
Abstract
Introduction
Arecent explosion in the wearable technology market has resulted in a number of commercially available health monitors, activity trackers, and heart rate (HR) monitors. They are designed to suit the novice beginner to the serious athlete. Monitoring of HR during physical activity and exercising allows for real-time control of exercise intensity and training effect. 1 A number of these monitors have been evaluated for accuracy and precision against the electrocardiogram (ECG) with varying results. 2
Many of these devices are available commercially for personal use. It is our hope that this technology can be leveraged in the healthcare clinical setting in expanding the care we currently provide to our patients. Preoperative optimization programs seek to implement a series of interventions to improve and enhance recovery after major surgery. Important aspects of this are the use of exercise programs. 3 –6 Published data from our group indicate that barriers to successful completion of these programs exist for a significant group of our patients and could be due to inaccessibility to in-hospital supervised exercise programs. 7
We focus on assisting our patients presenting to prehabilitative services in preparation for major cancer surgery in our institution through telephysiotherapy. Telephysiotherapy is the development of telemonitoring systems to facilitate independent rehabilitation or, in our case, prehabilitation of patients within their homes. 8 To the best of our knowledge, no such program exists within our healthcare system to date.
The MYZONE® MZ-3 HR monitor is a popular recreational fitness device that is also priced at a level that would be affordable to a hospital prehabilitation service. It utilizes a system of targeted HR zones based on an individual's predicted maximum HR for goal setting and training effectiveness.
The MYZONE MZ-3 HR monitor and fitness tracker provides instant effort feedback by utilizing technology that detects cardiac electrical activity. It records and transmits HRs at a frequency of 1 Hz to a Bluetooth-enabled device with the MYZONE application installed. The MYZONE MZ-3 is marketed as being accurate to 99.4% when compared with ECG. However, there has been no published data to date investigating the precision and accuracy of the monitor compared with a Class II, FDA-approved ECG monitor.
Objective
In our evaluation of the MYZONE MZ-3 HR monitor, we aim to examine the reliability of this technology against a clinical ECG monitor (Class II, FDA approved). Specifically, we looked to examine its accuracy, a measure of how close the value is to the actual (true) value, and its precision, a measure of how close the values are to each other. Figure 1 shows an illustrative representation of these two terms. This problem can be handled, in part, using a Bland–Altman analysis. Bland–Altman analysis determines the bias, or mean difference between the MYZONE MZ-3 and ECG, as a measure of accuracy and the 95% limits of agreement (LOA) as a measure of precision. 9,10
