
Abstract
Introduction:
This article reviews the intersection of common objectives between telehealth initiatives launched by health systems and community health (specifically community benefit). Telehealth initiatives can benefit communities and play a potential role in improving population health. There is great opportunity to better integrate telehealth activities into community health strategies and community benefit reporting (for nonprofit hospitals) while building the case for telehealth service expansion.
Methods:
Through descriptive, hypothetical cases, we demonstrate the intersection of the triple aim, specifically improving population-level health, and three common objectives between telehealth and community benefit: (1) improving access to care, (2) enhancing community health, and (3) advancing medical or healthcare knowledge.
Conclusions:
This article is intended to spur inspiration for possible telehealth and community health/community benefit connections.
Introduction
Our [healthcare] organizations were established—not for economic opportunity—but to address need for health services in our communities. Our facilities were born out of community need, a tradition that continues today.—Sr. Carol Keehan, DC, President and CEO Catholic Health Association of the United States.
According to the Centers for Disease Control and Prevention, a healthy community is one that is designed and built to improve the quality of life for all people who live, work, worship, learn, and play within their borders where every person is free to make choices amid a variety of healthy, available, accessible, and affordable options. 1 This description highlights the idea that each community has its own distinct community health needs to which local health services should be responsive. As stated by Donald M. Berwick (former Administrator of the Centers for Medicare and Medicaid Services), healthcare transformation “…won't yield to a massive top-down national project.” He explained:
“Successful redesign of healthcare is a community by community task. That's technically correct and it's also morally correct, because in the end each local community–and only each local community–actually has the knowledge and the skills to define what is locally right.” 2
With increasing national attention and financial incentives directed at initiatives that prioritize population health management and other components of the triple aim (i.e., improving the experience of care, improving the health of populations, and reducing per capita costs of healthcare), 3 all hospitals, regardless of tax exemption status, have broadening motivation to participate in activities that improve the health of the communities they serve at large. A specific illustration of this orientation toward a community focus with an emphasis on improving population health is promoted through accountable care organizations (ACOs) and with some states initiating programs such as Washington's accountable community health (ACH) program. These efforts, in which all hospitals within a community may participate, incentivize activities within a community Medicaid Regional Service in response to the assessment of prioritized community health needs. 4 These activities are targeted to promote health equality, local health improvement, and align resources and activities to improve personal health and wellness. Beyond these current broad initiatives and climate, some hospitals and health systems have a long-standing and mandated history of participating in activities that improve the health of the communities they serve at large. Specifically, nonprofit health organizations have a rich history of providing benefit to their communities through activities that are responsive to local need, increase access to care, advance knowledge, and help to relieve government burden.
For 501(c)(3) (tax-exempt nonprofit) hospitals and health systems, the tradition of health organizations providing services and activities to address defined community needs is expressed through community benefit. Community benefit as a strategic and mission-driven concept is adopted by many hospitals and health systems through the provision of care and improvement of community health within a defined area, with preference given to the poor and vulnerable in the community. 5 This tradition of responding to community needs was set into law with 2010 legislation requiring tax-exempt hospitals to work with public health and community members to assess community health needs and develop strategies for addressing those needs. All 501(c)(3) hospitals must report on these assessments, their community benefit activity and other information related to tax exemption to the Internal Revenue Service on Form 990 Schedule H. 6
In keeping with the goals of the triple aim (and more specifically with improving access and population heath that impact all hospitals) and the specific requirements of community benefit for tax-exempt nonprofit hospitals, we propose that health systems, when considering investment in telehealth, also consider (1) the impact of telehealth as an option to improve population health and increase access to care when reach and time to care may be an issue for all hospitals and (2) the concepts and requirements of community benefit and telehealth working synergistically to meet identified needs in the community and help tax-exempt nonprofit hospitals further their mission mandates, especially with the most vulnerable in the community. Specifically, the purpose of our article is to identify and describe the connection between telehealth and community benefit, with additional opportunities for improving population health and access to care for all communities.
