
Abstract
Background:
Most inhabitants in Latin America are concentrated in large urban foci with different access to facilities. Although the main hospitals offer specialized services, economically vulnerable populations cannot easily afford these services, the pediatric population being most affected. This article presents the design and implementation of a low cost telepediatric system, applied to primary care hospitals through a study in Bogotá, Colombia, mainly aimed to reduce the number of unnecessary transfers commonly sent to specialized medical services.
Materials and Methods:
The system was carried out over 6 months with a higher incidence of acute respiratory illness in children between 0 and 5 years in nine primary care hospitals in Bogotá. Nineteen (n = 19) pediatricians were trained by a group of engineers that supports the system permanently. The reduction of patient transfers was compared with previous reports of the National Statistical Department in Colombia.
Results:
The system reduced both the number of patient transfers to higher level hospitals by 83% and the waiting times for patient transfer, improving healthcare in pediatric patients at a reasonable cost, affecting more than 700 patients. At the same time, a decrease of about 17% in the use of antibiotics was observed, which is an important current public health issue.
Conclusions:
The use of telemedicine improves the efficiency of public health resources, even in big cities such as Bogotá, reducing the number of unnecessary patient transfers and the optimization and appropriate use of medicines.
Introduction
One of the main challenges facing Latin American health systems is the difficult access to specialized health services in underserved regions. This phenomenon has lately reached urban centers, as a consequence of the growing urbanized populations (most of them living in vulnerable areas), the increasing healthcare costs, and the inefficient management of the available services. 1 –6 Socioeconomically vulnerable people in Bogotá (about 70% of population 7 ) lack opportune access to specialized medical services. It is basically because of the limited number of available specialists to cover such population, especially for the pediatric community. While the rate of pediatric doctors is 1 per 1,096 children in developed countries, 4,8,9 in Colombia it barely reaches 1 per 5,692 children. 7,10 According to the Departamento Nacional de Estadística, * 14 of every 100,000 children casualties were caused by acute respiratory illness (ARI) in 2011. 7 This number increases during the rainy seasons (October to December and March to June 10 ), exceeding the capacity of the health public network and increasing child mortality rate of about 30%, according to the health local secretary. 10 –15
A coordinated endeavor between the health local secretary and the Universidad Nacional de Colombia's Telemedicine Center yielded the pilot study presented in this article, implementing a Web-oriented telehealth platform, adapted for the economic and technological conditions of the city's health network. The platform integrated different telemedicine modules based on the Reference Information Model (RIM) of the HL7 Standard 16,17 and several security access systems were implemented, compatible with any device able to connect to the Internet. In addition, the telemedicine software provides a communication interface that allows real-time sharing of both clinical history and videoconference that allows the increase of knowledge-sharing deal between specialists and doctors.
This article presents the results of a study, implemented during the 6 months between November and May in nine primary-level care hospitals of Bogotá. These health centers, located in the most vulnerable city areas, cared for more than 700 patients with a group of general practitioners who were supported by 19 pediatricians. This article is divided into the following sections: Methods present the system implementation process, Results introduce and analyze the obtained data, related to the number of attended patients and the conducted training. Finally, in the Discussion, results are discussed.
Methods
A general scheme of the implemented system is shown in Figure 1. The telemedicine information system, “SARURO,” 16,18 was developed in the Telemedicine Center of the Universidad Nacional de Colombia 8 years ago. The whole design was oriented to intuitively be close to a real clinical workflow: a pediatrician interacts in real time with another physician, they analyze the child's clinical conditions, and the pediatrician suggests a patient management that can be closely followed and easily modified. All cases were reported by general physicians, practitioners, and nurses using a customized electronic clinical history that facilitated the patient management, not only recording the initial patient condition but also allowing multiple evolutions of the same patient and several recommendations during a particular medical act. The average time to respond to a case was about 12 min. This set of medical interventions is collected together and easily available to any system actor with the proper permissions.
