
Abstract
Background:
In Brazil, the Program for Institutional Development of the Unified Healthcare System (PROADI-SUS) has implemented a telemedicine service for urgent situations and emergencies. It is delivered by a high-technology (HT) hospital to 15 remote healthcare units (RUs) in 11 different Brazilian states. The aim of this study was to investigate possible barriers and benefits in telemedicine service among these units.
Materials and Methods:
We performed a qualitative study on the perceptions of physicians involved in telemedicine service in their role as providers and consultants. An individual, semistructured recorded interview was conducted with 28 physicians (17 HT; 11 RU) encompassing telemedicine resources and interaction among HT and RU physicians. Data analysis was performed by Discourse of Collective Subject.
Results:
We identified the following barriers in the telemedicine service: (1) lack of experience in the use of technology or the quality of the internet signal; (2) the multiplicity of different telemedicine platforms; (3) the quality of the image sent to the HT hospital; (4) the misunderstanding that telemedicine is a time-consuming technology instead of a resource that may help to save lives; (5) not feeling comfortable exposing doubts to other HT colleagues; (6) problems in the management of telemedicine use in the RUs; and (7) political and legal issues. However, important benefits in telemedicine service were also described.
Conclusions:
The structural barriers should be the target of hospital managers. Development of standard remote care protocols may increase the use of telemedicine and create new work routines. Given the relationship difficulties among the RU and HT doctors during telemedicine consultations, other meetings should be organized to allow more interpersonal interactions. These meetings may also have the goal of sharing outcome indicators of their joint activity in telemedicine to stimulate and make them aware of the benefits of their interaction.
Introduction
Since the 1970s, there has been a growing interest in telemedicine systems. The main characteristics of a telemedicine system are (1) the geographic distance between the provider and the client during the clinical meeting (telediagnosis) or between two or more providers during a consultation (teleconsulting); (2) the use of telecommunication (computational technology) to allow or facilitate the interaction among providers and clients or consultants as well as to exchange information; (3) an information technology infrastructure and appropriate staff to perform the necessary tasks between the linked units; (4) the development of clinical protocols for diagnoses and treatments; and (5) the development of normal patterns of behavior to substitute the face-to-face contact among clients/consultants and providers. Telemedicine is considered a technological tool with the potential to improve healthcare systems. 1 Nevertheless, several obstacles can influence its adoption to reach improved patient's outcomes, expanded access, and increased efficiency of health services.
The fast development of telecommunication and information technology has provided a solid foundation for telemedicine. The service provided by telemedicine can be as effective as a personal consultation. 2 In a modern definition, some authors suggest that telemedicine is part of the field of e-health, which applies a network communication to deliver health services and medical education between two distant locations. 3
In the case of disasters or geographic isolation, it is frequently impossible to wait for the physical presence of a medical team. Telemedicine can be the only way to allow fast first aid. 4 Telemedicine may reduce hospital costs and convalescence time because the patient may be able to recover at home. 5
To improve the success of a telemedicine program, it is important to bridge the gap between medical services (such as teleradiology for hospitals in rural regions) so that urgent services (e.g., strokes) can be covered and between different centers providing video chats so that specialists can help primary care professionals. 6
In a report published by the World Health Organization, the most frequent barrier to telemedicine implementation was the perception that it is too expensive. This is true for some of them; however, others can be implemented using pre-existing infrastructure. In developing countries, underdeveloped infrastructure was a common barrier to telemedicine development. Another possible barrier yet to overcome is that some patients and healthcare workers resist adopting service models that differ from traditional approaches or practices, while others lack computer literacy to apply telemedicine approaches effectively. 7
Potential benefits of telemedicine are increased access to professional expertise in remote and rural settings and cost savings. However, several limitations and barriers to the application of telemedicine are evident, including overdiagnosis, dependence on a functional telecommunication system, and legal aspects. 8
To overcome consultation barriers at small rural hospitals, a telegeriatric service model was implemented involving a geriatrician remotely using wireless, mobile high-definition videoconferencing; a trained nurse in the rural area; structured geriatric assessment configured on a Web-based clinical decision support system; and support from a local multidisciplinary team, showing that a telemedicine model is feasible with training, adequate equipment, and logistics. 9
In Brazil, the Program for Institutional Development of the Unified Healthcare System (PROADI-SUS) has implemented the telemedicine service for urgent situations and emergencies delivered by a high-technology (HT) hospital to 15 remote healthcare units (RUs) in 11 different Brazilian states. Throughout this system, physicians from the RUs can discuss medical cases with specialists from the HT hospital, where a second opinion can be important to investigate possible improvements in diagnosis or treatment. Resources in the RUs can be limited due to lack of medicine and equipment to assist patients.
