
Abstract
Background:
Prenatal diagnosis of complex congenital heart disease (CHD) has been shown to improve newborn outcomes. The rate of prenatal diagnosis and access to fetal echocardiography vary widely across the United States.
Introduction:
A clinical fetal tele-echo service was established at King's Daughters Medical Center (KDMC) in Ashland, KY, a region in eastern Kentucky that is 3 h from the nearest congenital heart surgeon. The aim of this study was to determine if fetal tele-echo utilizing local sonographers at a small regional hospital can accurately and efficiently identify fetuses with complex CHD.
Methods:
Medical records were reviewed for all mother–infant pairs who had fetal tele-echoes performed at KDMC and interpreted by University of Louisville pediatric cardiology between March 2011 and December 2013. Findings on fetal tele-echo were compared to newborn echo and clinical course, and divided into four groups: (1) Correct—no difference between fetal tele-echo and newborn echo, (2) Likely Correct—normal fetal tele-echo and benign newborn course, (3) Major Difference—one that affected newborn clinical course, and (4) Minor Difference—did not affect clinical course.
Results:
Seventy-five mother–infant pairs were analyzed. Fetal tele-echoes were Correct in 21%, Likely Correct in 56%, showed Major Differences in 0%, and showed Minor Differences in 23%. For identifying complex CHD, fetal tele-echo had a sensitivity and specificity of 100%. The average number of fetal echocardiograms per mother–infant pair was 1.1.
Discussion:
Fetal tele-echocardiography performed by local sonographers at a small regional hospital can accurately and efficiently identify fetuses with complex CHD.
Introduction
Prenatal diagnosis improves newborn outcomes for patients born with serious congenital heart defects. Congenital heart defects are the most common birth defect, occurring in around 1 in 100 live births. 1 Some of these defects are mild, but others can cause death in the newborn period if undetected or untreated. Prenatal diagnosis of congenital heart defects allows for planning and preparation, both with regard to location and timing of delivery, and also availability of optimal newborn care. Infants with a prenatal diagnosis can be optimized to be in a more favorable physiologic state before operative repair, 2,3 resulting in less perioperative and long-term morbidity 4,5 and mortality. 3,6 –8 Patients without prenatal diagnosis often require emergent medical care and transport, both of which significantly increase the cost of care for these patients. 9
The rates of prenatal diagnosis of heart defects vary widely in the United States and around the world. Obstetrical screening has been shown to detect only 10–26% of heart defects, while for those who are found and referred, a fetal echocardiogram in experienced hands can identify the details of heart defects 90% of the time. 10 For patients undergoing newborn heart surgery, previous published studies have found overall rates of prenatal diagnosis of congenital heart defects from 28% to 67%. 4,11 We have previously shown that infants with heart defects requiring surgery or intervention before 1 year of age at Kosair Children's Hospital (KCH) in Louisville, KY, had a prenatal diagnosis only 28% of the time. 12
The state of Kentucky has many healthcare needs. Our center, KCH, is the only center in the state where pediatric patients can undergo cardiovascular surgery. The United Health Foundation's 2014 ranking of state health placed Kentucky at 47 out of 50 overall. 13 In an effort to improve the rate of prenatal diagnosis of congenital heart disease (CHD) in Kentucky, the University of Louisville (UofL) Division of Pediatric Cardiology established a fetal tele-echocardiography service at King's Daughters Medical Center (KDMC) in Ashland, Kentucky. Compared to previous studies looking at fetal tele-echo, the unique aspects of this program are: (1) the use of local sonographers employed by the small regional hospital to perform fetal echocardiograms rather than sending someone from the pediatric cardiac center to obtain the scans, 14 (2) the geographic distance of 190 miles or 3 h by car between the regional hospital and the cardiac center, 14 –16 (3) the use of store-and-forward telemedicine to allow interpreting physicians at the cardiac center to optimize workflow and efficiency, 14 –16 and (4) the expectation that sonographers at the regional hospital obtain all of the images for a complete fetal echocardiogram to be sent for interpretation. 17
Methods
This was a retrospective chart review. Our patient population was all mother–infant pairs who had fetal tele-echocardiograms preformed at KDMC in collaboration with UofL Division of Pediatric Cardiology between the dates of March 2011 through December 2013. Mother–infant pairs for whom no newborn information was available were excluded. All of the information collected was documented in the electronic medical record as part of routine peripartum and newborn care at KCH and/or KDMC. No additional information was collected from mothers or infants for the purposes of this study. This study was approved by the Institutional Review Boards of the UofL, KCH, and KDMC.