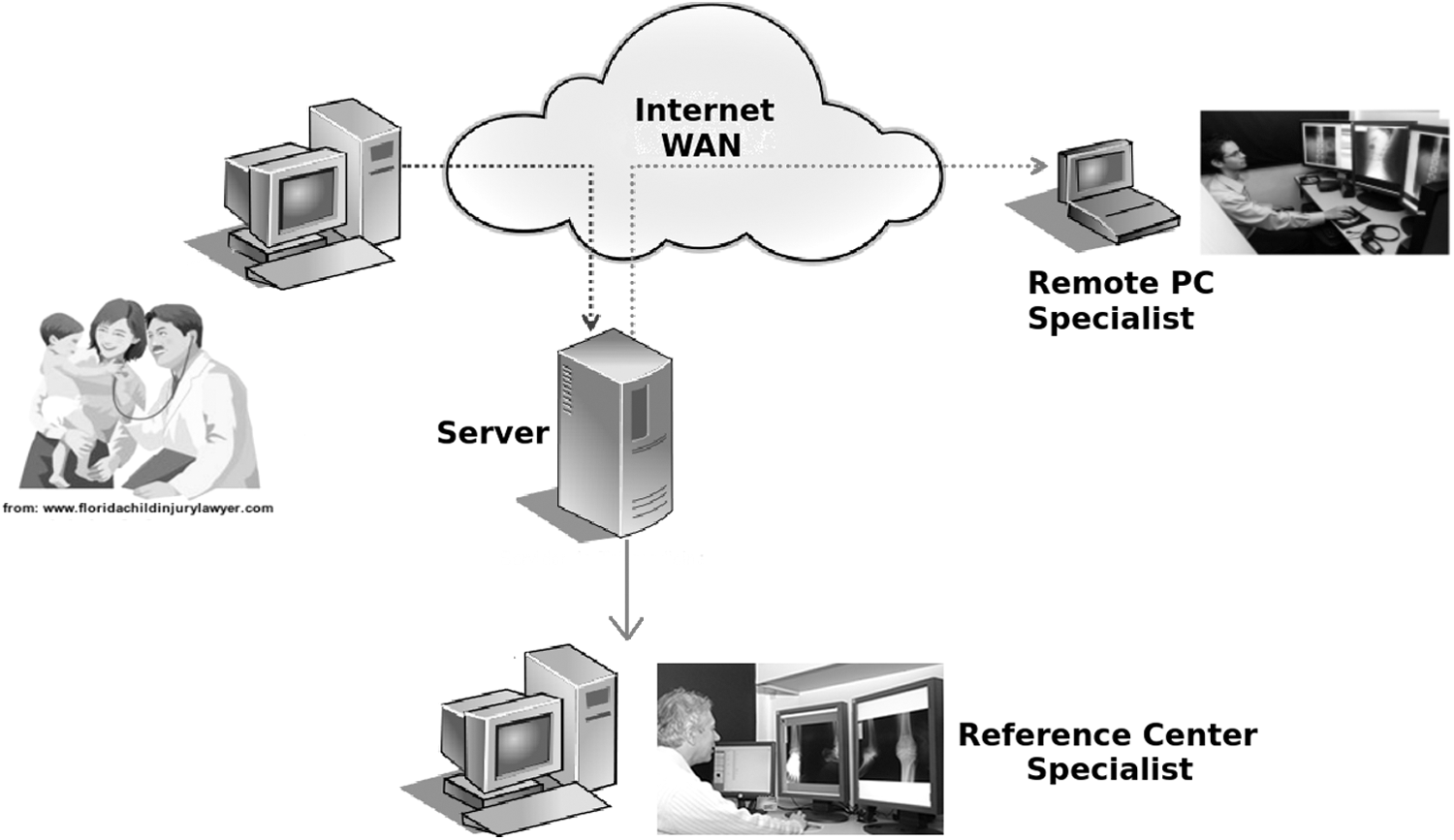
The figure shows a general scheme of the Telepediatric system, using telemedicine.
The number of cases not referred by telemedicine was counted; the physicians had to answer the following question before sending the patient case information: If your institution would not have telemedicine services, do you consider that this patient has had been referred?
The SARURO Platform
SARURO, is a Web-oriented telehealth platform adapted to the social and economic conditions of any hospital and health center. 16,18 The system is devised to operate in poorer connection conditions, using a local database that stores the information and connects with the server system when Internet is available. This platform integrates different telemedicine modules, in which medical processes are modeled using the HL7 † RIM. It is an abstract model for medical information management, defined by some backbone classes. This model provides the required versatility to obtain a proper management of any associated event. In the same way, it provides useful management of every telemedicine situation by using a reduced set of superclasses instead of the usual object-oriented classes of any language. Particularly, to control session logins and logouts, a Control Act is used for assigning roles to connected users. It means that the data model allows to audit each performed act, maintaining a register of the participating entities and roles. 16
SARURO was implemented on a PostgreSQL server, along with the needed functionalities for searching and using the medical data. The system was developed in Java, under J2EE architecture and using the JBoss application server. Besides, it provides a digital signature of the patient's clinical history, studies, and treatments, fulfilling appropriate security conditions of the medically archived information.