Through descriptive hypothetical cases, we demonstrate the intersection of common objectives between telehealth and community benefit, and the common objectives include (1) improving access to care, (2) enhancing community health, and (3) advancing medical or healthcare knowledge. For purposes of this article, we align our reference to telehealth initiatives launched by health systems with the American Telemedicine Association definition of telehealth, which includes the use of medical information exchanged from one site to another through electronic communications to improve patients' health status as well as remote healthcare that does not always involve clinical services. Videoconferencing, transmission of still images, e-health, including patient portals, remote monitoring of vital signs, continuing medical education, and nursing call centers are all considered part of telehealth. 7 We limited the case scenarios to only the common objectives, and not all of the objectives of telehealth or of community benefit. In recognition of the special reporting requirements required for tax-exempt nonprofit hospitals, we suggest application of the tax-exempt nonprofit hospital community benefit reporting requirements, as constituted by the Internal Revenue Service (IRS) to maintain 501(c)(3) nonprofit tax exemption status, in the case scenarios. We ground our cases in representative telehealth literature that (if properly contextualized) may support the common objectives of telehealth and community benefit. To further recognize tax-exempt nonprofit reporting requirements within community benefit, we contextualize our discussion to also demonstrate how community benefit reporting requirements may apply in the case scenarios.
Identifying Common Objectives Between Telehealth and Community Benefit
To be reported as community benefit to demonstrate fulfillment of a hospital's tax-exempt purpose, programs and activities must address documented community health needs and include at least one of the following objectives: improve access to healthcare services; enhance the health of the community; advance medical or healthcare knowledge; and/or relieve or reduce government burden to improve health. 8 Conceptually, telehealth (and more narrowly telemedicine) initiatives share many of the same core objectives as community benefit. Pulling from the telehealth evidence base, we have identified three common points of overlap (Fig. 1) between activities that benefit a community and selected telehealth initiatives: (1) improve access to healthcare, (2) enhance community health, and (3) advance medical or healthcare knowledge. We discuss these common overlaps below as a means to inspire community benefit thought and strategies that include telehealth initiatives (we provide additional details of literature referenced in the body of this article to further showcase these three common objectives in Appendix A–C ).