This study may contribute to an increased understanding of the complex relationships between governmental institutions (SUS and remote healthcare units) and a private hospital, which delivers the telemedicine service to the latter. This investigation is a result of examining the telemedicine database from the HT hospital, which indicates that only 1,627 calls from the 15 RUs were made in 3 years.
The aim of this study was to investigate possible barriers and benefits in telemedicine service from an HT hospital to remote public healthcare units that are part of the SUS. Therefore, this study is relevant in the fields of clinical practice, public health, and policy.
Materials and Methods
The protocol was approved by the Ethics Committee of Hospital Israelita Albert Einstein (No. 138662714.0.0000.0071). The anonymity and confidentiality of the participants were ensured.
Participants
After signing an informed consent, 17 HT physicians were interviewed in loco, and 11 RU professionals were interviewed by telemedicine (Fig. 1). In all cases, the principal investigator of this study, who is not involved in telemedicine service to avoid bias, conducted the semistructured interviews. The professionals from the HT hospital were personally invited to participate in the study and those from RU were invited by e-mail. All professionals who were willing to contribute and available for a 1-h interview were included.
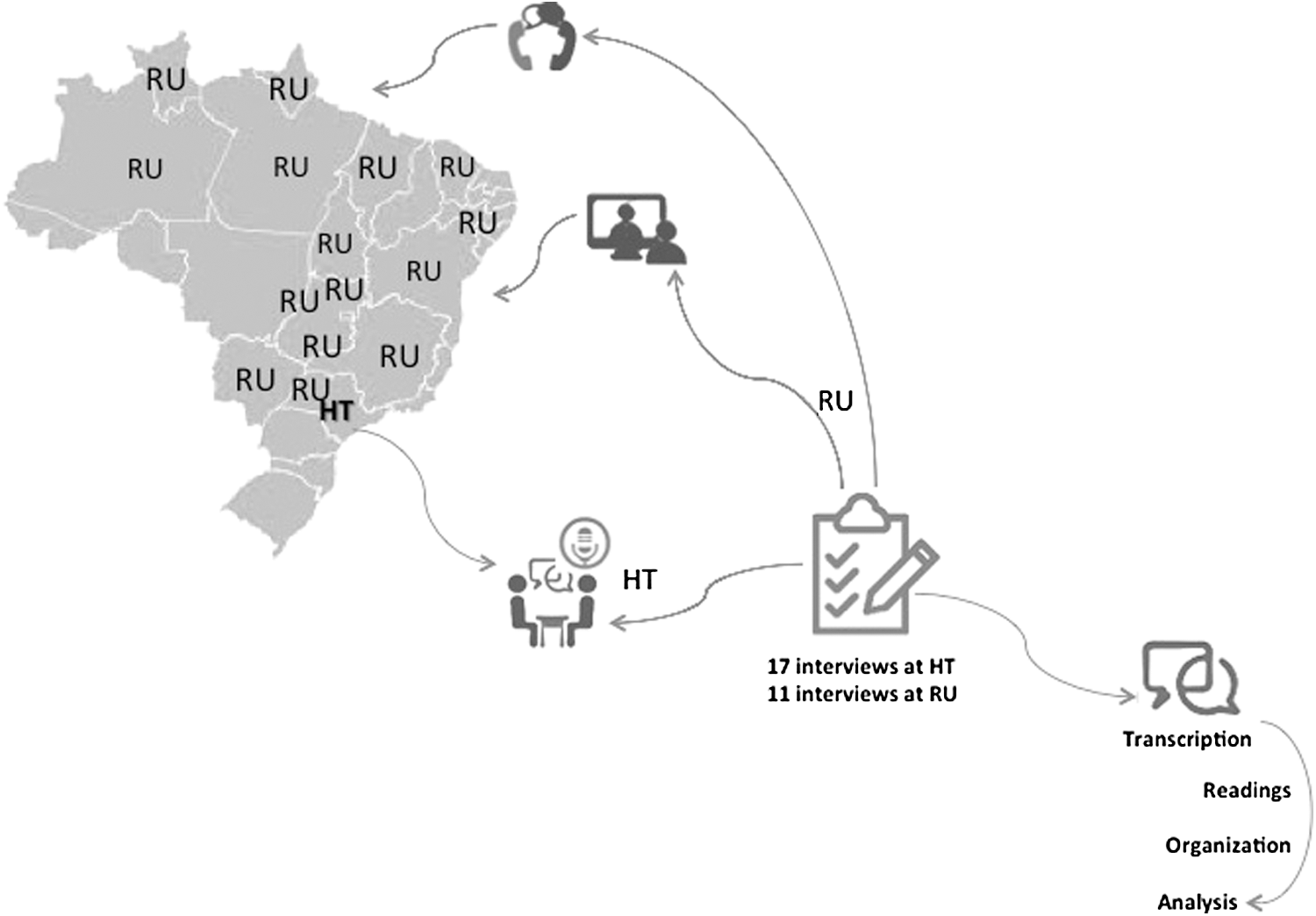
The HT hospital and RU locations in Brazil. HT, high-technology; RUs, remote healthcare units.
Data Collection
Individual semistructured interviews of the professionals involved in telemedicine were recorded to investigate the experience of using telemedicine resources: (1) What has been your experience in telemedicine? Have you identified any barrier or difficulty? (2) What has been your experience interacting with other physicians by telemedicine? (3) Have you identified any benefit from the telemedicine service?
