
Abstract
Introduction:
Family caregivers are socially isolated and burdened as they care for their loved one, often for many years. Internet support groups can address some of the barriers related to the social isolation, self-efficacy, and burden experienced during caregiving by connecting individuals with similar problems to one another. The purpose of the meta-analysis was to analyze the effect of Internet-based group support interventions on social support, self-efficacy, and burden.
Methods:
A two-step search process was used to identify peer reviewed evidence to answer the research question. Multiple databases, including MEDLINE, Cochrane Database of Systematic Reviews, CINAHL, PsycINFO, and several others, were searched to identify systematic reviews from which to identify the final articles for data extraction.
Results:
Seven systematic reviews identified 10 studies to answer the research question. A statistically significant effect was found from the interventions targeting social support and self-efficacy. We were unable to assess the effect of these interventions on caregiver burden due to the variance in measurement constructs.
Conclusions:
While it has been found that Internet group support interventions have a positive effect on social support and self-efficacy, the size and quality of studies are moderate, and thus, large-scale randomized controlled trials are needed for a higher level of evidence.
Introduction
Peer support has been found to be beneficial for caregivers, as it promotes positive emotional support, allows the venting of negative feelings, and assists caregivers with finding strategies for challenging circumstances. 1 –3 Group support has been found to be helpful for caregivers of patients with a variety of conditions, including cancer and dementia. 1 Numerous theories support this approach, and a variety of group support interventions have been designed and evaluated 1,3 and shown to improve many different health outcomes. 4 –7
While group support interventions may be beneficial, the challenges of designing and implementing them are also well known. Overcoming scheduling conflicts and geographic barriers to meet the needs of several people have long been reported as reasons since participating in groups can be limited. In the case of caregivers, the inconvenience of traveling to a central location and the need to have someone stay with the patient while they are gone are significant barriers. 8
In the 1990s, numerous studies found telephone-based groups to be a useful alternative to face-to-face groups. 9 –11 With the increasing availability of technological tools through the Internet, a number of Internet group interventions have been designed and tested. 4,12 –15 These interventions allow numerous individuals to interact with one another in a supportive manner either through video, chat features, or a bulletin board type experience with or without a designated leader. In addition, the Internet has made the availability of both synchronous and asynchronous interventions possible for homebound caregivers, lessening the impact of scheduling conflicts and geographic barriers. Group intervention technology tools that can support caregivers include synchronous video- or text-based communication options, online educational and peer support classes, and online coaching or help forums. Asynchronous support options include bulletin board or message board discussions, group e-mail communication, libraries for educational material, educational videos, and online clinical reports. 12,16 –23 In addition, group interventions hosted on social networking sites such as Facebook have been evaluated 24 –28 and found to be feasible and promising in terms of improving caregiving outcomes. 29
As technology use has increased, the evidence for Internet group support interventions has also grown. While numerous outcomes have been studied, we were particularly interested in social support, self-efficacy, and caregiver burden. Recent studies of hospice caregivers found that social support decreases during hospice stays, 30 at the same time caregiver self-efficacy is needed, and burden increases. 31 As well, a small pilot study on using Facebook for group support found it a feasible and promising intervention for hospice caregivers. 29 Thus, the purpose of this meta-analysis was to answer four basic questions related to Internet group support interventions for adult caregivers: (1) What is the effect of Internet group support interventions on caregivers' social support?; (2) What is the effect of Internet group support interventions on caregivers' self-efficacy?; (3) What is the effect of Internet group support interventions on caregiver burden?; and (4) What are the most tested Internet-based intervention components for caregivers of adult patients?
Methods
Selection of Studies
An initial literature search found numerous systematic reviews that focused on similar research questions. To assure an in-depth review of the most recent literature, we narrowed our search criteria and implemented a two-step process to identify the most recent and relevant studies. Step one involved searching databases for systematic reviews or meta-analyses related to online group support for caregivers. Using existing systematic reviews or meta-analysis, we were able to narrow the search to the most current and applicable studies. Existing systematic reviews and meta-analyses were selected based on the following inclusion criteria: (1) they included original studies of online group support interventions for adult family caregivers of adult patients; (2) they were published during or after 2013; and (3) they were published in English. Searches were run in the following databases: MEDLINE (2013–2016), MEDLINE In-Process (2015), Cochrane Database of Systematic Reviews, CINAHL, PsycINFO, Social Services Abstracts, Sociological Abstracts, and Scopus. The following terms and their synonyms were searched as controlled vocabulary terms or as text words in each of the databases: (self-help group$ or support group$ or social support$ or social network$) and (online support$ or online or internet or facebook$ or web$1 or website$ or web site$ or computer media$ or chat or chats or chatted or chatting or chatroom$ or chat room$ or world wide web or
Using this strategy, we identified 26 reviews. After removing duplicates and excluding reviews that did not meet our inclusion criteria, seven systematic reviews remained. The original search strategies used in each of those seven systematic reviews are included in Table 1.