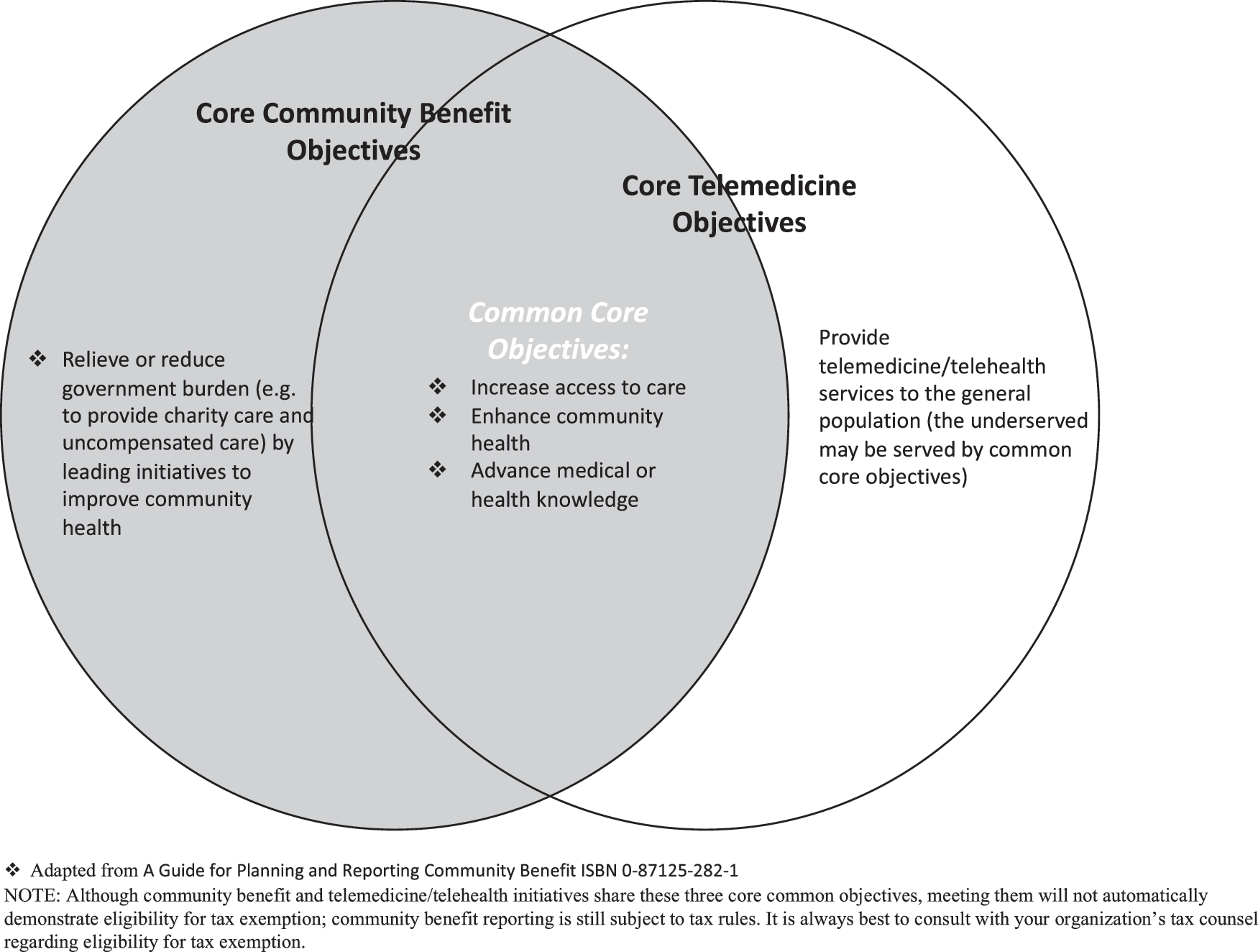
Overlapping common core objectives between community benefit and telemedicine/telehealth initiatives to provide services to vulnerable populations [6].
Common objective 1: improving access to healthcare
Telehealth has a strong track record for improving access to care for vulnerable and underserved populations. Telehealth initiatives, such as virtual visits, telemonitoring, and home telemedicine, are commonly deployed by health organizations to extend the reach of care to patients who face barriers to accessing traditional in-person health services. For example, such initiatives target patients struggling to manage one or more chronic conditions, 9 rural or remote populations with limited access to care facilities and medical professionals, 10 –13 and individuals in need of mental health and substance abuse services, 11 among other vulnerable groups.
Common objective 2: enhancing community health
Whether through education, health promotion, or disease management, the evidence base suggests that telehealth has a positive impact on individual and community health. Mobile health, virtual visits, and telemonitoring programs are often shown to improve self-efficacy and self-care among patients with chronic conditions, increase adherence to treatment regimens and disease management plans, and improve clinical outcomes such as controlled hypertension. 14 –17 In addition, telecoaching interventions targeted at older adults, racial and ethnic minorities, and other vulnerable groups are often used to encourage healthy behaviors related to physical activity and weight reduction, cancer care, and smoking cessation. 18 –22 Combined, these efforts improve overall health at the individual and community levels.
Common objective 3: advancing medical or healthcare knowledge
Telehealth is also utilized to provide education and training to healthcare professionals. Telementoring, teleconsultation, and other virtual programs disseminate knowledge and training to medical professionals in isolated or rural areas in the United States and worldwide related to evidence-based diagnostic and treatment techniques. 23 –26 Relatedly, telehealth is used to provide continuing medical education to providers through the use of virtual lectures and live broadcasts of surgical procedures. 27,28
Community Benefit Reporting: 101
To better understand the benefits of telehealth to improve community health and how that may translate into community benefit reporting by tax-exempt nonprofit health organizations, we must first understand the basics of community benefit requirements.