All fetal echocardiogram images were obtained by two local sonographers in Ashland, KY, who were employed by KDMC. One was a senior sonographer with extensive experience who was registered in obstetrical (OB) ultrasound and the other was the technical director of the KDMC echo laboratory and was registered in echocardiography for adults and pediatrics. Neither of the sonographers had performed fetal echocardiograms previously, but both had done extensive self-study before formal training using A Practical guide to Fetal Echocardiography: Normal and Abnormal Hearts by Abuhamad and Chaoui. 18 Fetal echocardiography training was provided by a pediatric cardiologist from UofL over a 4-month period. Training consisted of formal lectures with handouts and video examples and 6 days of life scanning with the pediatric cardiologist, which alternated between KDMC in Ashland, KY, and KCH in Louisville. Then, a series of practice scans were performed on volunteer patients by the sonographers at KDMC and images were sent to KCH where they were reviewed by the pediatric cardiologist and detailed feedback was given. The images of volunteers who were scanned as part of the training were de-identified and no reports were generated as part of the medical record. One of the sonographers became credentialed in fetal echo by the American Registry for Diagnostic Medical Sonography during the study period.
Complete fetal echocardiograms were obtained at KDMC following the protocol (Supplementary Data; Supplementary Data are available online at
Prenatal echocardiograms were interpreted as normal if they showed normal fetal cardiac anatomy and function. Isolated fetal premature atrial contractions were classified as normal. Abnormalities noted on fetal echocardiography were classified as likely to require urgent intervention at birth or not. Postnatal echocardiograms were interpreted as normal if they showed normal newborn cardiac anatomy and function; isolated patent ductus arteriosus and/or small patent foramen ovale were classified as normal. 20 Abnormalities seen on postnatal echocardiogram were divided into critical and noncritical lesions, critical lesions being those expected to require surgery or catheter intervention within the first year of life. 21 The infant's newborn clinical course was reviewed in the electronic medical record at KCH and KDMC, which included the newborn hospitalization and any newborn outpatient visits, emergency room visits, or subsequent hospitalizations at KDMC. If there was no evidence of cardiac abnormality in the electronic medical record, the infant was presumed to not have complex CHD.
Since this is a retrospective review with descriptive data, results were placed into two-by-two tables for analysis. No further statistical analysis was done on this data set.
