
Abstract
Background:
One area where telemedicine may prove to be highly effective is in providing medical care to the geriatric population, an age group predicted to account for 20% of the population in the near future. However, even though telemedicine has certain advantages, the usability of these systems with this population merits investigation.
Materials and Methods:
This article reviews the literature published from 2000 to 2016 with the goal of analyzing the characteristics of usability-related studies conducted using geriatric participants and the subsequent usability challenges identified. Articles were found using Web of Knowledge and PubMed citation indexing portals using the keywords (1) Telemedicine* AND Geriatrics* (2) Telemedicine* AND Usability* (3) Telemedicine* AND Usability* AND Older Adults*.
Results:
A total of 297 articles were obtained from the initial search. After further detailed screening, 16 articles were selected for review based on the inclusion criteria. Of these, 60% of the studies focused on the overall usability of telemedicine systems; 6.25% focused on the usability of a telepresence robot; 12.5% compared a face-to-face medical consultation with the use of telemedicine systems, and 25% focused on the study of other aspects of telemedicine in addition to its usability. Findings reported in the studies included high patient satisfaction with telemedicine in 31.25%, whereas another 31.25% indicated a high acceptance of this method of medical consultation. Care coordination in 6.25% of the studies; confidence in telemedicine in 6.25%; trust, privacy, and reliability in 6.25%; and increased convenience when compared to personal visits in 18.75% were also reported.
Conclusions:
This review suggests limited research providing scientifically valid and reproducible usability evaluation at various stages of telemedicine system development. Telemedicine system designers need to consider the age-related issues in cognition, perception, and behavior of geriatric patients while designing telemedicine applications. Future directions for research were developed based on the limitations as well as other results found in this systematic review.
Introduction
Telemedicine, which is the exchange of medical information between locations through the use of electronic communication devices, is primarily used to improve healthcare services. 1 Its most significant feature, its dependence on communication technology, allows it to function as a surrogate to in-person meetings, 1 thus providing diagnosis, pretreatment and/or posttreatment to medical issues comparable to the conventional face-to-face method of medical practice. 2 The first reference to telemedicine, although primitive, was made in 1897 in a magazine article reporting the use of a telephone in a home setting in lieu of personal visits to the doctor. 3 Another early application of telemedicine was seen during NASA's first manned space mission when vital signs were collected regularly from the astronauts to address concerns of ground-based physicians regarding the effects of the absence of gravity on the human body. 1 Today, patients use laptops, tablets, smartphones, and other such telecommunication devices 4 for private real-time consultations with healthcare providers at distant hospitals and clinics concerning medical and pharmaceutical information. 3,5 –7
One area where telemedicine may prove to be highly effective is in providing medical care to the elderly, 8 an age group that may soon account for 20% of the population; however, little research has focused on how effective care can be delivered to this population. 9 Studies indicate that 92% of elderly are affected by at least one chronic health issue and in some cases two. In addition, they experience reduced mental ability due to dementia 8 as well as reduced motor capabilities especially in fine motor coordination. 10 Deteriorating health combined with poor motor skills, waiting in line at clinics and hospitals to be assessed by a doctor, or travelling long distances to a healthcare unit, thus, become arduous. One potential advantage of telemedicine is that it eliminates the travel necessary for more conventional treatment, travel that is expensive both in terms of personnel and finances. 8 In addition, there is also a shortage of medical staff to handle the issues of the older population, 11 a situation compounded in rural areas by the cost of employing a full-time geriatrician, which may be impractical because of the reduced caseload. 12 These issues related to the healthcare of the elderly may be addressed by telemedicine.
The research conducted investigating the application of telemedicine to geriatric medical issues suggests it can be applied in various ways, including providing long-term care for chronic diseases, medical access to the elderly in the comfort of their homes, monitoring of vital signs and behavior, and increased access to physicians and other healthcare professionals in nursing homes. 8 More importantly, the medical advice provided through telemedicine has been found to be of good quality, resulting in improved patient satisfaction. 13 In addition, the use of telephone consultation and video conferencing in geriatrics has been found to be cost effective.