Individual interviews were chosen to allow the participants to describe their experiences and perceptions in detail and because it would be difficult to organize focus groups with the RU professionals. Data collection was stopped after all the volunteer participants in the research were interviewed.
Data Analysis
The qualitative data analysis comprised four steps: (1) full transcriptions of recorded interviews; (2) systematic and targeted readings to identify the key ideas to identify the essence of individual discourses (literal transcription of their declaration); (3) categorization of these key ideas; and (4) reconstruction of individual discourses into synthesized discourses in necessary numbers to express the social representation about the studied phenomena, which is characterized in the Discourse of the Collective Subject (DCS). 10 The principal investigator was responsible for transcription of the interviews. Three researchers who are not working in telemedicine consultations (to avoid bias) contributed to build the DCS. Disagreements during this process were discussed and handled during research meetings.
The Qualitative Research Review Guidelines—RATS—were consulted for preparation of this article. 11
Results
We identified the following central ideas related to three themes, according to the following methods: different types of barriers, difficulties in personal interaction, and benefits in telemedicine service.
Technological and Structural Barriers
DCS 1 from the RU
Most of the identified barriers are technological/technical barriers. Lack of experience using the technology or the quality of the Internet signal. Sometimes technology helps the consultation; sometimes it is a delay because we must wait for technical help to conclude the consultation and to include all necessary data being sent to the HT hospital.
It is also important that the structure of the telemedicine must be ready to use as soon as the patient arrives at the hospital. For example, sometimes the telemedicine service is requested afterward, when the patient is already in the Intensive Care Unit or Infirmary. However, when the call starts in the Emergency Room and we are called to help a new patient, we must hang up the call.