The reporting mechanism for community benefit and other information related to tax exemption is the Form 990 Schedule H. This form encourages accountability among tax-exempt nonprofit hospitals by asking hospitals to report the cost of their community benefit and other activities. Broadly, Schedule H reporting categories include financial assistance for those without the ability to pay for health services; unpaid costs related to government-sponsored mean-tested healthcare programs; and community benefit services, such as community health improvement services, health professions education, subsidized health services, research, cash and in-kind contributions, community-building activities, and community benefit operations. 8 It is important to note, community-building activities are reported separately on Schedule H and do not factor into the monetary reporting of community benefit. Table 1 provides a description of these categories.
Description of Community Benefit Reporting Categories [8]
Most of what is captured on Schedule H includes dollars spent in various categories. Determining what activities count financially for community benefit can be difficult. However, commonly accepted guidelines and standards for what does and does not count as community benefit, consistent with IRS instructions, are available. A summary of these guidelines is provided in Table 2. In addition to the reporting requirements on Schedule H, tax-exempt nonprofit hospitals are also required to conduct a community health needs assessment (CHNA) and develop an implementation plan based on the identified needs and priorities every three years. 29 This additional requirement may impact what does and does not count for community benefit.
Guidelines for Counting Community Benefit [5]
According to the Catholic Health Association of the United States, telehealth activities may be reported as community benefit as long as the activity meets the definition of community benefit. 30 By leveraging the mutual objectives of telehealth and community benefit, the costs associated with providing certain telehealth services may be captured through community benefit on Schedule H for tax-exempt nonprofit hospitals. While reporting telehealth as community benefit is not a direct capture of revenue, it is an investment in the community. Part of the organizational consideration should be how vulnerable populations may benefit from these services. Fortifying the health of vulnerable populations and communities may lead to improvements in population health. The hypothetical cases described below offer examples of how telehealth and community benefit share important objectives and potential community benefit reporting relevance.
Hypothetical Cases
The following use cases offer examples of how telehealth services delivered by tax-exempt nonprofit hospitals of varying size, location, and target patient population may be reported as community benefit. For each, we provide a case overview, identify specific Schedule H community benefit categories as applicable (reviewed in Table 3), provide a case description, and conclude by tying telehealth and community benefit efforts back to their mutual objectives of increasing access to care, advancing knowledge, and improving community health. These hypothetical cases are not meant to substitute for legal or accounting advice, but rather to demonstrate conceptual links and potential application. As is always recommended, organizations should first seek the counsel of their own organization to determine reporting relevance for tax purposes.
Potential Categories of Community Benefit Reporting for Telehealth Use Cases
Case 1
Case overview
Hospital A uses telehealth to expand access to care coordination services to vulnerable older adults in the community. As a result of Hospital A's partnership with a local federally qualified health center (FQHC), Hospital A will expand access to telemonitoring through the FQHC for all low-income older adults and other vulnerable persons in the defined community who have been discharged from any hospital in the area.
Case description
Hospital A is located in a large metropolitan area and has a disproportionally high pay or case mix of Medicaid and uninsured individuals. A portion of their defined community, as reported in Form 990 Schedule H and in their required CHNA, includes many zip codes that constitute an impoverished part of the urban core, with higher rates of poverty and higher concentrations of older adults (with long-standing resident status) compared with state averages. Many of the older adult residents in these zip codes rely on local FQHCs as their primary source of care. FQHCs are the safety net providers for all members of the community, regardless of the ability to pay. Through their own community health assessment process, these FQHCs recognize the need to better monitor the health of older adults in their service area: older residents have worsening functional and medical status, one or more diagnosed chronic conditions, and high rates of hospitalization. Hospital A has established relationships with FQHCs in these zip codes through a residency program.