Even though telemedicine has advantages, the usability of these systems with the geriatric population requires investigation. While the technology implemented is readily available and widely used, the geriatric population may not be as able to navigate and use it as well as the younger generations. For example, understanding technology-related commands provided by a healthcare professional during a session may be problematic to users with minimal experience and familiarity with technology. Furthermore, the usability of telemedicine by the older population may also be affected by health-related issues, especially because system designers usually do not consider this age group to be potential users, and, therefore, focus little attention on the problems faced by them. 14 However, the overall usability of telemedicine systems is important in creating a positive attitude toward the use of technology in general and in the increased adoption of these systems specifically. 15
This article investigates the areas of usability that have been studied in the geriatric telemedicine setting. More specifically, it reviews articles with the goal of understanding (1) the characteristics of usability-related studies conducted with the geriatric population, (2) the aspects of usability explored in these articles and the instruments used to measure them, (3) the data analysis methods used, (4) the impact of the usability of geriatric telemedicine technology on the geriatric user population, (5) usability challenges associated with telemedicine platforms, and (6) the limitations observed.
Materials and Methods
Institutional Review and Human Subject Determination
This study was exempted from approval by the Clemson University's Institutional Review Board since it did not involve active human subject research. No individual patients participated in this study.
Inclusion and Exclusion Criteria
Only articles investigating usability factors in terms of telemedicine and geriatrics published in peer-reviewed publications between the years 2000 and July 2016 were considered for this review. However, one article identified from the reference section–Couturier et al., 16 which was published in 1998 was obtained from the reference section of an article—met the inclusion criteria and was included in the review. Other criteria included the use of a pilot study with the participants in the geriatric age group. In addition, the study had to include usability-related data from the perspective of the patient, not from the perspectives of the doctor or the caregiver. Another criterion important for inclusion was the requirement of a direct communication between the care provider and the patient.
