
Abstract
Background/Introduction:
Early telerehabilitation trials with stroke survivors have shown promising results, but there remains a lack of knowledge of what areas of rehabilitation people with stroke are interested and willing to receive using technology. The purpose of this study was to describe the access to low-cost consumer technologies and willingness to use them to receive rehabilitation services among stroke survivors.
Materials and Methods:
Participants were included in this survey study if they had a stroke, lived in the community, were 19 years of age or older, and able to understand English. Participants completed a study-specific telerehabilitation survey via phone call, mail, in-person, or online. Descriptive statistics were used to characterize the sample and survey responses.
Results:
One hundred two survey responses were returned, representing a 79.1% response rate. The mean age of this urban (67.3%) and rural (32.7%) sample was 67.6 years. The technologies most commonly owned were as follows: televisions (91%), landline telephones (88.0%), and computers (79.0%). A large proportion of the sample reported an interest to receive assessments (58.4%), training and exercise programs (64.0%), and education (61.4%) via telerehabilitation, however, many were not interested to receive telerehabilitation (∼39%) and believed that the quality of care would be less than in-person rehabilitation (71.0%).
Conclusions:
The use of consumer technologies for the delivery of rehabilitation services is both feasible and desirable by stroke survivors. Telerehabilitation services at present should augment and not replace in-person rehabilitation. However, in cases where in-person rehabilitation is neither accessible nor possible, telerehabilitation could serve as an acceptable alternative and is a key area for future research.
Introduction
Stroke is a leading cause of disability worldwide. 1 Every year, of the 15 million people who have a stroke, 5 million are left with a chronic disability. 1 It is reported that at 6 years poststroke, 61% of stroke survivors continue to require assistance with performing basic activities of daily living. 2 It is therefore concerning that acute rehabilitation received in hospital may be too brief to achieve all the functional goals possible, 3 gains may be lost after discharge due to minimal follow-up, and that many people report unmet rehabilitation needs. 4 –6
Clinical guidelines recommend that stroke survivors with unmet rehabilitation goals should have timely access to specialized rehabilitation services. 7,8 A positive relationship exists between increased amounts of therapy time and meaningful improvements following a stroke. 9 However, both urban and rural populations can be limited in their access to traditional in-person stroke services following discharge due to high demand, lack of specialized services, difficulty leaving the home, or lack of transportation. 10,11 Investigation of alternate service delivery models that are accessible, flexible, and equally therapeutic is necessary.
Telerehabilitation, a new and developing field of telehealth, is the use of technology to remotely deliver rehabilitation services to patients with transportation barriers or separated by geographical distance. 12 –14 Telerehabilitation includes all aspects of rehabilitation, including therapeutic intervention, prevention, supervision and monitoring of progress, education, counseling, and patient assessment. 10,12 –16 Research has shown that telerehabilitation can decrease long-term disability, increase secondary prevention, and allow for an earlier supported discharge. 12,14,17 Importantly, telerehabilitation has the potential to provide longer follow-up after discharge from acute care, thereby increasing the positive dose–response of therapy time. 9 Effectiveness of telerehabilitation following a stroke continues to be an area of research; however, early trials have shown promising results for its utilization. 18
Telerehabilitation has historically used expensive technologies delivered to health centers, rather than focusing on inexpensive readily available technologies that can be delivered in a home setting. 10,19 Low-cost consumer technologies, such as the computer, Internet, and telephone, are becoming more frequently owned and used among the public, particularly among older individuals. In 2009, 66% of Canadians aged 65 and older used the Internet at home, a proportion that has steadily increased since 2005. 20 Thus, telerehabilitation delivered using low-cost consumer technologies is a plausible solution to increase access to stroke rehabilitation. However, a greater understanding of the technological preferences of people with stroke and their perspectives of using technology to receive telerehabilitation for their stroke recovery is warranted. The purpose of this study is to investigate the access to consumer technologies and willingness to use them to receive rehabilitation services among stroke survivors.