Search Strategy of Systematic Reviews Retained on Measuring Social Support, Self-Efficacy, and/or Caregiver Burden
The second step in our process was to identify original studies from the seven systematic reviews. The reviews contained 195 research articles. To be retained for subsequent analysis, studies met the following inclusion criteria: (1) the study was published in 2000 or later; (2) the study was published in English; (3) the study participants included adult caregivers of adult patients with at least one chronic health condition; (4) the study evaluated an Internet-based intervention that included at least one component focused on group support (rather than support of individuals or dyads only); and (5) the study reported outcomes related to caregiver social support, self-efficacy, and/or burden. Studies were not required to be of any specific design (experimental, observational, etc.) as long as they had the designated outcomes. Specifically excluded were studies focused on caregivers of patients with mental illness and/or those that evaluated interventions focused exclusively on monitoring of physical or functional status. Studies focusing on different outcomes were used in a separate analysis.
Data Extraction and Coding
The first two authors (D.P.O., S.P.) developed an initial code book based on a cursory review of the studies in the final sample. Risk of bias was assessed using Cochrane's risk of bias tool, which was part of the codebook and consists of five items (sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting). All authors except S.P. were divided into three coding teams. Each team pilot-tested the initial code book with a review of two studies. The codebook was subsequently modified based on feedback from the teams. The remaining sample was divided among the three coding teams. Each team member independently reviewed each article and compared findings with the second team member, reaching consensus on the final extracted data. Once the coding teams reached consensus on their assigned articles, the information was given to S.P. for a third review, analysis, and final consensus.
Data Synthesis and Analysis
Studies were grouped for analysis based upon their description of individual outcomes of social support, self-efficacy, and caregiver burden. Statistical analyses were performed using Comprehensive Meta-analysis Software version 3 (Biostat, Inc., Englewood, NJ). The standardized mean difference (SMD) of postintervention data for main outcomes between online group support interventions and control groups was calculated. Because we expected varying intervention effects, we used the DerSimonian and Laird random-effects model to compute effect sizes because it uses the assumption that different studies are estimating related but different intervention effects. 32
A SMD effect size reflects the difference in means between treatment and control subjects in terms of their standard deviations; hence, it can be used if similar outcomes are reported using different scales. 33 As our studies measured the outcomes of interest with varying scales, we calculated the SMD instead of the difference in means. We calculated 95% confidence intervals, and we considered p < 0.05 statistically significant for all analyses. Heterogeneity among studies was evaluated by the Q statistic, with p < 0.10 indicating heterogeneity, and by I 2 statistics. I 2 values over 50% may indicate substantial heterogeneity and 75–100% indicates considerable heterogeneity. 34 Publication bias was assessed using a funnel plot and the Egger regression test.
Results
Literature Search
The results of the review process are diagramed in Figure 1. The final number of systematic reviews meeting criteria was seven. Table 1 summarizes the search strategy for each of the reviews. From those 7 reviews, 10 original studies had outcomes of social support, self-efficacy, or caregiver burden. Studies included a variety of patient conditions. Table 2 details each of the articles included in this meta-analysis and links them to the systematic reviews from which they originated.
