caries assessments. Caries assessment was completed at tooth level based on a protocol developed by the WHO. 18 This protocol has the advantage that it has been designed to be simple and easy to use in large-scale oral health surveys. At the screening level, the use of the International Caries Detection and Assessment System (ICDAS) method was not possible because intraoral photographs only provide a two-dimensional view, which makes it difficult to carry out the analysis based on the tooth surface.
Statistical Analysis
Weighted kappa (K) statistic was used to estimate the intergrader reliability of the photographic and face-to-face caries assessment methods. 19 To estimate the intragrader agreement, 15% of the records were recharted again, at least 4 weeks after the initial charting of the dental photographs. The sensitivity, specificity, accuracy, positive-predictive value, and negative-predictive value of the photographic method for each charter were calculated. Because photographs only provide a two-dimensional view, it is difficult to inspect all surfaces of the teeth, particularly the interproximal surfaces of posterior teeth. Therefore, the assessment of caries was based on the entire tooth rather than tooth surface, with the teeth scored as either having caries or being sound. Interproximal or root caries were excluded, due the difficulty of detecting these carious lesions in photographs. Filled and missing teeth were also excluded from the analysis. The sample size calculation was based on a two-sided 95% CI (confidence interval) for a single proportion using the Z-test approximation, an effect size of 0.1 and an expected observed proportion of 0.90. The number of participants with caries that met a power of 0.8 was estimated to be 35 [n ≥ (Z2/m2) × p (1 − p)]. 20 With the prevalence of caries at 35% (1.86 × 35 = 65), 65 participants without caries are needed. So a sample of 100 participants was recruited.
Results
The demographic characteristics of the sample are presented in Table 1. Approximately, 500 dental photographs (5 photographs per subject) were obtained from the participants using the smartphone's camera. Of 3,200 teeth scored, the percentage of unrated (not amenable to be scored) teeth was 8% (266 teeth) for charter 1 and 19% (596 teeth) for charter 2. Sensitivity and specificity values for the photographic method compared to the benchmark face-to-face caries assessment ranged from 60% to 63% and from 96% to 99%, respectively. The sensitivity value for the photographic caries assessment (charter 1 vs. charter 2) was 85%. Weighted kappa as a measure of intragrader agreement for the photographic assessments was almost perfect (K = 0.84). The intergrader agreement between the two methods of screening (photographic vs. face-to-face) ranged from moderate to substantial (K = 0.54–0.66). The level of intergrader agreement between charter 1 and charter 2 was substantial (K = 0.68). The diagnostic accuracy measures and level of agreements for both photographic and face-to-face screening methods are presented in Table 2.
Demographic Characteristics of the Sample
Accuracy and Reliability Measures
Benchmark screening: face-to-face oral screening; Charter: photographic caries assessment.
CI, confidence interval; NPV, negative-predictive value; PPV, positive-predictive value.
Discussion
This study shows that the combination of store-and-forward telemedicine and inexpensive smartphone camera use, offers a valid and reliable means of remote screening for dental caries. Despite the scarcity of research evidence on the use of a smartphone camera in dental screening, the present findings strengthened our previous reports that the mobile teledentistry approach has the potential to detect caries from a photograph taken by a smartphone camera with an acceptable “moderate” diagnostic validity and reliability. 4,16 It is acknowledged that neither the photographic method nor a standard face-to-face screening approach can detect interproximal or precavitated carious lesions without radiography examination and the failure to use radiography could result in underestimation of caries occurrence. Therefore, at the screening level, the focus of this study was on the evaluation of efficacy of a mobile teledentistry approach for dental screening, not for the clinical estimation of caries prevalence.
Our findings showed a moderate level of concordance between the two screening approaches (photographic vs. face-to-face) and the two dentist charters. It is well-known that different dentists can reach different diagnostic outcomes. 21 The moderate level of concordance (K = 0.68) between the two charters was most likely due to the difference in clinical experience and training. Although both charters had a lower level of intergrader agreement relative to the benchmark face-to-face screening, the intragrader agreement for the photographic assessment was quite high, suggesting that the charters were uniform in the charting and the way they detected caries from the photographs.
Despite “unaided” face-to-face oral examination being the primary method used to assess oral health status, previous research has shown that this technique is not accurate, with a sensitivity of less than 50%. 22,23 Our results indicate that photographic caries assessment maintained a relatively moderate level of sensitivity and a very high specificity, comparable to that of face-to-face caries assessment. The specificity values were higher than sensitivity values across the two charters and the two screening approaches. The higher value for the specificity could be attributed to the inability of the charters to see some carious lesions on a photograph compared to the benchmark face-to-face assessment. The sensitivity of the photographic method (charter 1 vs. charter 2) met the WHO's reference standard of 0.85–0.90. 18 In contrast, the sensitivity scores for the photographic method (60–63%) compared to the benchmark face-to-face assessment were lower than the WHO's reference standard. The lower value of the sensitivity is likely to be because filled and missing teeth were not included in the analysis. Missing teeth and restorations/fillings are more likely to be detected on a photograph. 16 Charter 1 had a slightly higher level of concordance and sensitivity relative to charter 2. This is probably explained by the potential of charter 1 to identify carious lesions on the photographs more than the other charter or when uncertain by rating a tooth with suspected lesion as having caries.
