
Abstract
Introduction
Oral cancer is the sixth most common cancer worldwide 1 with a global average age-standardized incidence rate (ASR) of 3.9 per 100,000 population and age adjusted death rate of 1.9 per 100,000 population. 2 The majority of oral cancer cases are diagnosed in the developing regions of the world where the ASR can go as high as 20 per 100,000 for example, in India. 3 Globocan estimates that in the less developed countries, more than 110,000 deaths were attributed to oral cancer in 2012 and this is expected to increase by 50% to reach 160,000 in 2025. 4 This is perhaps not surprising as oral cancer is typically associated with late presentation where more than two-thirds present at late stages, 5 which consequently result in poor survival. 6 While the late presentation of oral cancer is perhaps not different from other cancers diagnosed in developing countries, oral cancer affords a unique potential for early detection through direct examination of the oral cavity. 7 –9
Oral cancer is often preceded by visible lesions termed as oral potentially malignant disorders (OPMD), 10 which can be detected during routine screening by clinical oral examination (COE). Oral cancer screening is an evaluation process by dental practitioners on a target community to determine whether these individuals have OPMD or oral squamous cell carcinoma. 11 A high prevalence of OPMD has been reported in South and South East Asia 12,13 and in Malaysia, the prevalence of OPMD and oral cancer have been reported to be 0.01–9.6% 14 –18 and 0.04% 16 respectively. A previous study in India have shown that oral screening resulted in early diagnosis, down-staging of the disease, and prevention of oral cancer-related deaths. 19,20 While early detection has shown effectiveness in reducing the burden of oral cancer, cost effective and efficient methods are critical in determining the successful implementation of early detection programs particularly in low resource setting where the ratio of dental specialist to the community is low.
The major challenges in early detection of oral cancer lie in detection, patient referral, diagnosis, and treatment, 21 and this hinges on the clinical pathway and seamless communication between primary and secondary healthcare professionals. One way to communicate quickly and effectively between these two professionals is through telecommunication, which is also known as teledentistry. Teledentistry can be defined as the use of information technology for communication, to exchange information on dental records, digital imaging, and health-related information using mobile devices. 22 Teledentistry has been used to facilitate screening, diagnosis, consultation, treatment planning, and more importantly to maintain continuity of care in a cost-effective manner. This could be particularly useful in reaching under-served populations. 23 –25
Mobile phones are widely used in communities in developing countries where its usage in a country such as Malaysia is reportedly at 144%. 26 Further, emerging evidence demonstrates that smartphone usage is increasingly being embraced by healthcare professionals, for example in United States the figures increased from 64% in 2009 to 81% in 2012. 27 However, the use of mobile phone applications (Apps) as a method of virtual consultation between dentists and oral medicine specialists (OMS) is limited 28 –31 and application of such technology to identify and screen high-risk community for systematic documentation and referral of patients remains limited. 32 Given the high usage of mobile phones and the advancements in imaging technology within these gadgets, this affords a unique opportunity to develop programs to utilize teledentistry in the early detection and referral in the context of oral cancer. One critical component in utilizing mobile phone imaging in the early detection and referral of patients with suspicious oral lesions, is the accuracy where concordance between evaluating a lesion through an image captured by the mobile phone and that through COE should be high to avoid false negative or false positive that could affect management decisions. In this study, we examined the feasibility of using mobile phone imaging in a low resource setting to determine whether it can be integrated into standard workflow of patient management, and we measured the concordance in clinical diagnosis between COE and images taken with the mobile phone.
Materials and Methods
Setting and Patient Selection
Ethical approval for this study was obtained from the Medical Ethics Committee, Faculty of Dentistry, University of Malaya [DF CO1606/0055(L)]. Sixteen patients were included in this study; eight patients who have target lesions (leukoplakia, lichen planus, and oral submucous fibrosis) and eight patients who have normal oral mucosa and/or variants from normal (leukoedema, linea alba, palatal torus, fordyce granules, or nonreferable oral mucosal changes (frictional keratosis) were selected by two independent OMS (A.R. and R.B.Z.) for this study. Before clinical examination, patients were informed of the objectives of this study and written informed consent was obtained from these individuals to allow dentists to take pictures of their mouth. The flow chart of the study is depicted in Figure 1.