Materials and Methods
Study Design and Participants
Individuals who have had a stroke were included in this cross-sectional survey, if they lived in the community and were able to provide informed consent, 19 years of age or older, and able to understand English. Participants were recruited from March to April 2015. Individuals from a rehabilitation hospital's research database were contacted by the research team and provided study information. The research team also presented the study to stroke recovery groups (in both urban and rural settings) and requested stroke advocacy and community groups to send study information to their membership and post information on their Web sites.
Measures
Participants completed a demographic and stroke information form comprising questions related to age, sex, ethnicity, marital status, employment status, education, income, and population setting. Questions were also asked about the number of strokes, time since last stroke, and type of stroke. We used the modified Rankin Scale (mRS) to describe the sample's stroke severity. The mRS is a reliable and valid 21 scale that measures the level of poststroke functional independence. 22 Participants are asked about their ability to perform various functional tasks and are assigned a severity level, ranging from 0 to 5, based on their responses. Higher scores indicate a greater stroke severity. We used the functional comorbidity index (FCI) to describe the number of comorbid conditions each participant had. 23 The FCI total score is a sum of 18 self-reported comorbid conditions and ranges from 0 to 18. Higher scores indicate greater comorbidity. FCI measurements have been shown to be associated with hypothesized levels of physical function. 23
Communication technology survey
This study-specific survey was developed by the research team to obtain information on the following: 1. Access to rehabilitation services following stroke (e.g., type of rehabilitation, location, and distance to travel to receive rehabilitation) and difficulties with access (no difficulty/some difficulty/a lot of difficulty). 2. Use of communication technologies (e.g., technologies that people have access to, frequency of use (never/once per month/once per week/daily) and confidence with using technology (not confident/somewhat confident/very confident). 3. Perspectives of telerehabilitation (e.g., previous experience [yes/no] and satisfaction [very satisfied, somewhat satisfied, somewhat unsatisfied, or very unsatisfied, with telerehabilitation], interest to receive telerehabilitation for assessments, training or exercise programs, and education [very interested, somewhat interested, or not interested], and agreement on advantages/disadvantages of telerehabilitation [strongly disagree, disagree, agree, or strongly agree]).
Research Protocol
Interested individuals contacted the research team to receive more information about the study. After providing informed consent to participate in the study, participants were given the option to complete the study questionnaires by phone, online, in-person, or by mail. Reminders by e-mail or phone calls were given to participants who had not completed the survey after 2 and 4 weeks. All participants received a $10 gift card. Approval for this study was obtained from the university's research ethics board and the local health authority.
Data Analysis
Descriptive statistics were used to characterize the samples and their responses to the survey items. Some item responses were combined together for concise data description. For example, the response options “some difficulty” and “a lot of difficulty” were grouped together to describe the percentage of people with difficulties getting to appointments due to health, transport, or cost; for questions asking level of interest in telerehabilitation, options for “very interested” and “somewhat interested” were grouped together; and when the survey asked a respondent to rate whether they “strongly agree” or “somewhat agree” with a statement, these options were combined together for a percentage of those who agree.
For items inquiring about interest to receive assessments, training or exercise programs, or education about stroke rehabilitation via telerehabilitation, we used chi-square analyses to assess for differences in interest (i.e., more vs. less interest) by age (≥65 years vs. <65 years), work status (working vs. retired), sex (male vs. female), and population setting (large population vs. medium, small, and rural). All data were analyzed using SPSS (Version 23.0).
Results
In total, 129 individuals contacted the research team and expressed interest to complete the survey (29 by mail, 4 by phone, 59 online, 37 written in person). Of these, 102 were returned to the research team representing a response rate of 79.1%. However, due to missing data, the number of responses for each item ranged between 92 and 102.