Training and Follow-Up
One of the most common challenges of the telemedicine systems is the user adherence. In that sense, a user training strategy was implemented during the 6 months of the project: 69 training sessions and follows-up were conducted in the nine hospitals of the public network of Bogotá. These training sessions were organized to instruct the clinicians in telemedicine general topics, advantages, proper use and management of the SARURO platform, as well as the telepediatrician information system. There were also issues related to the security of the registered medical information and use of the videoconference system. At each session, real-time demonstration cases were presented to illustrate the platform main characteristics. The courses were available to users in the virtual learning platform named “SOFIA,” ‡ also developed by the Universidad Nacional de Colombia's Telemedicine Center. The trainings sessions were supervised by a group of 19 pediatricians and 8 engineers who provided continuous and permanent support to the project.
As a complementary strategy to the training sessions, an online course of 16 h was designed and uploaded to the system. The contents of this course allowed the physician to get familiar with proper handling of medical information, taking advantage of the existing telemedicine systems. This course included the following: an introduction to telemedicine, medical signal processing, an overview of medical imaging and capture techniques, standards for the health information management, patient monitoring, and medical legal aspects and guidelines related to the use of telemedicine as a standard medical practice. It is important to highlight that an important side effect of this strategy was the generation of an intrinsic network between general physician and specialist, allowing an optimal management of patients in critical state by prioritizing the patients reported.
Public Hospital Network
The public hospital network of Bogotá is composed of 22 hospitals, hierarchically organized by complexity: 5 tertiary-level, 8 secondary-level, and 9 primary-level hospitals, distributed in 142 attention points. 7,10,11 The primary care hospitals in Bogotá attend mainly emergency cases, some coming from the outpatient clinic area and some others from the inpatient area. The unspecialized physicians and practitioners transfer the patients to hospitals of higher level of complexity when necessary. The kind of transfer is regulated by the Regulator Center of Urgency and Emergency (RCUE).
The telepediatric system presented in this article was focused on the primary level of care hospitals, located in the most vulnerable urban areas of the city. Depending on the particular time in the day and the level of traffic jam, a transfer from one of the centers to the closer hospital, may take up to a couple of hours. These hospitals just perform activities included in the National Basic Health Plan (NBHP). It means the following: general consultations, hospitalizations, and emergency care of low complexity, among others 3,11 with no access to any specialized medical service. 19 Hence, this project aimed to facilitate the access of children of the most vulnerable areas in Bogotá to specialized medical services. The 90% belonged to the subsidized health system and just 9% to the contributory regime. In Colombia, a large part of the population receives health attention supported by public funds. This proportion illustrates the large impact of this project on the economically vulnerable people of the Colombian main city. § These data were registered from the clinical history of each patient.
Results
Over the 6 months of the project, 716 consultations were performed. Table 1 shows the number of cases reported per hospital and per month. The difference in the number of cases per hospital reflects the inhomogeneous distribution of the population in the city, that is, some of these hospitals attended areas with higher population density.
Number of Cases Reported During Project Execution in Each of the First-Level Participating Hospitals
As mentioned above, one of the objectives of the telepediatric system was to reduce the number of referrals to hospitals of a higher level of complexity. Results show that many of the usually referred cases could be attended at primary-level of care hospitals, with an adequate management of the medical available resources. From the 716 reported cases, only 23% (163 cases) required transfer to hospitals with higher level of complexity, remissions (Admissions? Transfers?) performed at the pediatrician's request. This significant reduction of remissions amounts to 83% of patients resolved in the primary-level hospital, avoiding the unnecessary patient transfers in 618 of the 716 cases. About 4% of the attended children were neonates (29 cases) and 52.7% were between 1 and 11 months old (377 cases), reflecting a population most vulnerable to severe respiratory illness. 11 The rest of the 310 cases corresponded to children between 1 and 14 years.
Each of these requests was answered in a maximum of 20 min, recording each case in a usual clinical history, allowing the registration of the patient evolution at any time and a proper follow-up of the proposed specialist treatment.
On the other hand, taking into account the World Health Organization (WHO) recommendation, WHO guidelines related on the indiscriminate use of antibiotics, the pilot study demonstrated a reduction of 17.26% in the use of antibiotics. This value is the result of considering those cases in which the use of antibiotics was suspended or changed by the pediatrician (52 cases) and comparing it with the total number of cases that uses antibiotics (301 cases). The group of pediatricians guided the general physicians to change their original antibiotic formulation. In this sense, it was found that in 72 cases (10.05%), specialists completely changed the initial treatment proposed by the general physician. Likewise, a reduction in infant morbidity and mortality requires a drastic reduction of the waiting time to be attended by a specialist, particularly in case of in ARI. Herein, 43.4% of the cases were acute bronchiolitis and overall, the 68.3% of all cases was associated with respiratory disease. However, cases of other specialties were also evaluated and treated, namely Dermatology (20 cases), urinary tract infections (16 cases), seizures and fever (43 cases), and gastric diseases (44 cases) (Table 2).