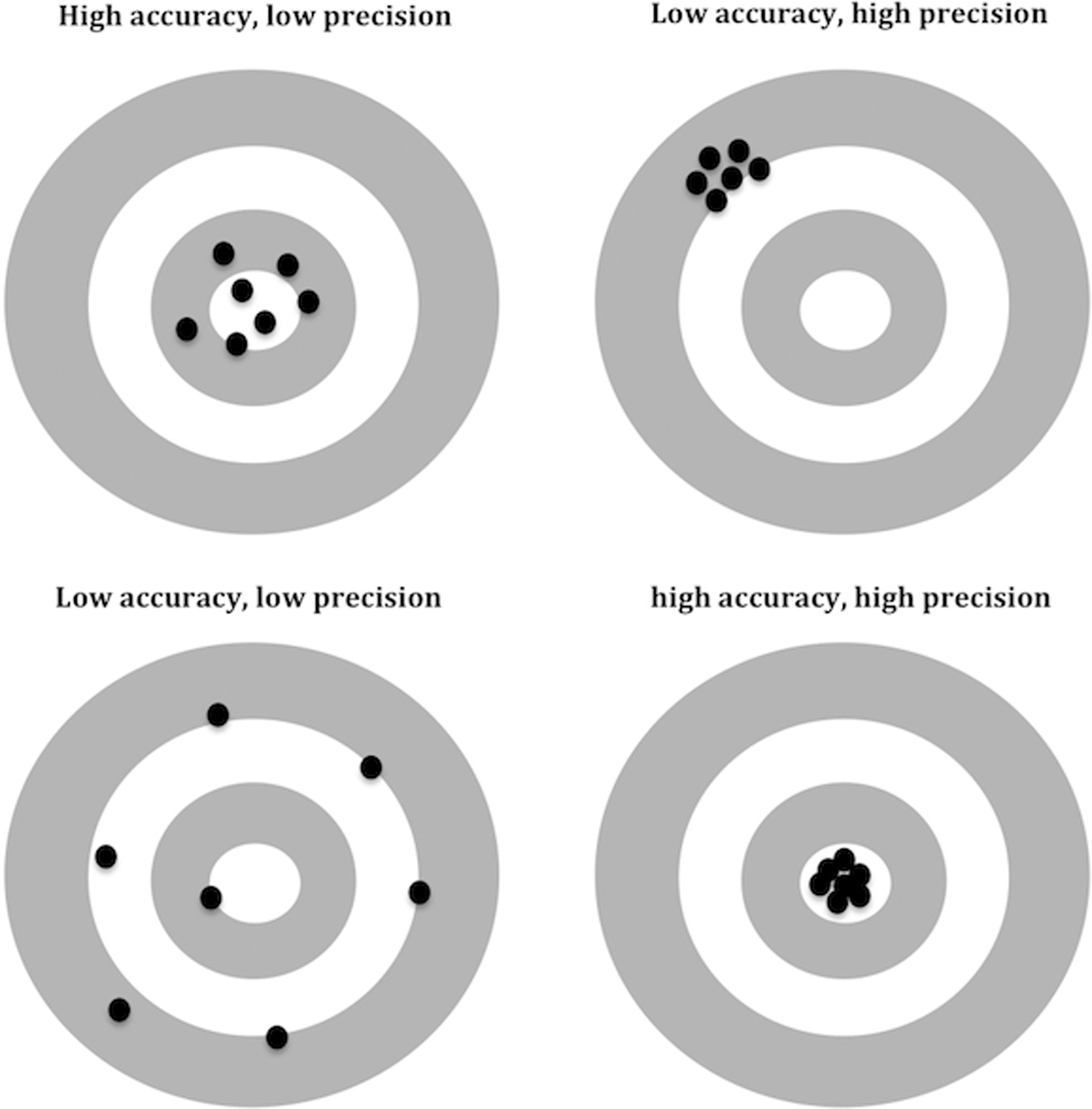
Accuracy and precision.
The goal of this study is to pilot the MYZONE MZ-3 HR monitor to assess its level of reliability to provide a feasible telephysiotherapy prehabilitation service through prescription-based exercise programs to patients presenting for major cancer surgery within our leading oncological health service.
Materials and Methods
Participants
Potential participants were recruited as a convenience sample. Participants selected for involvement in this study were young and physically active and had no major medical disease or current medications that would preclude them from undertaking vigorous physical activity or effect their HR. Verbal consent was obtained from each participant before testing. Participants were advised to refrain from consuming alcohol or caffeine in the 2 h preceding the test. All participants were in sinus rhythm at rest and throughout the test.
Data Recording Conditions
Participants performed the recordings during rest and exercise conditions on an exercise bike. Each participant was instructed to perform an increasing level of continuous vigorous high-intensity exercise causing rapid and wide variations in HR. The mean continuous recording time of each participant was 23:59 (±6:01) min. Five participants (1–5) used their own MYZONE MZ-3 device and the remaining two participants (6 and 7) shared the same device.
Measurements
We used a GE Healthcare Datex-Ohmeda S5 Compact Anesthesia Monitor (General Electric Company) to measure the ECG of our participants using a three-lead format. The Datex-Ohmeda S5 monitor was connected to a Windows-based PC utilizing its built-in RS232 (COM) Port through a USB to a serial adapter and cable. A C# .NET freeware application, VitalSignsCapture v1.004, was used to capture and record the ECG HR in real time to a comma separated (CSV) file on the PC. The MYZONE MZ-3 chest strap and device was fitted on our participants as outlined in MYZONE's instruction manual. A MYZONE-specific receiver was connected to our Windows-based PC through a USB. MYZONE MZ-3 HR was captured and recorded to a CSV file using MYZONE's admin console application (MYZONE Admin Console). ECG leads were secured to the subject to reduce “noise” and movement artifact during testing.
To ensure correct matching of HR on both the ECG and MYZONE monitors, the system clock on the Datex-Ohmeda S5 monitor was manually synchronized with the PC hosting the MYZONE admin console.