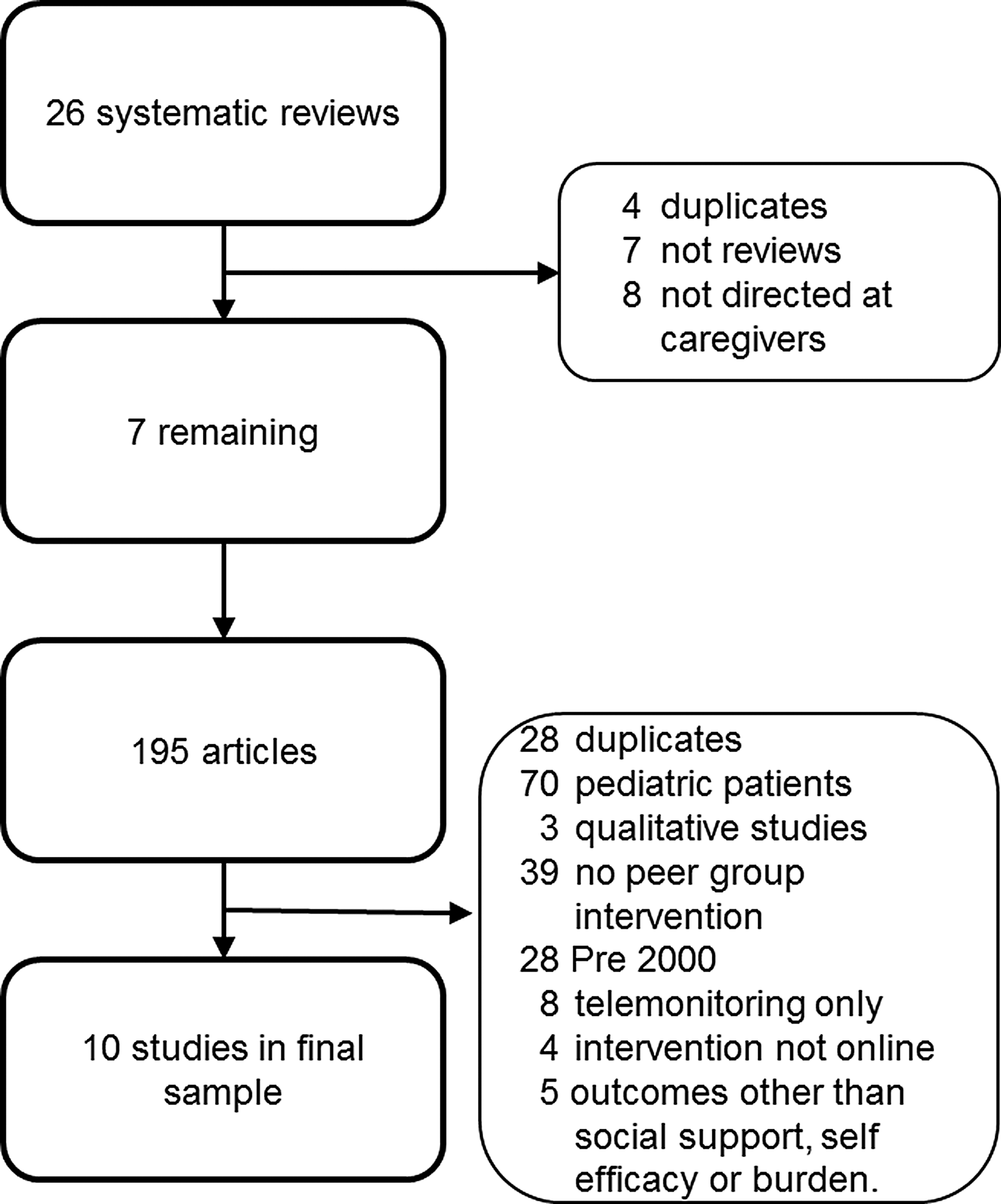
Flow chart of selection process and sample.
Summary of Studies Included in Current Meta-Analysis
CGB, caregiver burden; SE, self-efficacy; SS, social support.
Interventions
Table 2 summarizes the components of each of the interventions tested. While our inclusion criteria required that studies evaluate interventions that included at least one group-level component, not all components in each intervention were targeted to groups. For example, one intervention provided individual participants with links to Web-based educational information, but also had a group video chat. 16 All interventions but the one reported in Ducharme et al. 21 contained both synchronous and asynchronous components. The number of intervention components ranged from 2 to 5. The most common intervention component, used in 7 of the 10 studies, was Web site links to educational resources regarding caregiving and specific disease information. The second most used component was an online coach or help structure for implementation, problem solving, emergency support, or questions. Only the Ducharme et al. 21 and Lai et al. 35 interventions involved online group classes with an educational focus, and only the Chih et al. 12 and DuBenske et al. 23 interventions involved clinician reports, which were summaries of the individual's health condition that were given to the care team.