Studies using such communication devices as Electronic Medical Records (EMR) and self-measurement of vitals and medication adherence were not included in this review nor were studies on peripheral medical devices used as part of telemedicine and general health monitoring using web-based applications, which did not consist of care-provider and patient communications. Virtual reality-based health training applications, literature reviews, posters, and extended abstracts were excluded, as were articles discussing problems of the geriatric population, but not including results from a user research study.
Search Strategy
As part of a systematic search, the online citation index services PubMed and Web of Knowledge were searched using the keywords telemedicine AND geriatrics, and telemedicine AND usability, and telemedicine AND usability AND older people. The terms geriatrics and older people were used to find articles on the use of telemedicine by older adults, and the term usability was used to include usability studies with the geriatric population. The initial search for this review found 197 articles on the Web of Knowledge and 100 articles from PubMed.
The first and third authors independently screened the titles and the abstracts of these 297 articles identified from the search to determine which met the inclusion criteria. The remaining four authors further reviewed each abstract to determine its appropriateness, with any discrepancies between the screening and review processes being resolved by discussion between the reviewers involved. This two-step process resulted in 62 articles that met the inclusion criteria, with another 12 being selected from the references listed in these articles.
Content screening was then conducted on these 74 articles. It was found that although the mean age of the participants in several was in the geriatric range, the individual participants did not meet this age criterion. Other factors leading to exclusion were insufficient data regarding the usability of the telemedicine systems, no direct communication between the care provider and the patient, and telemedicine systems consisting of medical records and health monitoring, but no consultations. Finally, a total of 16 articles were selected for this systematic literature review (Fig. 1).
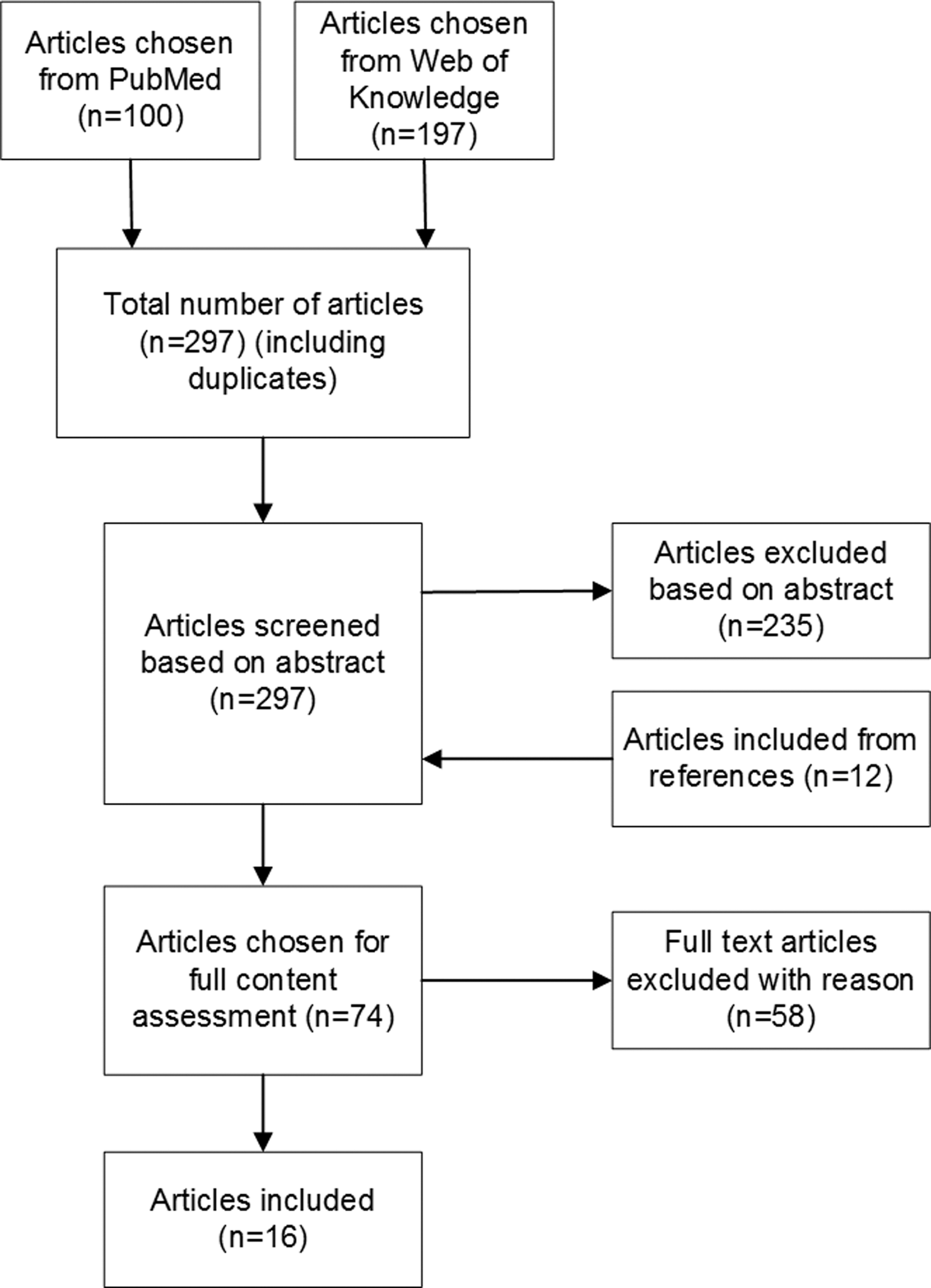
Study selection process.
Data Extraction and Presentation
A table consisting of author name, year of publication, study objective(s), methods, and a summary of findings was constructed to systematically document relevant information from these 16 publications. Table 1 below displays these data. Tables showing more specific details regarding patient selection criteria and size, the data analysis methods, the technology used, and the impact of telemedicine are presented in the appropriate sections of this article.
Summary of Research Articles
Results
