
Abstract
Background:
Shared-risk models encourage providers to engage young patients early. Telemedicine may be well suited for younger, healthier patients although it is unclear how best to incorporate telemedicine into routine clinical care.
Introduction:
We test the assumptions surrounding the use of telemedicine, younger and rising-risk patients, and primary care in ClickWell Care (CWC), a care model developed at our institution for our own accountable care organization.
Materials and Methods:
CWC's team of physicians and wellness coaches work together to provide comprehensive primary care through in-person, phone, and video visits. This study examines usage of the clinic over its initial year in operation.
Results:
1,464 unique patients conducted a total of 3,907 visits. 2,294 (58.7%) visits were completed virtually (1,382 [35.4%] by phone and 912 [23.3%] by video). Patients were more inclined to see the physician in-person for a new visit (1,065 visits [70.5%] vs. 362 [24%] phone and 83 [6%] video) and more likely to see the physician virtually for a return visit (606 [43.2%] phone and 249 [17.7%] video vs. 548 [39.1%] in-person), a statistically significant difference (X2 = 306.7, p < 0.00001).
Conclusion:
This new care model successfully engaged a younger population of patients. However, our data suggest young patients may not be inclined to establish care with a primary care physician virtually and, in fact, choose an initial in-person touch point, although many are willing to conduct return visits virtually. This new model of care could have a large impact on how care is delivered to low- and rising-risk patients.
Introduction
The implementation of the Affordable Care Act (ACA) laid the groundwork for significant reform of healthcare delivery by driving healthcare practitioners to focus on providing high-value and patient-centered care. The ACA has increased demand for primary care, 1 stimulating efforts to deliver care through innovative delivery models such as patient-centered medical homes to meet this need. 2 Such medical home models have often been the basis of successful programs for treating older, more complex patients using teams consisting of physicians and staff, including health coaches. 3,4 However, very little energy has been focused on younger, healthier populations. While these patients may not consume healthcare resources to the extent that chronically ill patients do, it is important to instill in them healthy habits and lifestyles to prevent chronic disease, control long-term healthcare costs, and achieve population health. The movement of the health system toward a shared-risk, population health-based model encourages us to engage our young patients early in their healthcare journey for the long-term health of the population.
New technologies that increase the personalization and individualization of healthcare have the ability to improve how we care for healthy patients. Among new technologies, telemedicine has emerged as one way to increase engagement and access to care, although it is still unclear how best to incorporate it into routine clinical care. Some current consumer-driven models of telemedicine do not engage in preventive or longitudinal primary care, instead handling mostly same-day and urgent issues, leading to fragmented, episodic medical care. 5,6
We describe the design and implementation of an innovative primary care model that tests the assumptions surrounding telemedicine, younger healthy and rising-risk patients, and primary care; we also provide initial learnings from its first year of operation. This novel, virtual primary-care clinic, ClickWell Care (CWC), was developed at our institution for its accountable care organization (ACO) and fully integrates clinical care with technology and wellness coaching.
Materials and Methods
Patients
For their healthcare, Stanford employees may select among several health plans, including Kaiser, an exclusive provider organization plan, and our institution's own ACO. Patients enrolled in the ACO were asked to choose primary care services within the health system. Beginning in January 2015, CWC, was one option for primary care. All patients who chose CWC were enrolled in this study, which was approved by the Stanford University Institutional Review Board.
Patients learned about CWC as an option for primary care through a mailed brochure sent to all enrollees or through our institution's primary care scheduling call centers when they called to book an appointment. The call center staff were trained to administer a health risk assessment (HRA) and were given in-service training and a script to describe CWC to interested patients.
Patients eligible for CWC included our employees aged ≥18 years who were able to speak, read, and write in English and were willing to do phone and video visits. While members of the ACO are our employees, as healthcare providers at CWC, we treat them as our patients. While we were most interested in the effect of our virtual offerings on younger patients, there was no upper age limit as CWC was open to all Stanford employees; some patients were older than the age 65. Ineligible patients included those hospitalized in the past year for any serious chronic medical condition such as uncontrolled diabetes, coronary artery disease, or stroke, or other serious medical issues as measured by the HRA administered to new ACO members. There was no exclusion criterion for patients with mental health challenges.