DCS 1 from the HT hospital
The main barrier is multiplicity of different telemedicine platforms and problems with the Internet, such as speed and quality. For example, the RU physician asks to discuss several cases from different patients during the same interview, which is not the ideal way to collect and register all the necessary information in our database.
Even so, when the Internet is not working properly, we continue assisting the RU using WhatsApp or telephone. I feel that the RU professionals have difficulties with the telemedicine equipment and must be motivated to overcome them. The RU does not always have all the examinations and procedures we need for an ideal diagnosis and treatment. The quality of the image examinations that we have received is not always adequate. Therefore, I have some questions about the quality and precision of the information the RU physician collects from the patient and the lack of a satisfactory clinical description; many times we depend on the references about the patient, which come from the RU because we are not able to do the clinical anamnesis in cases where the patient is not able to be transported to where the telemedicine equipment is located.
Other Barriers Described only by The HT Physicians: RU Management, Political Issues, Legal Issues, and Medical Training
DCS 2 from the HT hospital
The RUs should request more telemedicine consultations. I believe that the RU coordinator must be involved in monitoring the physicians' access to the telemedicine, motivating and instigating them to use the telemedicine consultations. It is important to create a new culture for technology use. One of the RUs is directly managed by the HT hospital and this hospital is more involved in telemedicine consultations.
DCS 3 from the HT hospital
Most RUs were selected by the Ministry of Health to receive the telemedicine equipment instead of requesting them individually. It is important to investigate the motivation of these RUs in the process of acquiring this technology. The Ministry should at least monitor the use of telemedicine by these units.
DCS 4 from the HT hospital
In Brazil, there are discussions about legal issues of telemedicine consultation. This is something relatively new and we are increasingly trying to help to consolidate the legal issues.
DCS 5 from the HT hospital
There is a huge difference in the medical training among medical schools in Brazil. Therefore, sometimes it is difficult for the RU physician to understand our requests, our questions, and I feel that they are not comfortable asking questions of colleagues from an HT hospital. However, the telemedicine service could be an instrument to decrease these gaps in medical training.
Interpersonal Relationship Difficulties
DCS 2 from the RU
I believe that it is important that my colleagues get more involved and motivated in using the telemedicine resources. We can learn a lot by talking to the HT specialists. It is important for our patients. However, I feel that some colleagues are inhibited with the idea of consulting or asking a specialist from the HT hospital and feeling unprepared to answer some questions from the HT specialist. It is about feeling ashamed of their own lack of knowledge, which is a mistake! We must take the opportunity to learn! On the other hand, the HT physician is not always available at the moment when he or she is needed, especially for highly complex interventions. I also felt that not all HT physicians have the patience to understand our difficulties here.
DCS 6 from the HT hospital
An important barrier, I felt, is that the RU physician is frequently a novice and he/she is not really aware of the importance of the quality of the consultation, as opposed to the quantity, even considering the lack of resources in the Brazilian public health system. There are many patients requesting assistance in the public health system and the novices see telemedicine as a time-consuming technology instead of a resource that may help to save lives and the opportunity to learn from the HT specialist. As a physician, I must know everything—this is the idea that a medical student must have about his/her profession. Without this attitude, as a physician, you will not feel comfortable about exposing your doubts to the HT colleague.
Benefits of Telemedicine
DCS 3 from the RU
The patient's care is certainly improved. In all cases, the treatment improved with telemedicine consultation, especially in the most complex cases, such as neurological diseases. Should I send the patient to another hospital or not? The HT physician helped me to decide the best procedure for the patient.
DCS 7 from the HT hospital
From this side of the screen, I could perceive that sometimes the RU physician was in doubt about the best procedure. Sometimes the RU physician is not experienced enough to know how to deal with the patient at the intensive care unit. In one of the RUs, I heard that we helped to decrease mortality in an ICU! That is huge!