Of the 16 studies identified for this review, 7 were conducted in the United States, 3 in China, and 1 each in Canada, The Netherlands, Germany, France, Denmark, and Singapore. A representation of this classification can be seen in Figure 2.
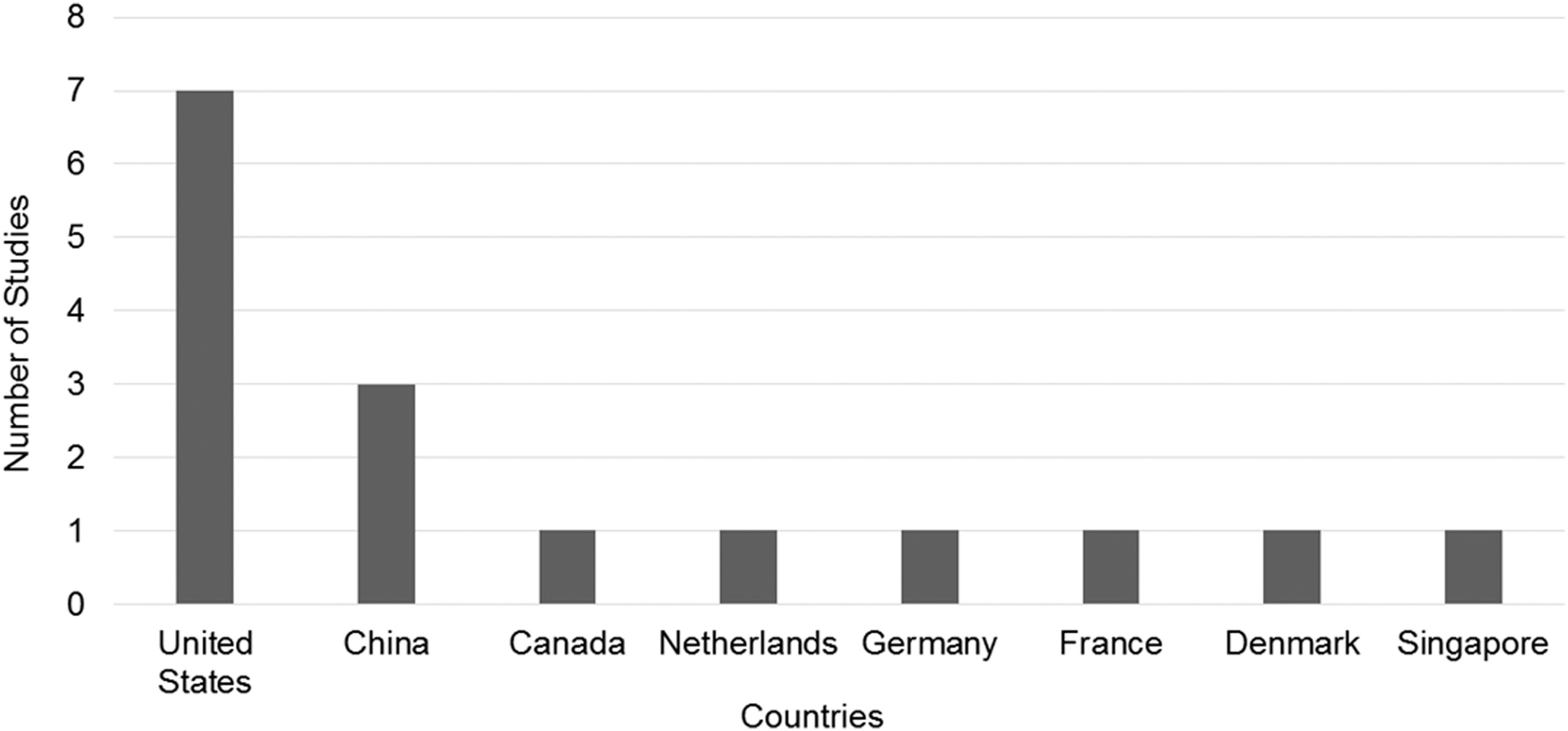
Number of telemedicine studies per country.
The articles included in this review focused on a wide array of issues, with 75% 16 –27 addressing such issues as acceptability, usability, reliability, feasibility, satisfaction, implementation of telemedicine and costs. The remaining 25% 28 –31 of the articles focused on specific objectives with patient satisfaction being one of several. However, this difference in primary objectives resulted in the studies giving limited attention to patient usability criteria. Four articles, or 25%, 20,28,30,31 involved studies using one control group and one intervention group, with the former seeing the care provider in person and the intervention group using telemedicine. Seven studies, or 43.75%, 17 –20,24,27,28 were based in elderly living centers; six articles, or 37.5%, 22,23,26,29 –31 were based in the homes of the elderly, and 18.75%, or three studies, 16,21,25 took place in a hospital/clinical setting. Details of each of these studies can be found in Table 1.
Patient Selection and Sample Size
Patient selection in 25% (four studies) was based on age only, that is, participants had to be aged 65 years or older, whereas the remaining 75% had specific criteria for patient inclusion. The four studies 17 –19,28 with the general age criterion required the patients to be within the appropriate age limit and have the capacity to independently read and sign the consent form. Some of the criteria for participant selection in the remaining 12 articles included mild cognitive impairment and mild dementia 20 as well as geropsychiatric patients. 21 Specific health conditions such as chronic systolic heart failure, 29 severe cardiac insufficiency, hypertension or unstable diabetes, 22 at least a one-year history of blood pressure problems, 23 patients with potential or active foot problems, 24 stroke patients, 25 geriatric orthopedic patients, 16 and patients requiring multidisciplinary care were criteria for participant selection in various studies. Other criteria included similarity in health issues, healthcare resource utilization and healthcare expenses, 30 heart arrhythmia, 26 and elderly living in a particular senior assisted living facility. 27
In addition to these criteria, several studies conducted tests to determine the physical frailty and mental condition of the patients. The Cantonese Mini–Mental State Examination (Cantonese-MMSE), 20 the EASY-care Two-Step Older Person Screening, 31 the Mini–Mental State Examination (MMSE), and the Epidemiology Studies Depression Scale (CESD) 23,31 were specific tests used for further screening of prospective participants.