The mean age of this mostly male (56.9%) sample was 67.6 years. Sixty-five percent of the sample reported being married or common-law and 56.9% retired. Sixty-seven percent of the sample reported being from a large population center (i.e., >100,000 people). Seventy-three percent reported having only one stroke, with a mean of 8 years since the last stroke. Such an observation concurs with epidemiological data, which show that one-quarter of the annual number of strokes are secondary events. 24 Sixty-four percent of the sample reported an mRS score between 3 and 5, indicating moderate (24.2%), moderately severe (35.4%), or severe (4%) disabilities resulting from the stroke. Demographic and stroke data are further detailed in Table 1.
Sample Characteristics and Health-Related Information
Access to Rehabilitation Services
Many participants received physical therapy (90.2%), occupational therapy (73.5), speech language therapy (58.8%), and saw a rehabilitation physician (41.2%) following their stroke. Four participants (3.9%) reported not receiving any therapy. The majority of respondents received rehabilitation as in-patients in a hospital (81.4%) and through outpatient appointments at a hospital (65.7%). A lesser amount of participants reported private (24.5%) or home-based (24.5%) rehabilitation appointments. Most participants (76.0%) travelled less than 25 km to attend their rehabilitation appointments following their stroke, however, one respondent reported travelling more than 100 km to attend appointments.
When asked about the level of difficulty of getting enough rehabilitation following discharge from the hospital, 48.0% reported having “some” or “a lot of” difficulty. Similarly, 39.2% reported difficulties having questions answered, 38.8% reported difficulties attending appointments due to health issues, 41.8% had difficulties getting to appointments due to transport and travel, and 27.6% reported difficulties due to costs of transport and travel.
Use of Communication Technologies
Figure 1 presents the ownership of consumer technologies by respondents that may be used for the delivery of telerehabilitation. All respondents reported owning at least one device. Ninety-one percent of the sample owned three or more devices.

Ownership of consumer technologies.
Of the people owning a landline telephone, cell phone, television, computer, and/or tablet, most reported using them on a daily basis (68.0%, 43.2%, 88.7%, 64.2%, 33.0%, respectively). Nine percent reported owning a gaming console. Of these participants, only 3% used the console on a daily basis. Ninety-one percent of the sample reported use of the Internet, of which 71.0% used the Internet on a daily basis. Ninety percent reported using e-mail, with 64.9% e-mailing on a daily basis. Frequency of technology use is detailed in Figure 2.

Usage of currently owned technologies.
Less than 10% reported being not confident with using each technology, suggesting that more than 90% of the sample were “somewhat” or “very” confident with using the technologies. Respondents reported being most confident with using televisions, landline telephone, e-mail, Internet, and computers, as shown in Figure 3.

Confidence with using currently owned technologies.
Perspectives of Telerehabilitation
Thirteen people (12.7%) reported previous telerehabilitation experiences (e.g., the delivery of rehabilitation exercises using the Wii Fit gaming console). All of these people reported being “somewhat” (n = 6) or “very” (n = 7) satisfied with their telerehabilitation. One person commented that their telerehabilitation was “very helpful since it eliminates the travel time and gasoline expense.” Another person commented that, “it would be better if you can see face-to-face, one-on-one (with the therapist).”
More than half the sample reported an interest to receive assessments (58.4%), training and exercise programs (64.0%), and education (61.4%) via telerehabilitation. Figure 4a–c shows the interest to receive rehabilitation services by technological device. The devices that received the greatest amount of interest averaged across the rehabilitation services were computer (72.9% were “somewhat” or “very” interested), television (68.7%), and landline telephone (59.4%). In addition, 72.8% and 70.1% of people expressed interest to receive telerehabilitation using the Internet and e-mail, respectively. The use of gaming consoles received the least amount of interest (27.2%).