Our previous research, 24 demonstrated that some photographs taken by smartphone were of low quality; we attributed this to a failure to comply with the photography protocol or due to the presence of saliva, blood, or debris. For the purpose of facilitating the charting process, both charters were asked to score any tooth not amenable to be scored as “unrated.” The difficulty in detecting carious lesions on the photographs and distinguishing them from artifacts could justify why charters scored some teeth as “unrated.” Such drawbacks could contribute to the suboptimal sensitivity and specificity. This is consistent with previous research that reported variations in the inter-rater reliability in caries detection, mainly in the posterior teeth, attributed to fissure morphology or staining. 25,26 It is well known that assessment of caries from photographs has a shortcoming in that a photograph can only provide a two-dimensional view, which prevents observing all tooth surfaces, particularly the interproximal surfaces of posterior teeth (molars). 4,24 The photographic method is also known to have limitations for the detection of caries on root surfaces (unless they are exposed through gingival recession) or nonvisible secondary caries. The two-dimensional view allows detection of carious lesions mostly on the occlusal surfaces, buccal and lingual surfaces, of the teeth. The teledentistry approach to dental screening (incomplete oral examination), used within the framework of its limitation, offers a reliable means of remote dental screening. This method can be most effective when a shortened arch with a reduced number of surfaces of limited visibility is present, such as in children.
From a practical point of view, it seems reasonable to take advantage of the advances in information and communication technology and increasingly widespread global connectivity to utilize potential cost-saving solutions such as smartphone use to make oral care services more accessible. Until recently, the use of the smartphone in telemedicine was not well received because of the low quality of the built-in cameras, limited storage space, and unsuccessful data transmission. 10 With many people now possessing smartphones, their use in routine dental services is projected to increase due to their inherent digital imaging capabilities, computational power, and sharing ability as well as access to low-cost, secure cloud storage.
Due to the shortage of dentists practicing in rural communities, residents in these regions may seek dental care from general medical practitioners (GPs) or emergency departments. This can result in underreferral or unselective referral of patients who need a specialist consultation, increasing the burden on rural populations through additional travel and increased waiting times. The mobile teledentistry approach to dental screen holds great promise for rural or remote communities where dental care services are limited. At the screening level, GPs, nurses, or even nonlicenced health professionals such as teachers or caregivers can obtain digital data (dental photos) for later evaluation by a dentist at a distance. 27,28 A dental expert accessing the database from the desktop can assess the records and determine whether cases need a referral or can be delayed. This approach provides a way to identify those for whom referral is unnecessary or prioritizing those requiring an urgent assessment by a dental specialist. This has the potential to reduce inappropriate referrals and prioritize patient assessments, thus avoiding unnecessary travel and reducing waiting times. 29 –31
Conclusion
Despite some limitations, this study suggests that the mobile teledentistry approach has the potential to detect occlusal caries from photographs taken by a smartphone camera with an acceptable diagnostic level. To improve the oral health of a population, ongoing monitoring of oral health status, using valid and inexpensive screening tools, is necessary. In light of the limitations of the face-to-face dental screening approach in large epidemiological studies, it is possible that a mobile teledentistry approach can offer a potential cost-saving alternative to address the problems of care access and the rising costs of dental care. Further well-designed research is required to address the existing limitations and improve the diagnostic performance of the teledentistry approach.
Footnotes
Acknowledgments
The authors received no financial support for this work. We would like to acknowledge the kind assistance of Dr. Christopher Pantin, Mrs. Debbie Williams, and Ms. Jennine Bywaters from Absolute Dental for their efforts in data collection. We also acknowledge the assistance of Dr. Jacques Filez from the University of Western Australia for his contribution in this trial. We would like to thank Di Xiao and Janardhan Vignarajan from CSIRO Australia for their technical support. Thanks also to dental students (Andrew Liaw, Olivia Haselton, and Abhayjit Dhillon) at the dental school, James Cook University, for their efforts in data collection.
Authors' Contributions
M.E., the main author contributed to conception, design, data acquisition, analysis, and interpretation, drafted, and critically revised the article; M.T., S.B. and E.K., contributed to design, data analysis, and critically revised the article; Y.K., contributed to development of the telemedicine system and critically revised the article; B.H., contributed to data acquisition and critically revised the article; J.S., contributed to data acquisition and critically revised the article. All authors gave final approval and agree to be accountable for all aspects of the work.
Disclosure Statement
No competing financial interests exist.