The CWC Model
The CWC is a “bricks and clicks” model, in which the physical brick and mortar clinic is the hub of care when needed but, in general, patients interact with their physicians and care team predominantly through virtual means. The care team is composed of physicians and wellness coaches working together to provide comprehensive primary care delivered through traditional in-person visits as well as virtual visits through phone and video. Expanded operating hours allow patients to access physicians between 7am and 9pm Monday through Friday and 9am–5pm on weekends. Primary care physicians (PCPs) manage new and return visits either in-person, through video visit, or by phone. They engage patients in both acute care and preventive health and help them identify initial health goals.
Patients schedule visits to their healthcare provider in CWC when they have a health problem or question or when they wish to have a physical examination. They are allowed to choose which modality they would prefer. At each new patient visit regardless of how the patient was seen (e.g., in-person, phone, or video), the provider explains to the patient how CWC operates and presents them with information on how to conduct phone and video visits.
Patients are then offered virtual wellness coaching appointments, without additional charges, to help them reach their health goals. Wellness coaches are certified trainers with additional training in nutrition and mindfulness-based stress reduction. Visits with wellness coaches are conducted only through phone or video. The wellness coaches work with patients to create physical activity plans, review dietary habits, and do virtual “cupboard raids” to understand each patient's current habits. They then work with patients virtually to create healthy grocery lists/menus and to review exercise techniques to help drive patients toward their wellness goals. In addition to physical activity and nutrition, wellness coaches engage patients on mindfulness and sleep hygiene. Patients are able to access a wellness coach from 7am to 8pm Monday through Thursday and 9am to 5pm on Fridays and Saturdays.
To improve adherence to wellness coaching and physician plans of care, CWC works with third-party companies to provide additional services such as same-day home delivery of medication free of charge to patients. 7 The goal of the third-party partnerships is to decrease the barrier to access the services needed to achieve healthy behavior while improving adherence.
Technology
Patients schedule video visits with physicians or wellness coaches through our secure online patient portal, MyHealth, or by calling CWC. 8 Patients can also engage with CWC through secure email communication and asynchronous photo consultations, where a patient can securely upload images to the online portal for later review by a physician. Video visits can be conducted through both the MyHealth (Stanford Healthcare's MyChart portal) mobile app and a web interface on a computer. The portal is fully integrated with the EPIC electronic medical record (EMR) currently in use at Stanford, allowing providers access to the patient's chart while conducting telemedicine visits. Providers document all telemedicine encounters within the EPIC EMR to assure patients' continuity of care.
Patients can also monitor and record pulse, blood pressure, and weight at home through manual entry into Apple Health or MyHealth, or by syncing a Bluetooth device such as a Withings device to Apple Health or MyHealth. If syncing data from Apple Health, patients must grant access to Apple Health through the MyHealth app. Data obtained is sent directly through the Cloud into their EMR for review by their physician or wellness coach.
All data between apps and backend servers are exchanged over encrypted links. User sessions are automatically logged out when the app is not in use to ensure that no patient health information is left on the device by our application. In addition to our internal testing, independent security audit firms are regularly engaged to validate the integrity of the end to end system.
Results
Preliminary Needs Assessment
When the ACO launched in January 2014, before the launch of CWC, the ACO plan was chosen by 10,052 of our 29,930 employees. Among the patients in the ACO, 78.7% selected a PCP while 21.3% did not; the latter group were auto-assigned to a PCP. The majority (53.7%) of the auto-assigned group were adults aged 18–40. During the first 6 months of the ACO, 42.7% of this group received at least 1 medical service compared with 54.9% of members who chose their own PCP (p < 0.00001). Of the services the auto-assigned group used, 5.6% were delivered in the Emergency Department and urgent care compared with 3.6% for those who had chosen a PCP (p < 0.00001). CWC was created in response to these findings of over-use of more expensive and fragmented emergency and urgent care and lack of engagement in preventive care, especially by younger patients.
Study Period
During its first year (January–December 2015), CWC engaged 1,464 unique patients, conducting a total of 3,907 visits (2,913 with a physician, 994 with a wellness coach) (Table 1). Fifty-five percent of visits with the physician were scheduled on the same day as requested. We found that 2,294 (58.7%) visits were completed virtually (1,382 [35.4%] by phone and 912 [23.3%] by video). For appointments with a physician, 1,300 (44.6%) visits were virtual compared with 1,613 (55.5%) in person. For virtual visits with a wellness coach, 580 (58.4%) visits were by video compared with 414 (41.6%) by phone.
Total Visits by Visit Modality
MD, medical doctor; WC, wellness coach.