Hospital A is considering expansion of their current telehealth capabilities to include additional telemonitoring in the home for older adults following hospital discharge to improve general health and reduce avoidable hospital readmission and emergency department visits. While Hospital A already provides telemonitoring for certain patients following discharge, local FQHCs propose a partnership to extend the reach of this service to all older adults in high need zip codes as identified on Schedule H and in the CHNA. Hospital A and FQHCs are also considering partnership with the Area Agency on Aging in this endeavor to assess the patients' home environment and provide a link to social services to address other areas of need.
Connecting telehealth and community benefit
This case links telehealth and community benefit through the mutual objective of increasing access to care. As per CHNA reporting, much of Hospital A's defined community constitutes an impoverished part of the urban core, with a disproportionately high case mix of Medicaid, uninsured, and older adults. As a result of Hospital A's partnership with local FQHCs, it will expand access to telemonitoring for all vulnerable older adults in the defined community who have been recently discharged from the hospital, regardless of patient affiliation. If Hospital A receives Medicaid reimbursement revenue for these services, the difference between a lower reimbursement and actual costs may count as community benefit. In addition, costs associated with providing the expanded telehealth services to Medicaid beneficiaries and other low-income patients, if beyond the hospital's routine discharge planning and follow-up policies, may count as community benefit.
Case 2
Case overview
Hospital B uses telehealth to provide education and training to providers and community members regarding chronic hepatitis C virus.
Case description
Hospital B is located in a mid-sized metropolitan area. A portion of their defined community, as reported in Form 990 Schedule H and in their required CHNA, includes several rural health counties that are medically underserved and experience higher rates of poverty compared with peer communities across the state. Rates of chronic hepatitis C virus (HCV) are also higher in these counties compared with state averages.
Hospital B is a part of Excellence Health System (EHS), which endeavors to promote clinical excellence and professional development through evidence-based and innovative learning approaches. As part of a strategic initiative to reach underserved rural areas of the state, EHS aims to provide educational offerings throughout the year to all physicians and healthcare professionals in the community, especially those located in rural health centers and other geographically isolated provider organizations, regardless of institutional affiliation. The telehealth department of Hospital B has videoconferencing equipment that allows the telehealth technology specialist to record educational offerings on the video bridge's content server. To address the high rates of HCV in these rural counties, professional development and trainings designed for rural practitioners are provided monthly, with an emphasis on hepatology. Hospital B and EHS then partner with state academic institutions, local health departments, and rural health centers to deliver the health professional education.
In addition to educating healthcare professionals, Hospital B hosts a TeleHepatology-ECHO program that offers preventive educational programming for all residents in the defined community living with HCV, regardless of patient affiliation with Hospital B. The ECHO program provides around-the-clock access to consumer training videos to improve the long-term health and wellness of individuals living with HCV and their family members. Examples of video topics include nutrition/diet, physical fitness, spirituality, psychosocial adjustment, resiliency, community resources, and medication compliance.
Connecting telehealth and community benefit
This case connects telehealth and community benefit through the mutual objectives of advancing medical and health knowledge and improving population health. As per CHNA reporting, Hospital B identified a need for professional development services for area medical professionals and community-based education for residents living with HCV. Initially limited to their own providers and patients, these telehealth educational and training services were expanded to all providers and HCV patients located in high need rural areas of the defined community, regardless of affiliation with Hospital B. To the extent that the education program can be considered continuing education required for licensure or certification, the costs can be reported as health profession education. In addition, associated service and technology costs may count as community benefit if not part of the cost of doing business. If the hospital can demonstrate and disseminate that telehealth is improving health and decreasing cost, then those costs may also count as community health improvement and the overall telehealth program must be subsidized.
Case 3
Case overview
Hospital C uses telehealth to improve healthy nutrition and prevent childhood obesity.
Case description
Hospital C is a smaller community hospital located in a fairly rural county in a southern state with some of the highest childhood obesity rates in the country. Through their required CHNA, and in collaboration with the local health departments in a three-county area, Hospital C has identified childhood obesity prevention as one of the top health priorities in its core service area.