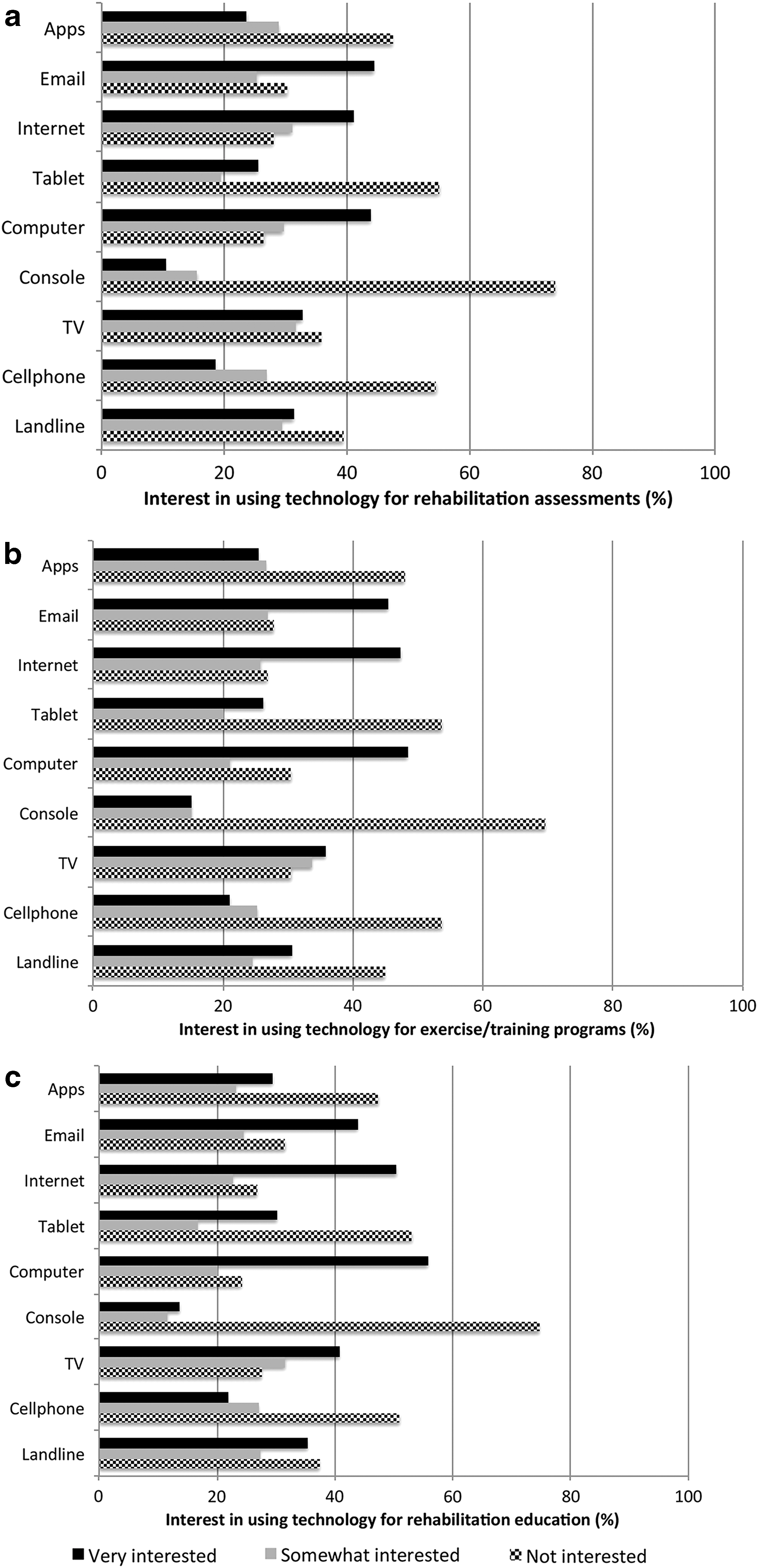
Chi-square analyses demonstrated that individuals younger than 65 had a greater interest to receive training and exercise programs (78.0% vs. 53.4%), as well as education about stroke rehabilitation (78.0% vs. 49.2%) through telerehabilitation, compared to individuals 65 years of age and older (p < 0.05). Similarly, significantly more individuals who were not retired reported a greater interest to receive training and exercise programs (76.2% vs. 55.2%), as well as education (72.1% vs. 53.4%), than individuals who were retired.