The Most Common Pathologies Reported During the Telepediatrics Project Execution and the Cases Treated with Antibiotics Before Using the System
Finally, as mentioned above, a total of 20 training sessions were conducted at each hospital. A group of pediatricians and engineers instructed the hospital staff about the use of the telepediatric system. In these sessions, 228 doctors and nurses were trained (Table 3), during at least 20 days. Each was registered in the information system SARURO and a digital signature was assigned, providing optimal safety conditions for the medical information.
Number of Trained Doctors per Hospital
Discussion
Telemedicine has been reported as a useful health public tool to cope with and integrate multiple fields in healthcare practice, providing methods for planning and optimizing health resources. 5,6 This article presents the results of a telepediatric system study implemented by the telemedicine center of the Universidad Nacional de Colombia along with the District Department of Health of Bogotá, as a strategy to improve the capacity of hospitals responsible for attending the vulnerable children population of the Colombian capital. In Latin America in general, there are populations with limited access to specialized health services, 2,19,20 mainly because the high complexity hospitals are concentrated in certain city areas that are hardly accessed by most of these underserved areas. 21 In addition, there exists a shortfall of medical specialists in most of public health centers. Patients, mostly children, are attended by general doctors and practitioners, facing complicated cases. 2,3
In this project, 19 highly qualified pediatricians, members of the Hospital de la Misericordia Foundation, were involved. These specialists were hired to attend remotely all the reported cases of each health center, 24 h per day, 7 days per week. Besides, the project had the permanent support of eight telemedicine engineers. The system was implemented in nine first-level hospitals of the public network of Bogotá during 6 months, time in which 716 pediatric patients were treated.
The system proved to reduce the number of referrals to higher complexity hospitals, decreasing both the waiting times for patient transfer and extra costs produced by unnecessary patient transfers. The cases that required to be referred were requested by a pediatrician in charge. It is worthy to note that 52.7% of the cases corresponded to children less than 1 year—the most vulnerable population to any kind of disease—especially related to respiratory illness. Moreover, in some cases, the group of pediatricians guided the general physicians to change their original formulation, especially antibiotic formulation, in 17% of the cases. This is a remarkable result since in 1998, the WHO guidelines explicitly declared that the indiscriminate use of antibiotics is a public health concern, but few effective actions have been conducted against this problem. 12 This concern is not only about patient inadequately taking antibiotics but also doctors abusing their use in many treatments. In Latin America, there are few studies that assess the impact of antibiotic use in hospitals, and there is no published information on the impact of such action on antimicrobial resistance and costs. 13 –15 Hence, any reduction in their use would benefit both the population and the health system itself in the future.
On the other hand, as widely acknowledged, one of the current telemedicine challenges is in gaining doctors' adherence, especially the older ones. In this project, although the Bogotá's health secretariat obliged the participating hospitals to register every ARI case in children under 5 years, some doctors were reluctant to use the telepediatrics system. Some of them gave their username and password to an assistant and few did not simply register the patient. Moreover, some hospitals had a high turnover of medical staff. For this reason, a continuous training was required.
Finally, although the American Academy of Pediatrics Committee on Pediatric Emergency Medicine has recently adopted the telemedicine practice to improve the health service and emergency services, 22 the literature describing the use of telemedicine in pediatrics is still low and few use cases have been reported. 4,19,21 –26 This article has shown the great potential of using this modality within cities, offering high-level medicine to the most vulnerable population as an effective care strategy, and leveraging the limited structuring of the basic health network under a specialist guidance remotely located in a reference center.
Conclusion
It is known that the telemedicine is a useful tool to bring specialized medical services to underserved regions. However, this article shows that its impact is also important for economically vulnerable cities. In total, 716 cases were attended by a group of 19 full-time available pediatricians. It showed the great potential of these strategies to reduce the mortality and morbidity rates in children. This platform was designed for use over any device with internet connection. On the other hand, the permanent interaction between physicians and specialists allowed constructing a health support network, helping to face together some health public problems such as the treatment of chronic respiratory diseases and the appropriate use of antibiotics, benefiting the most economically vulnerable people in rural areas, as commonly reported, but also in big cities as is herein presented.
Footnotes
Disclosure Statement
No competing financial interests exist.