There are many challenges and barriers regarding obesity prevention in children for this region. A high percentage of the children are eligible for free or reduced school lunch programs, and during the school year, a high percentage of children receive two meals through the school systems. In addition, school budgets and state accreditation pressures for the approximately six school districts in the region mean that more academic seat time and less physical education are occurring.
Hospital C, in collaboration with the three local health departments, wants to bring a free obesity prevention and physical activity program through telehealth to the schools located within the six school districts. Working in conjunction with the school administration and school nurses, Hospital C will provide the telehealth technology to provide health education and healthcare expertise to all students and staff in participating schools. All students will have the opportunity to participate, with enhanced services provided to students identified as high risk by the school nurse, following best practices for obesity prevention. School nurses and healthcare experts at Hospital C will work with the children and their families to connect and communicate with their primary care providers or health clinic.
Connecting telehealth and community benefit
This case connects telehealth and community benefit through the mutual objective of improving community health. Hospital C is using telehealth services to provide school-based obesity prevention to all children, particularly those at high risk for obesity, free of charge. Students are not expected to be patients of Hospital C to receive these services. Hospital C does not benefit more from this effort than the community; as a result, costs associated with healthcare expert services may be counted as community benefit. In addition, the cost to provide the technology to the schools may also count as community benefit.
Conclusions
This article reviews the intersection of common objectives between telehealth and community benefit. In addition, there is demonstrated impact that all hospitals, regardless of tax-exempt status, should consider. Through descriptive hypothetical cases, we demonstrated the intersection of three common objectives between telehealth and community benefit, including improving access to care, enhancing community health, and advancing medical or healthcare knowledge. Furthermore, we explain how the various aspects of IRS community benefit reporting requirements may apply in case scenarios. As revealed by the use cases reviewed, some aspects of telehealth initiatives may align with community benefit reporting guidelines. Therefore, tax-exempt, nonprofit hospitals should take full advantage of the inherent linkages between telehealth and community benefit.
Better aligning of telehealth investments and initiatives with community benefit concepts, goals, and reporting requirements presents great opportunity for health organizations to invest in efforts to improve the health of the community, especially vulnerable populations previously difficult to reach. In addition, all hospitals should consider telehealth as a means to achieving the goals of the triple aim. In the future, the reporting of telehealth best practices to positively impact communities by all hospitals will be important to encourage other organizations to pursue similar strategies and continue to build the evidence base around telehealth, improved population health, and increased access to care linkages.
Reimbursement is so often the mechanism of interest in efforts to strengthen the business case for telehealth initiatives. We argue here that health organizations and others in the telehealth community should think more broadly in their attempts to enhance the case for investment. We have focused on describing how investing in telehealth for community benefit has many positive potential impacts for communities and for the nonprofit hospitals. We also recognize that increasingly, policy and programs are sending the message that hospitals and communities in which they reside, may achieve positive impact when the important goals of the triple aim (improving quality, improving population health, and reducing costs) are realized. Investing more broadly in telehealth to meet the goals of the triple aim may also impact communities.
Footnotes
Acknowledgments
The authors thank the American Telemedicine Association's (ATA) Business and Finance Special Interest Group (SIG) for putting this topic on their agenda in the 2015 ATA conference business course. The authors thank participants for their important questions, which helped to guide the development of this article.
Disclosure Statement
No competing financial interests exist.