The studies varied in their sample sizes, the number of participants ranging from 8 to 495. The average age for all the participants in all the studies was over 65, hence qualifying them to be included in this review. Table 2 lists the criteria used by each study for selecting its participants.
Criteria for Patient Selection
● indicates the patient selection criterion for each article.
Telemedicine Technology
The devices and equipment used in the practice of telemedicine varied among the studies reviewed here. The most widely used communication device for video conferencing was a computer, 16,17,20,24,31 sometimes paired with a telephone to conduct the sessions. 22,28,30 In addition, telephone calls were used by the nurse to contact patients when the vitals they uploaded were significantly different from their normal values. 22,26 Telephones were also used to interview patients upon completion of a baseline vital check and to review their electronic records, 28,30 and one study used videophones for research purposes. 27
The study conducted by Vermeersch et al. 19 incorporated a robot, specifically built for telemedicine, consisting of a laptop, cameras, a joystick for movement, and a stethoscope attached. This telepresence robot was actively involved in the sessions as the patients used it to take various simple measurements ordered by the consulting care provider.
In two studies, 23,29 devices other than conventional communication modes were provided by the healthcare providers to help patients upload their vitals onto a website. The devices used for this purpose included Health Buddy by Health Hero Network, Inc. and LifeLink Monitoring based in Lake Katrine, New York. 29 These in-home messaging devices transferred data concerning the patient's vitals to a nurse who followed up with a telephone call if a problem was detected. In addition to Health Buddy, the study conducted by Czaja et al. 23 also used American Telecare's audio–video devices and IDEAL Life Telehealth System. A color television was also used for video output in two studies 18,25 and a Tanberg 1000 Video Conferencing System was used for patient and care provider communication in one study. 21 Figure 3 represents the communication devices used categorized as per 5-year period.
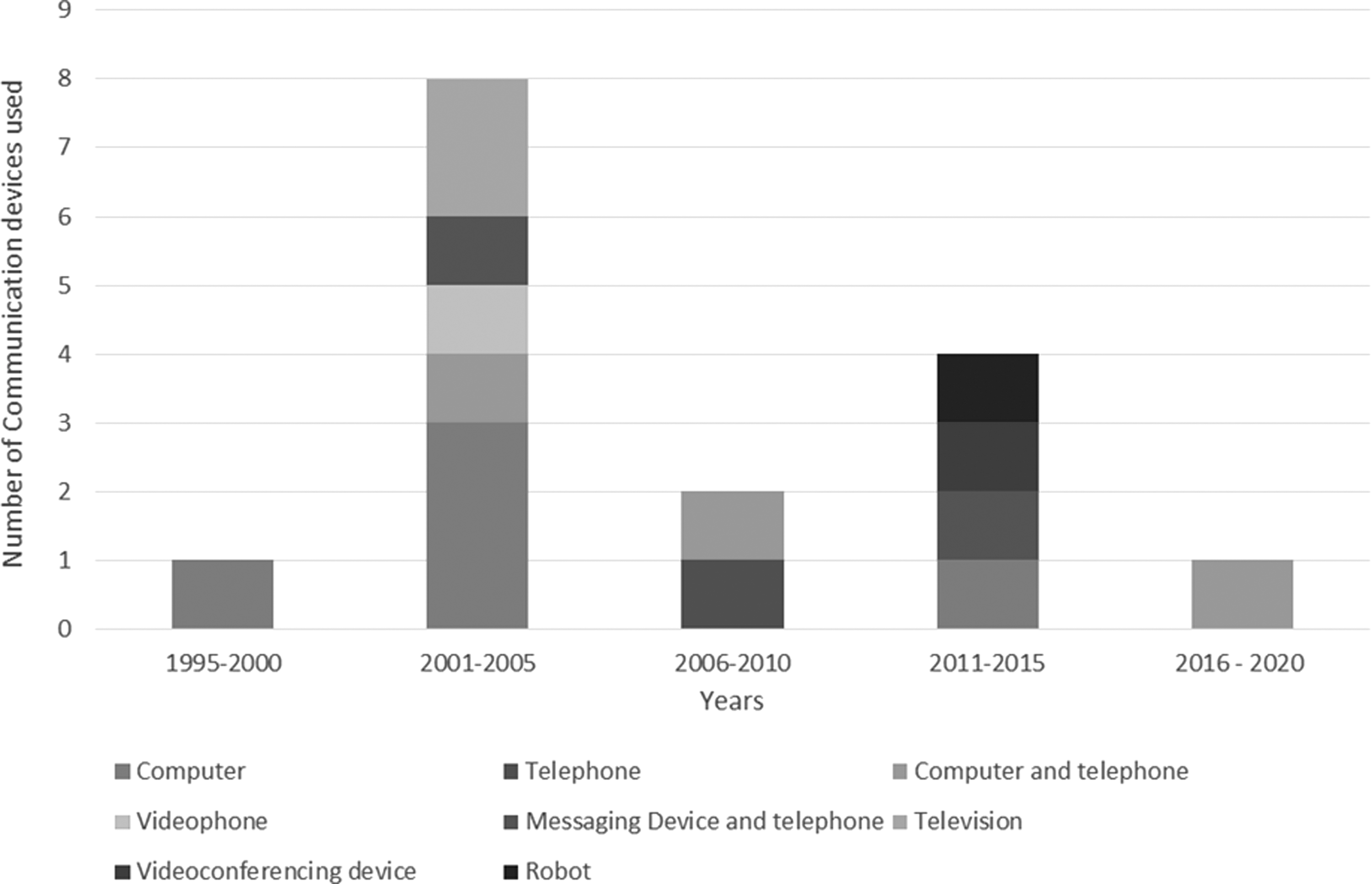
Communication devices used per 5-year period.