For patients with no postnatal echocardiogram, length of follow-up was determined by the last available medical records. For patients with postnatal echocardiogram, date of last follow-up was either the date of last clinical documentation or echocardiogram, whichever came later.
Results
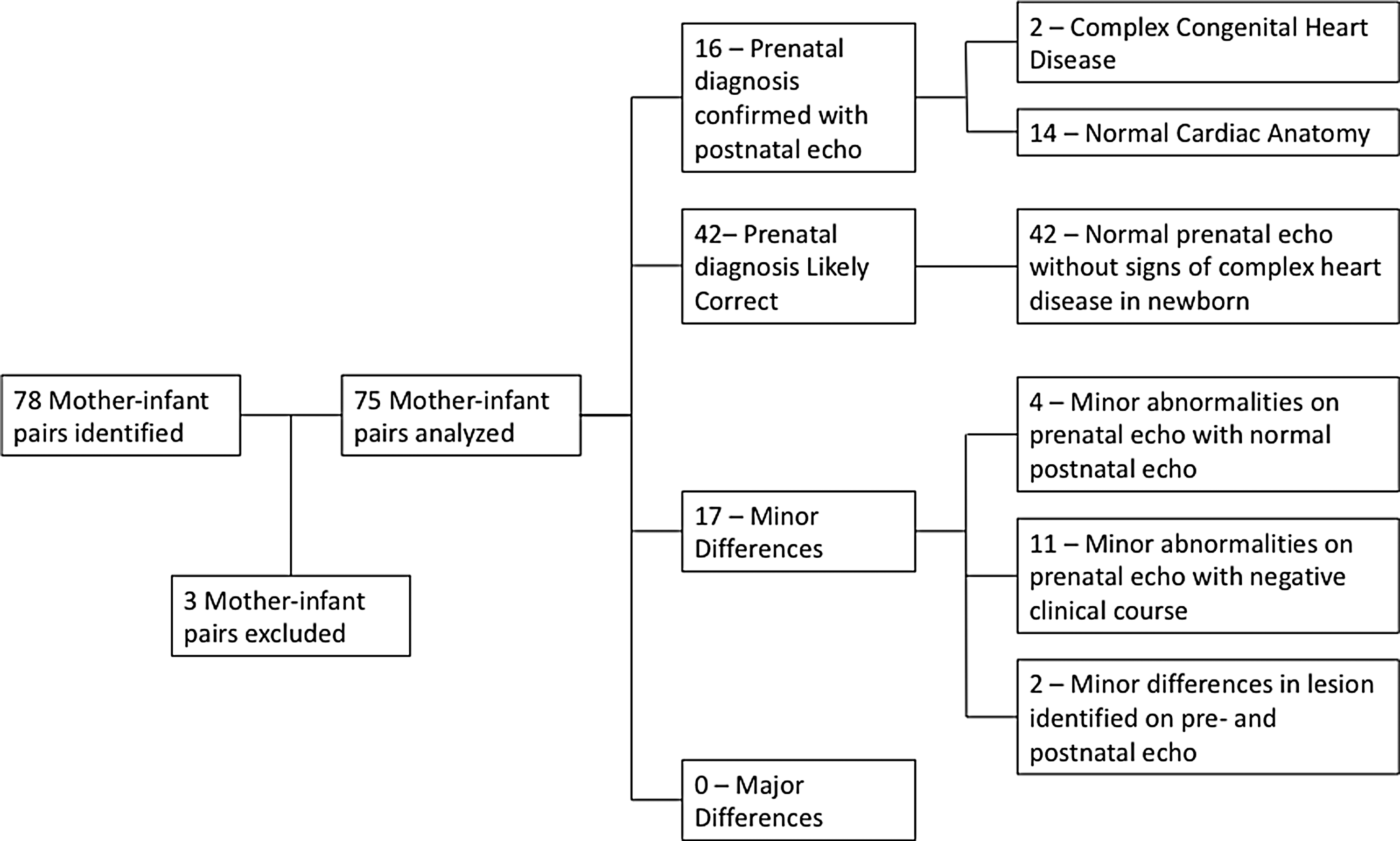
In the time between March 2011 and December 2013, 78 women had fetal tele-echocardiograms performed at KDMC and interpreted by UofL Division of Pediatric Cardiology. Three mother–infant pairs were excluded from the final analysis due to the newborn records not being available in the electronic medical record. The remaining 75 mother–infant pairs were analyzed.
The median gestational age of the fetus at time of first prenatal echocardiogram was 26 weeks 5 days, range 19–36 weeks of gestational age. If the gestational age was not included in the echocardiogram report, it was extrapolated from gestational age at birth and date of echocardiogram. If there was a discrepancy between biparietal diameter and age by last menstrual period, biparietal diameter was used.
Indication for fetal echocardiogram was either stated on the echo report or presumed based on the medical records reviewed (Table 1). We did not have access to medical records from the requesting obstetrician. For 21 mother–infant pairs, there was no documentation of the indication for fetal echo available, due to a problem transcribing handwritten orders into the electronic medical record during the early study period.
Patient Characteristics
Two infants had prenatal diagnoses of complex CHD expected to require urgent intervention after birth, which were confirmed on postnatal echocardiograms (Table 2). Fourteen infants had normal pre- and postnatal echocardiograms, giving a total of 16 mother–infant pairs with confirmed correct cardiac anatomy. Forty-two infants had normal prenatal echocardiograms performed and did not have postnatal echocardiograms but had benign clinical courses and no evidence of cardiac abnormality in the electronic medical record, and so, they were presumed not to have complex CHD and the prenatal echo was likely correct. There were no major differences identified. Two infants had a minor abnormality identified on prenatal echocardiogram but a different, noncritical, lesion diagnosed on postnatal echocardiogram. Eleven infants had mild abnormalities on prenatal echocardiograms with benign postnatal course and no postnatal echo performed. Four infants had mild abnormalities on prenatal echocardiograms but had normal postnatal echocardiograms and benign clinical courses, giving a total of 17 minor differences note between the pre- and postnatal findings (Table 3 and Fig. 1).