Discussion
Some barriers for the implementation of telemedicine are development of financial support and mechanisms to reimburse consultations; to get the technical equipment where providers and clients are; training to optimize the audio and video resources, and clear policies for procedures and services by telemedicine. 12 –14 In addition, other problems can be irregular bandwidth, poor network coverage, and unstable power supply obstructing interactivity and access to information. 15 Both the physicians from the HT hospital and the RUs identified some of these problems when they talked about technological barriers: the low quality of the internet signal; the multiplicity of different telemedicine platforms; and the quality of the image sent to the HT hospital. The RU professionals have some difficulties with the telemedicine equipment and some RUs chosen do not appear to be motivated to use this resource.
Another barrier in telemedicine is the acceptance of the telemedicine service by the staff because of the negative impact related to change in the service, credibility and autonomy, patient–staff interaction, and technical questions. Problems in communication among healthcare teams are barriers for the acceptance of telemedicine. 16 It is also important to take care of the verbal and nonverbal communication among the participants. 17 The RU physicians are impacted by the inhibition of communication related to RU physicians in situations in which they can be questioned by a specialist from the HT hospital, triggering feelings of shame. The HT physicians perceive that the physician from the RU is frequently a novice and he/she is not really aware of the importance of the quality of consultation, as opposed to the quantity. There are many patients requesting assistance in the public health system and the novices see telemedicine as a time-consuming technology instead of a resource that may help save lives. Consistent standards to guide development of telemedicine/telehealth clinical guidelines and protocols, such as the definition of a physician–patient encounter and the ability for nurses and other licensed practitioners to provide telemedicine/telehealth services, have been implemented to facilitate the use of telemedicine to develop a multidisciplinary approach. 18
Telemedicine services should be integrated into healthcare systems. 19,20 Implementation of telemedicine services depends on a positive link with a policy-level sponsor. 21
In this study, we are investigating a telemedicine service delivered from a private HT hospital to public RU integrated by the SUS from Brazil. The HT hospital is a philanthropic institution, which receives financial support from the Ministry of Health to deliver this service.
There are two factors that summarize the telemedicine success: (1) training and (2) education. It is also important to evaluate how the entire system works in conjunction with the users. 22 As noticed in our results, when the physicians talk about technological barriers, it is clear that most of these problems may be attributed to the lack of interest or understanding about the importance of telemedicine technology in helping patients with complex diagnosis or when a second opinion is important for the treatment. Financial support for continued training and education, which could be offered to telemedicine, may help overcome these barriers.
Improved management intervention at the RUs where telemedicine has been introduced is necessary to maintain high performance and continuity. For this matter, the management's lack of efficiency seems to be related to how the RUs are chosen. Criteria for selection of units that will receive the service should also be developed in search of greater engagement and results management.
As for the legal issues, the uncertainty shown by the physicians interviewed calls for a national telemedicine program strategy to ensure that the users, physicians, and patients have a more comprehensive environment and secure framework in which a given health professional can perform his/her duties. 7
Telemedicine may improve the quality of care and reduce patient readmissions. 23,24 This is particularly important in a country of continental dimensions such as Brazil, where this kind of technology has allowed direct and simultaneous contact with advanced centers in health; improved guidance support before life-threatening situations; improved the solvability of secondary care; and provided access to experts to whom the population would not otherwise have access. 25
In this study, patients from the RUs benefited from telemedicine communication among the physicians from the RUs and the HT hospital. Telemedicine is helping the RU physicians to make better decisions and improve the quality of care.
Conclusions
Although many barriers have been described, the benefits for RU patients are motivating the search for solutions. The structural barriers mentioned should be the target of hospital managers. Development of standard remote care protocols may increase the use of telemedicine and create new work routines. Given the relationship difficulties among the RU and HT doctors during the telemedicine consultations, other meetings should be organized to allow more interpersonal interactions. These meetings may also have the goal of sharing outcome indicators of their joint activity in telemedicine to stimulate and make them aware of the benefits of their interaction.
Footnotes
Acknowledgments
The authors thank Instituto Israelita de Ensino e Pesquisa Albert Einstein and the Innovation Department of Hospital Israelita Albert Einstein for the financial support.
Disclosure Statement
No competing financial interests exist.