Peripheral devices were also incorporated with these devices. High-resolution cameras were used in 31.25% to obtain a better view of the patient, 16,18 –20,25 with one study using a 3Com webcam inbuilt in a laptop for patient monitoring, 17 and a document camera was used in another. 24 In addition to video cameras, some studies incorporated medical devices to measure blood pressure 23,26,29 and scales to measure body weight, 23,29 whereas others had a more elaborate setup, including other medical testing devices such as a stethoscope 19 and a sphygmomanometer and oximeter. 22
To transfer the medical data from the patient to the medical professional, two studies 20,21 used standard broadband connections; three studies 18,24,25 used ISDN connections; two used wireless data transfer; 19,22 three studies 23,27,30 specified telephone line connections; 1 study used a standard GSM/GPRS connection, 26 and 1 study an ADSL connection. 17 One within-hospital teleconsultation study 16 used a coaxial cable for video conferencing across rooms. Of the 16 studies included in this review, 3 did not mention the data transfer connections used, 28,29,31 referring only to the website used for the data uploaded.
Websites were also used by care providers for obtaining patient information on a regular basis. One study 31 referred to the use of a self-developed portal, ZWIP, an Online Health Community (OHC), which contained a secure messaging system and a shared Electronic Health Record. Messages shared through this portal were visible to others, and discussions could be initiated by a user. A professional could enter the discussion only with the consent of the user. Another study 28 investigated the impact of the team's Health-e-access Program for acute illness care. In this study, when a telemedicine consultation was requested, a clinical technician first collected and transferred the clinical history of the patient through an EMR Service, TeleAtrics, then initiated the consultation. Tables 3 and 4 represent the communication devices and data transmission methods used, respectively, in each study.
Communication Device Used
● indicates the communication devices used in each study.
Data Transmission Method
● indicates the data transmission method used in each study.
Data Analysis Methods
The articles reviewed in this study used a combination of both qualitative and quantitative data analysis methods, with the former primarily being for interview data, whereas the latter involved data obtained from Likert scale values and ratings for qualitative values, such as satisfaction, reliability, confidence in the system and acceptance, and for dependent variables such as the before and after effects of telemedicine. Three studies used qualitative data analysis, with the remaining using quantitative data analysis methods.