When looking at our overall patient population (aged 18–65+), we found that our patients were more inclined to see the physician in-person for a new visit (1,065 visits [70.5%] vs. 362 [24%] phone and 83 [6%] video) and more likely to see the physician virtually for a return visit (606 [43.2%] phone and 249 [17.7%] video vs. 548 [39.1%] in-person) (Fig. 1). This finding was statistically significant (X 2 = 306.7, p < 0.00001). As we further segmented our population, we found patients aged 65+ were more inclined to see the physician virtually for new visits with 65.3% of such visits completed virtually compared with 27.8% in the 18–40 age range (Fig. 2). This difference disappears for return visits with 55.6% of all return visits completed virtually by those 65+ compared with 61.6% in the 18–40 age range (Fig. 2). For new visits, this was a statistically significant finding (X 2 = 9.13, p = 0.003). For return visits, there was no statistically significant difference between the age groups (p = 0.701).
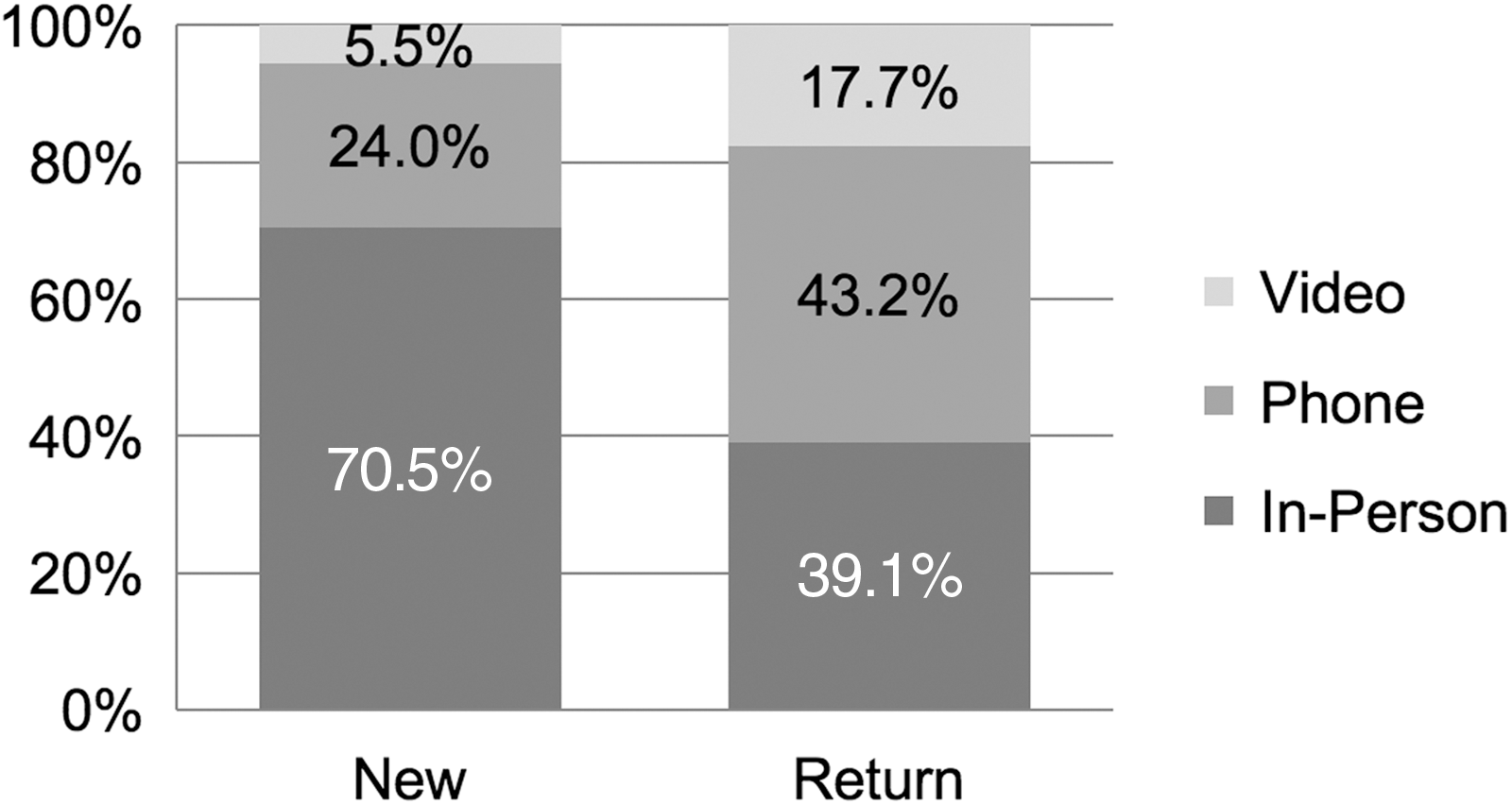
Physician visit modality by percentage of new versus return visits.