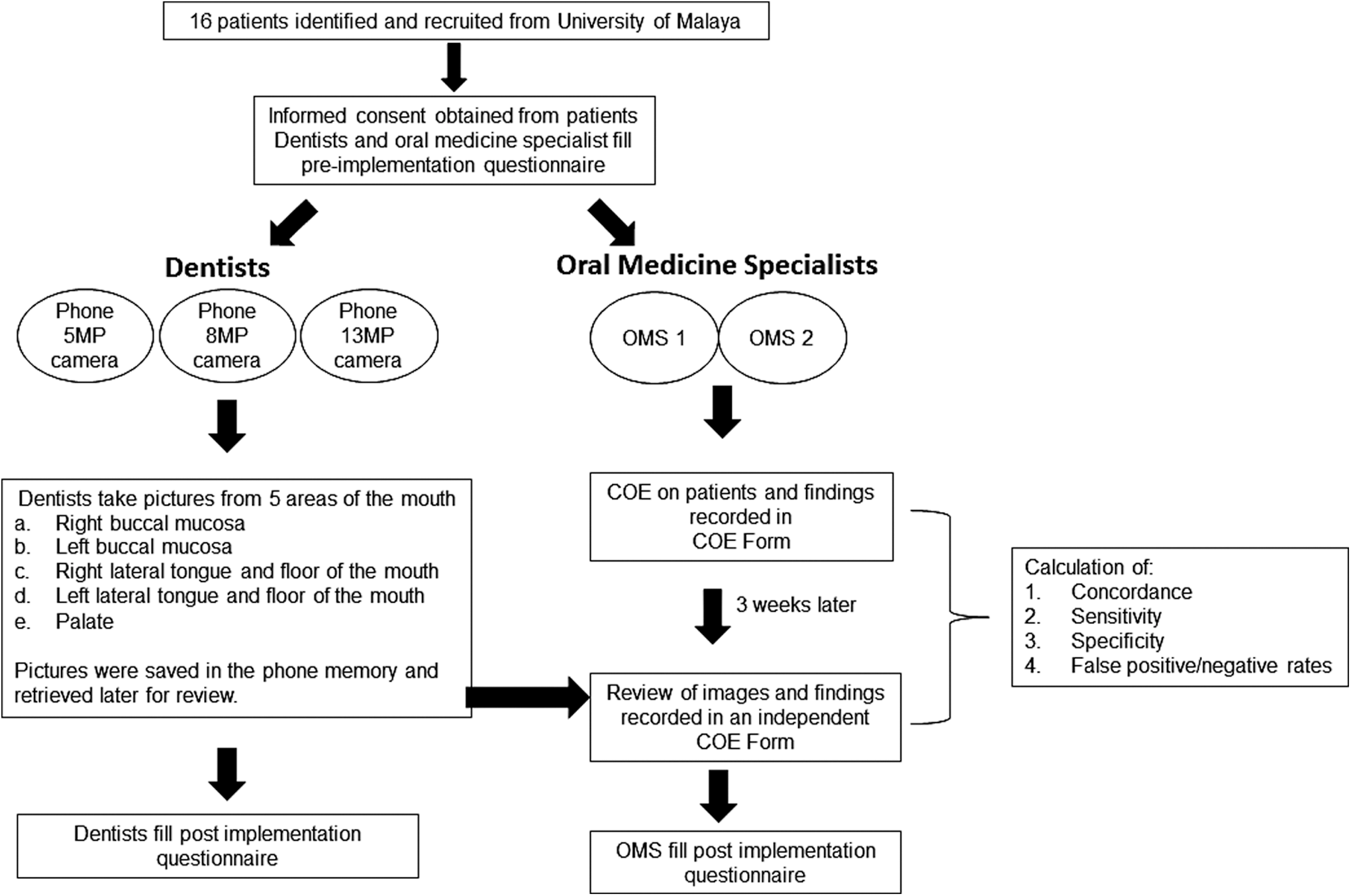
Study workflow. COE, clinical oral examination; OMS, oral medicine specialists.