Representative Evidence Supporting Linkage Between Telehealth and Advancing Medical or Healthcare Knowledge
| CITATION | TELEHEALTH/TELEMEDICINE SERVICE | TARGET POPULATION | POTENTIAL WAYS SERVICE BENEFITS COMMUNITY | DESCRIPTION |
|---|---|---|---|---|
| Hipple et al. (2013) | Web- and telephone-based distance training to support practice change related to tobacco control | Pediatricians practicing in low-income health clinics | Education on harmful effects of SHS on children, training on how to broach topic/address issues w/family members | Randomized control study comparing the effect of distance learning with a control group to improve provider–patient interaction related to tobacco control practices. |
| Distance training significantly improved rates of clinicians asking about parental smoking (and other smoking household members) as well as smoke-free rules in the home compared with the control group. | ||||
| Findings suggest that distance learning interventions can improve training outcomes for pediatricians in low-income clinics related to tobacco control. | ||||
| Antoniou et al. (2012) | Telementoring for laparoscopic surgery | Health professionals in geographically isolated general practices | Further dissemination of clinical mentoring for minimally invasive surgical techniques in isolated areas | Systematic review of the evidence-based literature on clinical telementoring applications in laparoscopic general surgery. |
| Completion of remotely assisted procedures was feasible in many of the cases identified in the systematic review. | ||||
| Findings suggest that telementoring programs for laparoscopic general surgery are feasible and safe in remote areas; however, their clinical effectiveness as teaching alternatives to traditional mentoring programs has not yet been evaluated. | ||||
| Mahadevan et al. (2012) | Telemedicine for postgraduate training related to anesthesia and critical care | Medical postgraduates undergoing training for anesthesia and critical care in India | Advance medical knowledge to medical professionals provided to those that may be challenged by geographic isolation and socioeconomic status of low- and middle-income countries | Observational study to examine the feasibility, advantages, and disadvantages of telemedicine learning sessions (organized two times a week between two teaching hospitals). |
| Findings suggest that telemedicine was effective in establishing communication between patients and physicians, as well as teachers and students, improving participant satisfaction, reducing infrastructure difficulties, and improving overall program outcomes in the low-resource study setting. | ||||
| Bediang et al. (2011) | Virtual Internet Patient Simulator (VIPS) as a tool for continuous medical education and decision support | Isolated health professionals in sub-Saharan Africa | Further dissemination of continued education and new diagnostic techniques to isolated rural areas in low- and middle-income countries | VIPS used to develop interactive clinical vignettes to be used by care professionals and students, taking into account clinical problem situations and contexts relevant to the target population. |
| Findings suggest that target population found VIPS to be usable and relevant and can be used to provide initial and continuing medical education in sub-Saharan Africa. | ||||
| Latifi et al. (2011) | Continuous Medical Education through telemedicine | Medical systems in Kosovo and other low- and middle-income countries | Advance education and medical or healthcare knowledge for health professionals in isolated and under-resources health systems in low- and middle-income countries | Cost–benefit analysis study to determine the cost benefit of telemedicine for continuous medical education compared with alternative methods of delivery in low- and middle-income countries over a 5-year period. |
| Telemedicine (including videoconferencing, broadcasting live surgeries, providing virtual lectures, and seminars) found to be a more efficient mechanism compared with alternative methods in ensuring continuous medical education and rebuilding medical systems among the target population. | ||||
| Burg et al. (2009) | Teledermatology | Dermatologists | Advancing continuing medical education and knowledge sharing in low- and middle-income countries | Reviews the current peer-reviewed evidence-based data related to the status of teledermatology as a tool to promote continuing medical education and share medical knowledge postgraduation. |
| Findings suggest that teledermatology is a user-friendly platform with a high potential for training medical professionals in low- and middle-income countries. | ||||
| Augestad and Lindsetmo (2009) | Tele-education for surgeons through videoconferencing | Surgeons in remote areas | Advancing access to medical knowledge in the surgical field for remote areas | Reviews the current peer-reviewed evidence-based data related to the use of videoconferencing as a clinical tool among surgeons. |
| Findings suggest that videoconferencing is widely and effectively used as a tool for surgeons to share medical knowledge and mentor clinical peers across a variety of contexts, included but not limited to emergency services, surgical telementoring, and postoperative follow-up care |
This table illustrates examples of common objectives related to advancing medical or healthcare knowledge; inclusion of a telehealth initiative in this table does not assert that the described telehealth activities align with all of the provisions related to tax exemption and reporting to Internal Revenue Service on Form 990 Schedule H [6].