Qualitative Analysis
In the study focusing on understanding the impact of home telehealth in terms of patients, providers, and organizations, 22 data collected through interviews were recorded and compression techniques were applied. Notes made during the periodic meetings with patients were also analyzed to gain an understanding of the patient perspective of home telehealth. One study analyzed patient satisfaction surveys provided at 6-month intervals through custom-made interview questions, 30 and exit interviews at the end of the teleconsultation were used to obtain feedback on patient satisfaction in another. 21
Quantitative Analysis
In addition to a Likert scale for analyzing telemedicine characteristics, several other statistical methods were used, sometimes in combination with a Likert scale. The study conducted by Jasemian 26 used questionnaires to test the usability, reliability, freedom, and mobility, and degree of confidence and trust in the system under study. To understand improvement before and after the telemedicine consultation, a within-group paired sample t-test was used by Schofield et al. 29 In conjunction with this, a signal ranked test to compute the mean number of hospital bed days of care before and after teleconsultation was also performed. In the test conducted by Shah et al., 28 baseline values for patients were measured using descriptive statistics along with a two-sample t-test, chi-square, or Fisher's exact test. To study the impact of the use of telemedicine on emergency departments, Generalized Estimating Equations were used. A mixed design repeated measure analysis of variance was used to test for differences between baseline time and the effects of telemedicine after 6 months along with a Mann–Whitney U test to measure patient satisfaction obtained through a questionnaire. 23 Another study analyzed categorical data using a chi-square test along with the Mann–Whitney U test for analyzing ordinal data and the Student's t-test for normal data. This was combined with a 5-point Likert scale test to analyze patient satisfaction. 25
A few studies used both qualitative and quantitative data analysis. 16,17,19,21 –25,27 Likert scale values were used to find the mean and standard deviation values for characteristics such as reaction, satisfaction, effectiveness, and usefulness and written comments for each of the Likert scale questions were characterized as positive or negative. One study did not specify the data analysis method used. 17
Impact of Telemedicine
Five studies, or 31.25%, investigating patient satisfaction reported that the participants indicated high levels of satisfaction, 16,18,21,29,30 whereas a high level of acceptance for telemedicine was also found in 5 (31.25%) studies. 16,22,24,27,28 In addition, 3 (18.75%) articles 17,20,24 determined that the participants found telemedicine to be more convenient than a regular visit to the doctor. Usability and effectiveness ratings 19 in one study (6.25%) and convenience of telemedicine 25 in another were reported to have high ratings. Another study 26 reported that more than 50% of the participants reported high values for usability, reliability, privacy, and trust and confidence in the system.
Confidence in teleconsultation 17 and care coordination 29 was found to receive high ratings by the participants involved in the studies. The technology was perceived to be easy to use by the participants, 27,29 and patients indicated that they could monitor their health better 22,23 and received better health-related information using telemedicine 22 than through traditional face-to-face consultations.
Results from two studies found that the number of emergency department visits declined due to the use of telemedicine, 22,28 and two studies 18,25 indicated that the cost of telemedicine was cheaper than its conventional alternative. However, one study found low rates of usage of a telemedicine portal, concluding that introducing new technology to the older population is not easy. 31 In addition, participants reported trouble seeing and hearing the care provider as well as a general lack of confidence in the system. 18
The patients using telemedicine indicated an improved awareness of their health in addition to feeling that the technology helped them monitor their health. More specifically, results reported that patients saw telemedicine as a convenient way to manage their healthcare. 17 Users also reported reduced privacy concerns and high confidence in these systems. 26 The presence of a nurse was attributed to higher confidence in navigating through the procedure. 22 While an increase in the technological experience directly impacted the patients' attitudes toward technology, studies also showed that issues such as interference between videophones and hearing aids were reported. 27 Patients were also found to be ill at ease due to the presence and use of a camera in one study. 16 A participant in another study complained about the inability to read the numbers on a videophone used for telemedicine purpose because of the color used. 27 However, this review found that limited research has been conducted focusing exclusively on the design of the telemedicine technology and how these factors impact a geriatric user's reaction to telemedicine systems.
Discussion and Future Direction
Contrary to the common belief that older adults are reluctant to use technology, research has found that 65% of the geriatric population wants to keep abreast of current advancements. 32 However, for telemedicine systems to be usable and friendly for these older adults, there is a need to adopt a human-centered design approach in their development. 23 The majority of studies included in this systematic review were conducted late in the telemedicine system design cycle, either at the end of the system design or after implementing the system. Future research should be conducted throughout the design process, specifically considering how age-related factors may affect the interaction of the elderly with telemedicine technology and, in turn, making the appropriate design changes. These problems may be in the areas of vision, hearing, cognition, and motor skills, to name a few. 10
Vision-related issues found in the aging population include problems in visual acuity, contrast sensitivity, and visual search. Visual acuity refers to the resolution at which a person sees an object while contrast sensitivity is the ability to differentiate between light and dark areas of an object, and visual search involves the movement of the eyes in conjunction with the focus on the surrounding area when in search of a specific object. In telemedicine systems, these visual problems may manifest in older patients experiencing difficulty reading the buttons on a phone or laptop. 27
Older adults also experience hearing issues involving problems with sound localization making it difficult to pinpoint the direction of a sound or difficulties in the perception of its loudness or in hearing the background noise indicating such issues as mechanical failure of devices. 32 These sound-related difficulties should be considered in selecting devices for telemedicine as they should either include appropriate adjustments to accommodate the older population or alternative means should be provided to compensate for the hearing problems. It was found in the studies reviewed here that patients with hearing disabilities found it difficult to communicate using telemedicine equipment, and participants also reported interference between a videophone and the hearing aid in the study. 27 Such problems as these, need to be addressed, as these systems are being designed and prototyped.