When asked to rate interest level on specific applications of telerehabilitation, respondents were most interested in exercise-based applications, such as using sensors to practice balance exercises (83.0%), watching home videos of prescribed exercises with a telephone follow-up (81.2%), and working on exercises with a therapist in real time (80.2%). Other applications asked about included the following: having rehabilitation questions answered via Internet chat or video conference (75.0%), assessing home adaptations through video/webcam (75.0%), and using an electronic journal to submit updates (66.0%).
The majority of respondents agreed that telerehabilitation would make them feel more independent (73.3%) and more confident in managing their progress (77.5%), as well as save them money in travel expenses (72.7%). The majority also agreed that they would like to have received rehabilitation in their home environment (84.2%) and agreed that telerehabilitation would make accessing stroke care easier (82.8%) and enhance current care (72.0%). However, there was also agreement that telerehabilitation would result in fewer in-person interactions with rehabilitation professionals (78.5%), that these interactions would be missed (89.0%), and that quality of care might be less than face-to-face (71.0%). Respondents were divided on their opinion of whether they would not want to discuss sensitive information over technology, with 48.0% agreeing with this statement.
Discussion
This study surveyed community-living individuals with stroke on their experiences with accessing rehabilitation services, uses of consumer technologies, and willingness to use those technologies to receive telerehabilitation. Almost all respondents reported having some form of rehabilitation at some point in their care following a stroke, however, a lesser proportion received outpatient therapy, and an even smaller group participated in private or home care therapy. Moreover, despite most of our samples residing in large city centers, where stroke rehabilitation services are more widely offered, almost half of the respondents reported having at least some difficulty getting enough or adequate rehabilitation postdischarge.
Our research indicates that the use of low-cost consumer technologies for the delivery of stroke rehabilitation services is both feasible and desired. Participants reported a strong interest to receive telerehabilitation via the same technologies in which they have a high confidence using (i.e., computers, the Internet, e-mail, television, and landline phone). This observation is similar to research in the general telehealth literature among people with chronic diseases, 25 however, our results are unique, in which we specifically report on the provision of stroke rehabilitation using technology. We also report on interest to receive specific applications of rehabilitation services, such as assessments, delivery of exercise programs, and education, using technology and not on “health services” in general as previously described. 25,26 By identifying the aspects of rehabilitation, people are interested in receiving via technology and also by what technology our findings may help to accelerate the development and acceptability of stroke telerehabilitation.
Many of our participants expressed interest to receive rehabilitation assessments, training/exercise programs, and education using some form of technology. Despite most of the samples having no experience with telerehabilitation, many participants expressed positive beliefs about the potential of telerehabilitation. Importantly, many agreed that telerehabilitation would promote their independence and help to manage their recovery and progress. Although such findings are positive and support the use of telerehabilitation for stroke recovery, they also raise challenges for rehabilitation professionals. 27 For example, a key issue facing clinicians is how to conduct assessments or provide interventions that are typically “hands on”. Such an issue speaks to a need to modify current techniques and training, for example, to bypass the need for a hands-on approach and to perhaps instead engage the assistance of a family member or a caregiver. 28 Thus, telerehabilitation using consumer technologies has the potential to not only increase access to and facilitate stroke rehabilitation services but to also evolve the way in which stroke rehabilitation is delivered and accomplished. It is therefore notable that research has described many benefits of home-based stroke rehabilitation, including satisfying patient choice/decision-making, improving functional outcomes, reducing length of hospital stay, improving physical health, cost-effectiveness, and reducing caregiver strain 29 –32 and more that our participants agreed that receiving telerehabilitation in their home would be beneficial to them.