Training
Three dentists and two OMS were trained to use the mobile phone camera an hour before seeing the patients. During the training, the dentists were instructed to capture five images from distinct sites of the oral cavity including (1) right buccal mucosa, (2) left buccal mucosa, (3) right lateral tongue and right floor of the mouth, (4) left lateral tongue and left floor of the mouth, and (5) palate.
Equipment and Procedure
Three mobile phones with different resolutions were used for this study and their specifications are detailed in Table 1. Images were acquired with an additional light source from the dental chair. The mobile phones were wiped down with wet wipes before use to ensure that the mobile screen is clear, and for infection control and the dentists wore powder-free gloves during the procedure. The images taken with the phone camera were stored in the phone storage and retrieved after the study.
Specification of the Mobile Phones Used
Coe and Teledentistry
The most important aspect of using the mobile phone in clinical practice or any other form of teledentistry is to minimize false negative or false positive reporting and an important indication to refer a patient to the OMS is to identify whether the lesion is an OPMD or not. We evaluated whether this could be accurately determined through the images, by measuring the concordance between COE and teledentistry. While it is important for the OMS to clinically diagnose lesions, the most important decision still remains whether the decision to refer is as accurate as if one were to conduct a COE. Therefore, the concordance in the referral decision made by OMS when doing COE compared to when reviewing images was also measured.
In this study, COE was conducted by two OMS and they needed to (a) note the presence of a lesion, (b) categorize the lesion as OPMD, non-OPMD, or normal variant, (c) diagnose the lesion, and (d) to state whether the lesion should be referred. Both the OMS were blinded to one another's findings.
After 3 weeks of wash out period, the OMS were asked to review the images taken by the three dentists. The OMS reviewed the images on a Sony VIAO computer (model PCG-6XGP) with a 13.1″ HD LCD screen. The average sizes of the images were 700 kb (range from 40 kb to 2,670 kb, depending on the resolution setting in each mobile phone that was used to capture the images).
Questionnaire
To examine the feasibility of using mobile phone imaging in low resource setting, two questionnaires were used before and after the study. The preimplementation questionnaires consisted of 10 questions constructed to obtain (a) general demographic of users, (b) users' expectation of using mobile phone as an adjunctive tool for early detection of oral cancer in the community, and (c) the factors that could motivate them to use a phone camera as an adjunctive tool. The postimplementation questionnaires consisted of 20 questions for OMS and 23 questions for dentists that were meant to determine (a) feasibility and satisfaction of the dentists and OMS on the use of a mobile phone to take pictures of the oral cavity (for dentists) or to make a diagnosis (for OMS), (b) factors that could motivate them to continue using mobile phone beyond the pilot study, (c) feasibility of implementing its use in their patient management workflow, and (d) quality of the images taken using mobile phone in this programme. Both questionnaires have been validated by independent dentists and OMS.
Statistical Analysis
Data were analyzed using SPSS 20.0 for Windows software (SPSS, Inc., Chicago, IL). Diagnoses made by both OMS were tabulated by descriptive statistic and concordance findings on diagnosis between COE and teledentistry were calculated using Cohen's Kappa coefficient ( ). Sensitivity and specificity of teledentistry were also calculated using COE as the gold standard.
). Sensitivity and specificity of teledentistry were also calculated using COE as the gold standard.
Results
Coe and Teledentistry
The concordance between COE and teledentistry are tabulated in Tables 2 –4.
Concordance in Detecting Presence of Lesion from Clinical Oral Examination and Diagnosis from Review of Images
COE, clinical oral examination; OMS, oral medicine specialists.