Comparison of prenatal tele-echocardiography with postnatal diagnosis.
Patients with Complex Congenital Heart Disease on Fetal Tele-Echo
DORV, double outlet right ventricle; KCH, Kosair Children's Hospital; KDMC, King's Daughters Medical Center; VSD, ventricular septal defect.
Patients with Minor Abnormalities on Fetal Tele-Echo
PDA, patent ductus arteriosus; PFO, patent foramen ovale.
Our primary goal was to determine whether prenatal tele-echocardiography can adequately identify fetuses with complex CHD, since a prenatal diagnosis affects the recommendations for delivery location and care available at the time of birth. No infant had a new postnatal diagnosis of complex CHD either by echo or clinical course. For our study population, fetal tele-echo was 100% sensitive and 100% specific for identifying complex CHD with 100% positive and negative predictive values.
We further asked whether fetal tele-echocardiography can identify all details of congenital heart defects, including mild defects. With this broadened classification, we identified an additional 17 patients with possible CHD diagnosed by fetal tele-echocardiogram. In this analysis, four patients with a diagnosis of CHD by fetal tele-echo also had CHD by postnatal echo, which includes the two previously mentioned patients with complex CHD. Fifteen patients with abnormal fetal tele-echocardiograms subsequently had either a normal postnatal echocardiogram or negative clinical course. No patient with normal fetal tele-echocardiogram had either an abnormal postnatal echo or clinical course suggestive of significant cardiovascular disease. For our study population, fetal tele-echo had a sensitivity of 100%, specificity of 79%, positive predictive value of 21%, and negative predictive value of 100% for identifying all aspects of CHD, including mild defects. The minor differences between prenatal and postnatal diagnoses in our patient population were felt to be due to limitations in image quality of the fetal tele-echoes.
As shown in Figure 1, two patients had minor CHD diagnosed by fetal tele-echo, but postnatal echocardiograms showed different minor lesions. One of these patients had prenatal diagnosis of ventricular septal defect (VSD) with suspicion for coarctation of the aorta. Postnatal echo showed multiple VSDs and a normal aortic arch. The other patient had suspicion for coarctation of the aorta on fetal tele-echo, but postnatal echo showed a small VSD and a normal aortic arch. Both patients had benign newborn courses without need for intervention or surgery.
The average number of fetal echocardiograms for mother–infant pairs was 1.1. Seven out of 75 mother–infant pairs required follow-up fetal echocardiograms. Four of those were subsequently determined to have normal cardiac anatomy by follow-up fetal tele-echo done at KDMC. One had a follow-up fetal tele-echo done at KDMC which showed a suspicion for a membranous VSD. One infant with complex CHD had follow-up fetal echocardiograms performed by UofL pediatric cardiologists at KCH. The other infant with complex CHD had follow-up fetal echocardiograms done both via tele-echo at KDMC and also by UofL pediatric cardiologists at KCH.
For this patient population, the average length of postnatal follow-up, based on available medical records, was 41.8 days, with a median follow-up of 28 days.
For the two patients with complex CHD identified on initial fetal tele-echo, prenatal counseling was arranged. One family had face-to-face counseling with a pediatric cardiologist in 1 week at the tertiary care center in Louisville. For the other family, a counseling visit was arranged in 2 weeks at a local outreach office in Ashland, based upon family preference. After multidisciplinary consultation and discussion with the families, both the patients with complex CHD identified by fetal tele-echo at KDMC in Ashland chose to deliver at Norton Hospital in Louisville, where the newborns were directly admitted to the NICU in the adjacent KCH. While both fetuses had additional anatomic findings delineated on serial fetal echoes done at the tertiary care center and also on follow-up fetal tele-echoes, the overall counseling regarding the presence of complex CHD, recommendation for delivery at a tertiary care center, and expected need for heart surgery did not change from the initial diagnosis to delivery. Both had newborn echocardiograms done immediately after birth, which confirmed the final prenatal cardiac diagnoses. Both newborns were hemodynamically stable throughout the NICU stay, had successful palliative first-stage cardiac surgeries, and were discharged home in good condition.