An effective device or display screen is one that helps users easily navigate through a series of activities to achieve a final goal. The success of this process depends on cognitive ability, which, in older adults may be affected as a result of age, resulting in reduced working memory capacity, perceptual speed, reasoning ability, and attention. Increased reliance on environmental support or on additional information concerning a specific task is also found in older adults. In addition, spatial ability, the skill to manipulate objects based on location required, for example when reading a map or a computer screen, also degrades with age, meaning the elderly may have issues with telemedicine. Bearing in mind the visual and cognitive constraints resulting from the onset of old age, a study to understand the needs of the elderly in telemedicine computer applications must be carried out. This would lead to a comprehensive list of problems faced by the geriatric population in using these applications. In turn, their requirements in such a system and design ideas to mitigate these issues could be formed.
Finally, a loss in motor skills and motor coordination in older adults also affects their ability to carry out tasks. 10 Their response time and the time taken to complete a task as well as their accuracy in doing so are reduced with age, 32 issues that should be considered in designing telemedicine systems. In addition to these factors, other suggestions for future research in this area are provided below.
Sample Size
Of the 16 research articles considered for this review, 8 cited sample size as a limitation of the study. Most of these involved sample sizes of fewer than 50 participants, with some being as low as 8. The remaining 8 studies used sample sizes ranging from 82 to 495 participants. One article made no mention of the number of participants included in its study. 17 As these results suggest, there is a need for studies with larger sample sizes to explore telemedicine usability among the geriatric population.
Cost Analysis
Although two studies 18,25 indicated that telemedicine was a cost-effective alternative to traditional in-person visits to the doctor, more studies are needed to validate this conclusion. In addition, it is important that future work investigate the impact of the equipment (high-end audio–video devices, basic smartphones) and the setting (hospitals, nursing homes) where telemedicine is used on its cost.
Absence of External Help
Patients explicitly reported feeling more comfortable using the telemedicine system in the presence of a nurse. 22 While this presence may have been reassuring leading to higher patient satisfaction in the study, circumstances may occur when a nurse is unavailable to provide this assistance. It is important to examine how people perform without this external help. Doing so may lead to new perspectives as well as problems concerning the usability of telemedicine by the older population.
Accessibility
All studies included in this literature review were set in hospitals, elder living communities, nursing care, or private homes. In all these settings, the patients had access to private audio–video devices or community equipment specified for general use, all of which were in place before the study was conducted. However, there is a need to study the availability of Internet access and videoconferencing devices among the geriatric population in general and in rural areas specifically. 33
Others
Other areas for future work include the issues related to privacy in the exchange of medical records online, the level of participant trust associated with telemedicine systems, and the availability of insurance coverage for these sessions. The security of data uploaded online is also an issue which may need further investigation.
Limitations
This systematic review is not without limitations. The search string was very specific and may not have captured all relevant articles. The lack of uniformity in the description of the articles' descriptions of usability reporting and the methodology employed in the studies means it is possible that articles meeting our inclusion criteria were overlooked and not included in this review. The exclusion of studies not published in English may limit the generalizability of our findings to the global effort to improve telemedicine usability evaluation.
Conclusion
This article reviews the research conducted on telemedicine systems as applicable to the geriatric population, focusing on its usability. While telemedicine has repeatedly been shown to be useful in obtaining medical information and advice, this review suggests a limited number of published studies describing scientifically valid and reproducible usability evaluations at various stages of telemedicine system development. To foster user acceptance of telemedicine technologies, it is important for healthcare consumers to have a positive attitude toward using such system. 33 –35 A key factor influencing user acceptance is the usability of the telemedicine system. 33 –37 It is critical for real-world applicability to situate telemedicine applications within the context-specific needs of the people benefiting from or otherwise affected by them. 33 –37 Limited research has been conducted evaluating the usability of such tools with geriatric patients. Studies with larger sample sizes and with a special focus on use of this technology by this population are needed. The geriatric population can profit from this method of medical consultation and, hence, efforts must be directed toward understanding usability issues and addressing them to ensure effective use by the elderly, an increasing important area of research as this population group continues to grow and medical costs increase.
Footnotes
Disclosure Statement
No competing financial interests exist.