Concordance in Recognizing Category of Lesion from Clinical Oral Examination and Diagnosis from Review of Images
Concordance in Referral Decision from Clinical Oral Examination and Diagnosis from Review of Images
Presence of lesion
In the first instance, the OMS had to determine the presence or absence of a lesion in each of the patients. The concordance between COE and teledentistry in determining the presence of a lesion are tabulated in Table 2. Taken together, the Kappa values for OMS 1 and OMS 2 were 0.625–0.750 and 0.500–0.875 respectively. These values indicate that the concordance between diagnosis through COE and reviewing images were moderate to strong. The lowest Kappa values for both the OMS were those with images taken using camera A, which has the lowest resolution. The overall sensitivity and specificity in identifying the presence of lesions through teledentistry were 71% and 100% respectively with a false negative rate of 0.13 (Table 5). These values improved with the resolution of the phone camera where sensitivity and specificity of 81.3% and 100% can be achieved with phone C (Table 6) where the camera resolution was 1080 × 1920 pixels.
Overall Sensitivity, Specificity, False Negative and False Positive in Detecting Presence of Lesion, Recognizing Category of Lesion, and Referral Decision
Sensitivity, Specificity, False Negative and False Positive Rates in Detecting Presence of Lesion, Recognizing Category of Lesion, and Referral Decision Based on Individual Mobile Phones
Category of lesion
Here, we classified the category of lesions into OPMD lesion, non-OPMD lesion, and normal (normal variant and no lesion). From Table 3, the Kappa values for OMS 1 and OMS 2 were 0.639– 0.761, and 0.515– 0.881 respectively. These values signify that the concordance between COE and reviewing images was moderate to strong in determining whether a lesion is an OPMD. The overall sensitivity and specificity to correctly identify OPMD were 75% and 100% respectively with a false negative rate of 0.24 (Table 5). Again, with phone C, a sensitivity of 87% was achieved compared to 80% and 56% for phone B and A respectively where the camera resolutions were lower (Table 6). Further, false negative rate can also be reduced with a higher resolution camera where the false negative rate reduced markedly to 0.13 when phone C was used (Table 6).
Referral decision
While it is important for the OMS to clinically diagnose the lesions, the most important decision still remains whether the decision to refer a patient is as accurate as if one were to conduct a COE. From Table 4, the Kappa values for OMS 1 and OMS 2 were 0.738–0.871 and 0.600–1.000 respectively. The concordance in referral decision made either through COE or reviewing images were moderate to almost perfect. Similar findings were also found in this section where the lowest Kappa values for both OMS were seen in images taken using camera A, which has the lowest resolution among the three cameras. This indicates that using the images, individuals who needs to be referred to OMS can be accurately identified for further management. Consistently, the sensitivity and specificity in making the correct referral decision were 81% and 100% respectively, with a false negative rate of 0.19 (Table 6). Notably, when phone B and C were used, the sensitivity and false negative rates were 86–93% and 0.07–0.14 respectively (Table 6). Taken together, reviewing images taken using the mobile phone enables the correct referral decision with high sensitivity and specificity, and low false negative rates.
Integration into Standard Clinical Workflow
In this feasibility study, three dentists and two OMS answered questionnaires before and after the study. All dentists agreed that using a mobile phone as an adjunctive tool has the potential to improve early detection of oral mucosal lesion and is easy to be used in the community setting. In addition, all dentists would like to continue using the mobile phone beyond the study as they were motivated by the belief that the mobile phone was user friendly, and could assist in detection of oral mucosal lesions by providing a direct link between dentists and OMS, that would enable dentists to ask for opinion if they see any suspicious lesion. These findings were consistent between the pre- and postquestionnaires. While they reported that it took about 10 min to capture the five images, they found that all patients were cooperative when the pictures were taken. Even though 2/3 of the dentists thought that using the mobile phone would cause longer waiting time compared to COE, this process allowed the dentists to document changes within the oral cavity that could be referred to when the patient is followed up at a later date. These findings from the questionnaires are summarized in Table 7.