More than 60% of our sample reported an mRS score between 3 and 5, suggesting moderately severe to severe limitations following their stroke. 21,22 Despite this stroke severity, our participants were still interested in using technology for rehabilitation. It is then plausible that if the technological devices were adapted for people with physical and functional deficits, then there would be greater interest in telerehabilitation. Bimanual tasks, such as typing or holding a phone while using the other hand, were reported the most difficult by respondents. Possible solutions and areas of research to address such barriers include developing adaptive equipment to ensure functionality and ease of use, such as an enlarged keyboard, visual and audio cues, stabilizers, or stands for necessary equipment.
Despite many participants agreeing on several benefits of telerehabilitation, they also raised several concerns, including that telerehabilitation would result in having fewer interactions with rehabilitation professionals, the quality of care would be less than in-person, and they would miss the social interactions. Furthermore, it is notable that ∼20%, 30%, and 45% of our samples reported not owning a computer, cell phone, or tablet, respectively, and that 42%, 36%, and 39% of participants (when averaged across all technologies) were not interested to receive assessments, training or exercise programs, and education, respectively, via telerehabilitation. This suggests that a substantial proportion of people with stroke would not be able to access telerehabilitation services or willing to receive rehabilitation using technology. Thus, although our findings suggest many people are willing and interested to receive telerehabilitation, it is not a blanket solution to increase rehabilitation capacity or access to such services. Rather, it is plausible that telerehabilitation services at present should augment and not replace in-person rehabilitation. However, in cases where in-person rehabilitation is neither accessible nor possible, telerehabilitation could serve as an acceptable alternative. Therefore, identifying service gaps along the rehabilitation continuum and developing and evaluating telerehabilitation programs to fill those gaps are key areas for future research.
Limitations
Our study may have had a volunteer bias in that individuals who have more access and familiarity with technological devices may have been more likely to participate in the study. However, ∼20% and 30% of the participants did not own a computer or cell phone, respectively, suggesting that there was a representative proportion with lower technology experience. The self-report nature of our data may be biased by social desirability and influenced by the way in which the data were collected (e.g., online vs. telephone vs. in-person responses). In addition, our results reflect the perspectives of people with stroke who are only one stakeholder in the development, evaluation, and implementation of telerehabilitation. Equally important to learn are the perspectives of clinicians and administrators on the use of telerehabilitation for stroke recovery, which is an area for future research. Finally, because information about the study was posted online and sent to members of community groups, we do not have an accurate number of individuals who were aware of the study and decided not to participate. Despite this, 79% of the individuals who had access to the survey provided responses.
Conclusions
The use of low-cost consumer technologies for the delivery of rehabilitation services is both feasible and desirable by stroke survivors. Stroke survivors currently feel most confident using the television, computer, and landline phone. These technologies are also the most commonly owned and, including the use of e-mail, they also received the most interest by stroke survivors for use in telerehabilitation. A substantial proportion of stroke survivors are not interested in receiving telerehabilitation and do not own all technologies. Therefore, efforts should also be made to educate and provide demonstrations about what technologies can assist with to increase interest. Thus, it is plausible that telerehabilitation at present could augment and not replace in-person rehabilitation. However, in cases where in-person rehabilitation is neither accessible nor possible, telerehabilitation could serve as an acceptable alternative.
Footnotes
Acknowledgments
This work was supported by Canadian Institutes of Health Research Postdoctoral Fellowship (B.M.S.) and Operating Grant; Michael Smith Foundation for Health Research Postdoctoral Fellowship (B.M.S.) and Senior Scholar Award (J.J.E.); Canada Research Chair in Neurological Rehabilitation (J.J.E.); and the Heart and Stroke Foundation Canadian Partnership for Stroke Recovery Operating Grant.
Disclosure Statement
No competing financial interests exist.