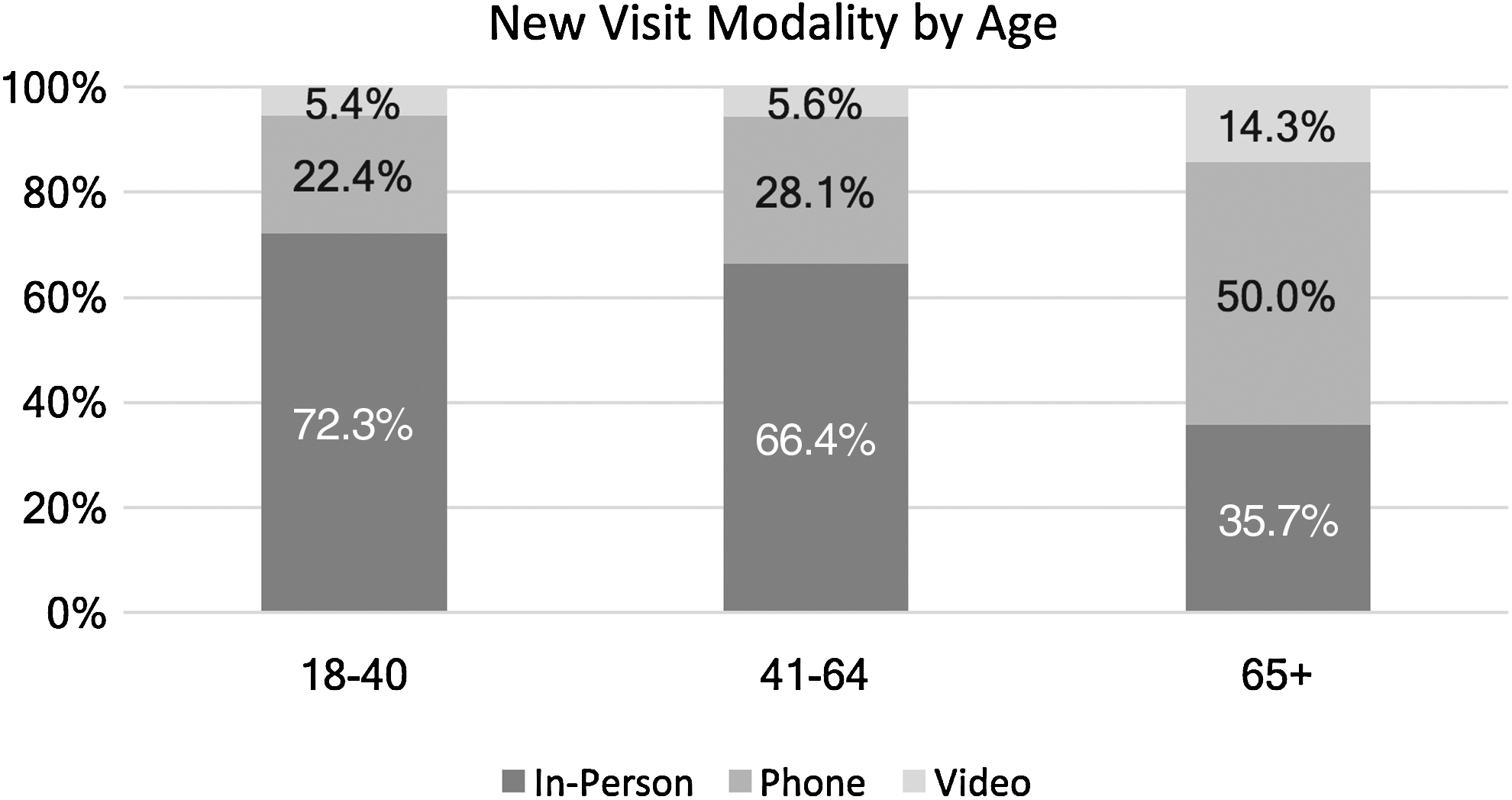
New visit modality by patient age.
CWC enrolled younger patients (average age 35.6 years) than our traditional primary care clinics (50.6 years) (the data on average age in our traditional primary care clinics were generated by our Operations department) (Table 2).