Dentists' Satisfaction on Using Mobile Phone as an Adjunctive Tool for Early Detection of Oral Cancer
Reviewing of images through the computer by the OMS took less than 5 min per case and generally, both OMS were satisfied with the images captured with the mobile phone camera, and think that this has the potential to improve early detection of oral cancer. However, images taken using phone A was deemed to be poor compared to phones B and C. In addition, it was suggested that a picture of the lesion (if one was present) should be taken first before proceeding to document the rest of the oral cavity systematically. Further, the OMS also stressed that adequate training of the dentists is needed to ensure that the images taken are of high quality.
Discussion
In this feasibility study, we measured the concordance between diagnoses based on COE and teledentistry and determined whether the use of mobile phone imaging can be integrated into standard workflow of patient management. Consistent with other studies on teledentistry, 24,33 we observed moderate to strong concordance between COE and reviewing the images taken with the mobile phone in terms of recognizing the presence of lesion, the category of the identified lesions and referral decision. These findings show that there is potential to use this work flow in low resource setting especially if we can train healthcare worker or health aide properly to take images of the designated sites. Further, this workflow can also help to assist screening in the community and follow-up of patients. While we found moderate to high concordance rates between COE and teledentistry, we found that an important factor in determining the use of mobile phone cameras in the clinical setting was the resolution of camera where higher the resolution, the higher the concordance rates and the lower the false negative rates.
While infection control is an important factor to consider when using the phone as an adjunctive tool in the clinic, we did not include any covering on the phone as there is no direct contact between the patient and the phone. Furthermore, a cover on the phone may compromise the quality of the images. In this study, the dentists wore powder-free gloves while examining the patients and using the phone to take images. Even in situations where powdered gloves are used, it is unlikely that the powder on the gloves will affect long-term usage of the phone as phones these days are installed with screen protectors.
As the main target of cancer screening is to identify oral cancer at an early stage to prevent death from invasive cancer 34 the teledentistry approach complies with the main principle of screening, and indeed the use of the mobile phone as a tool for oral cancer surveillance in the community is emerging. 32 The workflow introduced in this study can help to reduce the possibility of missing a high-risk lesion or over diagnosis as it allows communication between the dentists and the OMS before referral. 34 Consistent with this, the OMS in this study agreed that the usage of mobile phone has the potential to improve early detection of oral cancer when clear images of the target lesion are captured. From this study, several areas for improvement were highlighted including the need for information on patient history and good quality images that are not unique to this study, and have been discussed previously by others. 32,35,36 These challenges can be addressed and overcome by adequate training and practice on the use of the mobile phone camera. In addition, the camera specification could also play a vital role in ensuring that the images are of high quality. Here, we found that images taken using camera with 8- or 13-MP were rated by the OMS as clear compared to images taken using 5-MP camera. Overall, this study demonstrated that dentists and OMS accepted teledentistry positively as they believe that it could assist in detection of oral mucosal lesions and improve referral decisions. This finding reflects previous research where all participants including patients, dentists, and specialists showed positive perception toward teledentristry. 24,28
Limitation
While this is the first study to demonstrate the measure of concordance between COE and teledentistry in a low resource setting, we acknowledge the intrinsic limitations that we faced during this study. The dentists had limited time to be trained to use the mobile phones for capturing images of the oral cavity therefore, the quality of the images taken were not ideal. Even though both OMS have 3 weeks of washing out period, bias may be introduced as they may still remember their diagnosis during COE when reviewing the images taken using the mobile phone. The concordance values in this study could be influenced by the spectrum of lesions included in this study, however, we had included lesions that are most commonly observed in the clinical setting to evaluate whether these are effectively detected through the images when they are presented.
Conclusions
This study shows that moderate to high concordance between COE and diagnosis from reviewing of images can be achieved. Further, the study provided evidence that the teledentistry approach can be integrated into clinical setting for patient management. It remains for the team to provide adequate training to improve its implementation on a larger scale.
Footnotes
Acknowledgments
This study was supported by Berjaya Cares Foundation, UMRG RP045A-15HTM from University of Malaya and other supporters of Cancer Research Malaysia. Cancer Research Malaysia is a nonprofit organization committed to an understanding of cancer prevention, diagnosis, and treatment through a fundamental research program.
Disclosure Statement
No competing financial interests exist.