The VitalSignsCapture software polled the Datex-Ohmeda S5 monitor and recorded HR information at 5-s intervals. The MYZONE configuration recorded HR at 1-s intervals.
All subjects were observed before commencement of exercise to ensure good signaling of HR for both devices.
Statistical Analysis
The agreement between the MYZONE MZ-3 and ECG was analyzed using a Bland–Altman plot. To account for several paired measurements for each participant, the analysis was adjusted to repeated observations derived from the same participants. 11,12 The bias (mean difference), standard deviation (SD), 95% LOA, and plot were derived using SPSS for Windows (version 23; IBM).
Paired HR data from each participant were matched on the basis of time stamps as logged by our recording software. Since MYZONE HR was recorded on a second-to-second interval, it was matched to the corresponding Datex-Ohmeda S5 HR. The remaining MYZONE HRs with unpaired Datex-Ohemda S5 HRs were excluded from our analysis.
On a number of occasions, the MYZONE MZ-3 HR was not captured and thus could not be paired to the corresponding Datex-Ohmeda S5 HR. It is our assumption that during these periods, there was a brief loss of contact either between the MYZONE MZ-3 and the participant or between the MYZONE MZ-3 and MYZONE USB receiver. Fifty-five data points remained unpaired from a total of 1,983 data points.
On analysis of our data, we noted an asynchrony between the Datex-Ohmeda S5-captured HR and the MYZONE MZ-3-captured HR from five of our participants. These five participants were tested on the same day. Despite our best efforts to manually synchronize clocks for both of our recording software, it is possible that our data points were not perfectly synchronized. We corrected this asynchrony by shifting our ECG obtained HR to the left by 20 s (Fig. 2). We acknowledge this correction as an adjustment to the data acquisition speed with no filtering or elimination of data points and consider it unlikely to have any clinically significant effects on our results.

Heart rate measured by ECG and MYZONE® for one participant.
Results
A total of seven healthy participants were included in the study. Mean age of the participants was 29.7 (±7.0) years. There were five female and two male participants. The total number of paired HR data points was 1,928 for all seven participants. The results (see Fig. 3) show that the bias between ECG and the MYZONE MZ-3 was 0.4 beats per minute (bpm). Adjusted 95% LOA were found to be −4.5 to 5.3 bpm. The percentage error (95% LOA/mean HR) was 3.6%.
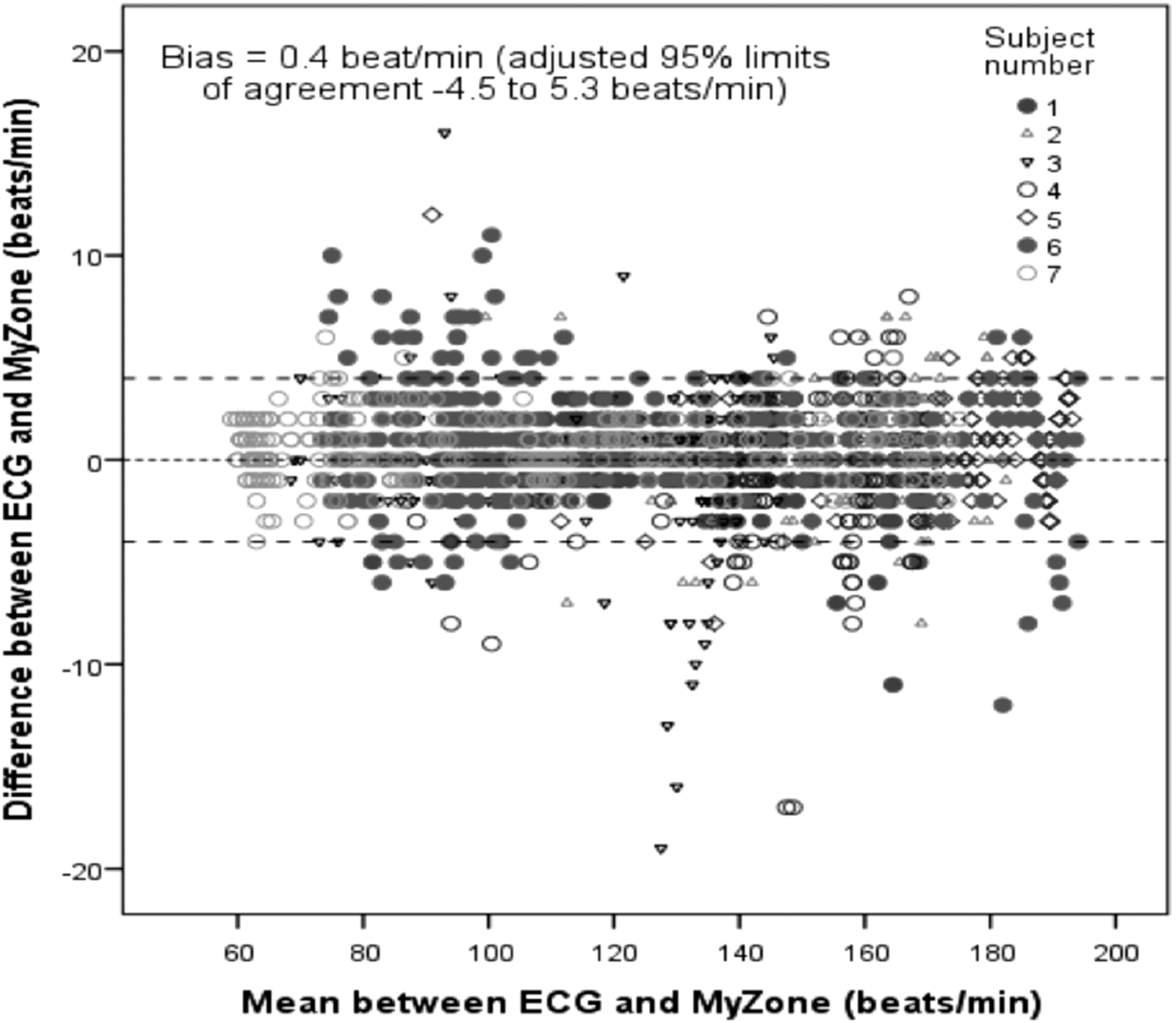
Bland–Altman plot for ECG and MYZONE MZ-3.