Demographics by Total Visits
MD, medical doctor; WC, wellness coach.
The most common diagnoses were related to preventive care, including routine physical examinations, vaccinations, and healthcare maintenance followed by more acute issues such as rashes, back pain, and urinary tract infections.
Discussion
In its first year, CWC was shown to more effectively care for younger, healthy, and rising-risk patients who had failed to engage with primary care and had overused emergency and urgent care services as members of our ACO. The average age of patients in this clinic was <40, yet, despite being tech-savvy, they were less inclined to establish care with a PCP virtually as previously suggested in consumer surveys. 9 –11 More than 70% of patients younger than 40 chose an initial in-person touch point, although many were willing to conduct return visits virtually. For this population, access to same-day visits, even for preventive healthcare, was of high importance.
Interestingly, older patients in our study were more likely than younger ones to complete a new visit virtually although more likely to choose to be seen in-person for a return visit. This finding demonstrates that older patients may not be limited by the use of technology. We suspect older patients are more experienced with the health system and therefore understand that in-person physician visits are not always necessary to receive care.
Practices that embed virtual visits, including both telephone and video visits into primary care are rare. Many of them support rural communities or rely on point-to-point settings to deliver care. 12,13 Many offer phone and email visits alone but only to return patients. 14 –17 Kaiser Permanente implemented direct-to-consumer phone and video visits in their primary care and specialty practices in 2014. That year, 13,000 video visits were performed across 5,000 providers, demonstrating that there were few virtual visits for each individual provider. 18
Many researchers have claimed that telemedicine is especially well-suited for younger and healthier patients, 5,9 –11 “the ‘worried well,’ who simply want a quick resolution to their minor medical complaint.” 9 Citing patient surveys, they conclude that young patients would rather receive low cost, convenient healthcare than have a regular PCP. 9,11 However, conflicting surveys have shown that having a relationship with a PCP is indeed important. Recent research suggests that having a relationship with the same PCP over time improves quality of care, decreases hospitalizations and emergency visits, and increases patient satisfaction. 19 Despite these disparate claims, there has been little systematic research to suggest how young, healthy patients would choose to receive care and little evidence to suggest best practices for engaging them in preventive care.
Health coaching integrated into primary care has been reported in numerous studies as a way to improve outcomes, increase patient satisfaction and engagement, and increase trust in PCPs 20 –24 but has often been offered only to patients who are at high risk or patients with an identified chronic disease. 21 –28 Most such programs engage in telephone coaching without the option of video coaching, 23,25,28 and some require face-to-face visits for the initial encounter. 20,22,27,29 One such program, Mercy Clinics, uses certified registered nurses as health coaches. They reach out to patients before and between physician visits. They assist with management of diabetes and hypertension and contact patients overdue for care to ask them to return in person to the primary care clinic. They also offer self-management support but require patients to meet with them in person for their initial visit. 30,31
While companies such as Teladoc engage a younger subset of patients who have had less previous access to care, 5 these virtual urgent care companies do not provide primary preventive care nor do they offer a brick-and-mortar location staffed by the same physicians. Thus, CWC is the only primary care clinic to effectively target a younger, healthier population of patients through an integrated clinical and wellness program that delivers a large amount of its care through virtual visits.
CWC differs from previous models for several reasons, including the ability for patients to receive all of their care virtually through phone and video visits; a focus on younger and healthier patients; integrated wellness coaching; not focused solely on chronic disease; and delivered exclusively through phone and video visits.
While our initial results provide some interesting preliminary insights, we are still evaluating the effectiveness of our model. Our finding that young patients want in-person touchpoints with their providers will be useful to others planning to implement similar programs. However, more data are required over time, including the volume of visits by both young and older patients, as well as trends in the use of emergency and urgent care. We plan to continue our research in this clinic and will report utilization trends as well as data on patient satisfaction, outcomes, effectiveness of wellness coaching, and cost effectiveness.
Limitations
Our study has several limitations. It includes just 1 year of data from a new model of care we introduced in 2015 to employees of Stanford University. The number of patients enrolled in CWC was small relative to the entire population of Stanford University employees. Furthermore, the results may not be generalizable to a larger population, most notably with regard to education and comfort level with technology given Stanford's location in Silicon Valley.
Conclusions
Virtual primary care serves as an interesting and innovative new model of care that could have a large impact on how care is delivered to low- and rising-risk patients. We believe it is a potential model for consideration by other ACOs and primary care clinics across the country.
Footnotes
Disclosure Statement
No competing financial interests exist.