Discussion
Fetal tele-echocardiography, performed by local sonographers at a small regional hospital and interpreted by pediatric cardiologists using store-and-forward telemedicine, was able to accurately and efficiently identify patients in our population with complex CHD. In this study, the fetal tele-echo studies performed by local sonographers were of high quality, such that repeat fetal echoes were performed on only a small minority of patients, with an average of 1.1 fetal echo per patient. No cases of complex CHD were missed by fetal tele-echo, and no patient was referred to be delivered at a cardiac center who ultimately would not have required such a high level of care. None of the newborns with normal fetal tele-echocardiograms had evidence of CHD after delivery. This provides reassurance that those infants with normal fetal tele-echocardiograms are at low risk to have significant cardiovascular disease immediately following birth and those identified likely benefited from delivery at a referral center.
Our results are similar to published reports of fetal echocardiograms performed at pediatric cardiac centers. Overall, 23% of our patients had difference between prenatal and postnatal findings, and differences found at pediatric cardiac centers have ranged from 5% to 29%. 22,23
Our analysis differs from the majority of previous studies on fetal tele-echo, in that it compares prenatal findings directly to postnatal diagnoses, including newborn transthoracic echocardiograms, surgical findings, and clinical follow-up. Most previous studies of fetal tele-echo did not assess accuracy of prenatal diagnosis but focused on image quality, 14,17,24,25 interobserver agreement, 26,27 patient and staff comfort, and satisfaction, 28,29 cost, 30,31 and impact on referral patterns. 16 Some studies did look at the accuracy of fetal tele-echo, but either first identified newborns with known CHD and then had a blinded reader review the fetal tele-echo to see if correct anatomic findings could be identified 27,32,33 or used traditional fetal echoes done at a pediatric cardiac center as the gold standard. 14,15 As mentioned above, and highlighted by a recent study from Bensemlali et al. 23 fetal echoes done at a pediatric cardiac center can be discordant from the postnatal diagnoses up to 29% of the time. One study by Hishitani et al. 16 did a partial analysis comparing abnormal fetal tele-echoes to postnatal diagnoses, but there was no reporting of fetal tele-echoes that were read as normal, limiting further analysis. A study by Gomes et al. 34 analyzed 201 fetal tele-echoes and based on review of medical records, “…diagnosis was confirmed in all cases after birth…,” without further details or analysis reported, and so, it is not clear if newborn echocardiograms were performed, what was the length of newborn follow-up, and if there was assessment for minor differences between prenatal findings and postnatal diagnoses.
A potential impact of our study is that it describes a fetal tele-echo model that has been successfully implemented into the day-to-day workflow of a busy clinical practice. In our model, the images are sent via a secure Internet connection using store-and-forward telemedicine. This allows the interpreting physicians at the pediatric cardiac center to optimize workflow and efficiency by reading the scans once all of the images are obtained rather than dedicating longer periods of time to observe the entire scan via live video feed.
Our study has several limitations. In the patient population in this study, we were able to correctly identify all major cardiac lesions and did not have any significant false negatives. We had a relatively small sample size and reasonably expect that in a larger sample size that would not always be the case. Our review of medical records was limited to the hospital at the telemedicine site and our pediatric cardiac center, and so, if an infant had follow-up outside of these systems, we would not know if they had subsequent diagnosis of CHD. To try to ensure that no CHD was missed, studies with suspicion for coarctation or concern for a possible VSD were categorized as abnormal rather than “within known limitations of fetal echo.” Fetuses with these findings accounted for the majority (66%) of the minor discrepancies in our analysis and may not be categorized the same way at other centers.
This model of fetal tele-echocardiography has the potential to benefit families who do not have easy access to a pediatric cardiologist by helping to decrease costs and travel time, improving the rate of prenatal diagnosis of CHD, ensuring appropriate expectant mothers deliver at a pediatric cardiac center, and ultimately improving outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.