Discussion
This exploratory study was conducted with a view to selecting an ideal HR monitor for use in a community-based prehabilitaion program in patients presenting for major cancer surgery.
The ideal monitor for this purpose should have the following characteristics: 1. Have acceptable levels of precision and accuracy compared with a clinically validated ECG monitor. 2. Ease of use for elderly patients. 3. Affordability for use by patients and the prehabilitation program.
The results of this study indicate that the MYZONE MZ-3 HR monitor has an acceptable level of reliability (bias 0.4 bpm) and accuracy (95% LOA −4.5 to +5.3 bpm) during testing in healthy volunteers.
This study has several drawbacks including the lack of a structured exercise protocol during exercise testing. However, the instructions given to the participants resulted in an acceptable range and distribution of HRs.
Also, the need to retrospectively apply a 20-s correction to synchronize the data streams for five participants could be construed as a potential inaccuracy in the analysis. We performed a Bland–Altman analysis on the uncorrected data, and the resulting bias (0.4 bpm) and 95% LOA (−5 to +5 bpm) were not clinically significant for the purposes of telephysiotherapy as the difference in HR was consistent across the whole data set.
We studied this device in healthy volunteers, and the reproducibility of these results may be affected by the presence of lung disease, pleural effusions, breast implants, cardiac dysrhythmias, and obesity.
Conclusion
The commercially available MYZONE MZ-3 HR monitor has an acceptable level of reliability for use in healthy volunteers performing exercise across a wide range of HRs.
Further studies using a similar methodology are required to validate the use of the MYZONE MZ-3 in patients presenting for cancer surgery.
The device can be potentially used for delivering telephysiotherapy to patients undergoing major cancer surgery. Prehabilitation services can use these devices to prescribe and monitor exercise progress and improvement that we hope will have a meaningful impact on recovery from major surgery.
Footnotes
Acknowledgments
The authors would like to thank the volunteers for their time and the Voyage Fitness Pakenham, Victoria, Australia, for providing the equipment and facility for conducting the study. We would also like to thank MYZONE for providing the MZ-3 HR monitor and receiver used in this study. Dr K.H. would like to thank WA Health and Raine Medical Research Foundation for their support through the Raine Clinical Research Fellowship.
Disclosure Statement
No competing financial interests exist.