Risk of Bias and Quality Assessment
Table 3 summarizes the quality assessment for the sample using Cochrane's risk of bias criteria. 34 Of the 10 studies, 3 were nonrandomized. Of the seven randomized controlled trials, three studies 12,19,23 reported their randomization sequence generation and mentioned allocation concealment. Hence these three studies are the only ones in our dataset that were determined to have low risk of bias. The remaining four randomized controlled studies mentioned randomization methods, but did not specify sequence generation techniques. These remaining four also failed to report on the allocation concealment and, thus, are considered at high risk of bias. Blinding participants would be difficult due to the nature of the intervention requiring participant involvement; however, one study blinded the outcome assessors, while three studies did not report blinding and six did not blind. Finally, regarding reporting of incomplete outcome data, attrition was well described in six studies, not adequately reported in three studies, and not addressed at all in one study. Of those six reporting complete data, we could assess that four were not selective in which outcomes were reported and the remaining studies did not report enough information to assess if outcomes were selectively reported. As noted in Table 3, of the total of 50 criterion cells (5 cells for each of 10 articles), low risk of bias was found in 18 (36%), and high risk of bias was determined in 16 (32%). We were not able to determine risk in 16 (32%) of the criterion cells. In conclusion, only three studies 12,19,23 had low risk of bias in each category of bias assessment. All other studies were determined to have low to moderate risk of bias. There was no publication bias noted on funnel plots or Eggers regression (p = 0.41 for social support outcomes and p = 0.20 for self-efficacy outcomes).
Risk of Bias in Included Studies Using Cochrane's Criteria
Randomization was mentioned, but no information was provided on sequence generation.
Studies were nonrandomized.
Selective outcome reporting evaluates if all of the prespecified (primary and secondary) outcomes have been reported in the prespecified way. We found this difficult to assess in most of the studies as there was no published protocol.
Outcome assessors were blinded.
Social Support
Five studies evaluated the effect of Internet group support interventions on caregiver social support. Three of the studies 17 –19 were randomized with groups assigned as either a control or a comparison group. One study 16 compared two intervention support groups (text-based and video chat). Two studies did not have any type of control or comparison group. The length of time the Internet interventions lasted ranged from 3 weeks to 18 months. While all studies used outcome instruments that measured social support, they all used different instruments. The sample sizes ranged from 19 to 91 individuals.
The overall pooled effect of Internet group support interventions on social support was a statistically significant SMD of 0.464 (95% CI 0.118–0.811, p = 0.009) for a total sample of 222 caregivers. Because social support was measured using varying scales, we could not convert the SMD to the original metric. Our calculations indicate that there was an improvement equivalent to almost half of a standard deviation of the baseline scores in intervention group compared to control. There was moderate heterogeneity of results noted with an I 2 = 58.92%, which means almost 59% of variance noted in effect sizes reflects true variance in effect. Of the five studies that reported social support outcomes, only the Smith 19 study did not show improvement in social support with Internet group support. Study results are detailed in Figure 2.

Effect of interventions on social support.
Self-Efficacy
Three studies measured self-efficacy with different instruments. The individual sample sizes ranged from 21 to 91. One of the studies 21 did not include a comparison group. The remaining two studies compared two interventions. 16,22 The length of the interventions ranged from 11 to 20 weeks. The overall pooled effect of Internet-based group support on self-efficacy was statistically significant, with a SMD of 0.44 (95% CI 0.22–0.659, p < 0.001) for a combined sample of 132 caregivers. Similar to social support, self-efficacy was measured using varying scales so the effect size would be 0.44 times the standard deviation of the baseline scores. The heterogeneity was low with an I 2 of 18.40%; hence, only 18.4% of the observed variance reflects real difference in effect sizes. Self-efficacy results are depicted in Figure 3.

Effect of interventions on self-efficacy.
Caregiver Burden
Meta-analysis of caregiver burden outcomes was not possible because of the measures chosen and the study designs. We are not confident that the four studies defined and measured burden comparatively. Therefore, we did not combine effects in a meta-analysis, but reported the studies as a part of our review and comparison of interventions. Chih et al. 12 did not measure the intervention effects on burden but rather the effects of a clinician report that summarized symptoms and caregiving needs on burden, with no difference noted between intervention and control group in perceived burden. Glueckhauf 22 measured subsets of the Caregiver Appraisal Inventory. Subjective emotional burden was significantly better during posttest measurements, while positive aspects of caregiving subscale and time burden subscale were not significantly different between pre- and postintervention periods. DuBenske et al. 23 measured caregiver burden as the subjective impact of caregiving using the Caregiver Quality of Life-Cancer Scale and Burden Scale and showed significant improvement in the intervention group compared to control at 6 months on these burden scales. Lai et al. 35 used the Chinese version of the Zarit Burden Interview, and results were only reported in median and range form with no significant difference noted between online and on-site participant burden.
Discussion
The results of our meta-analysis indicate that Internet group support improves social support and self-efficacy among caregivers of adult patients with chronic health conditions, including cancer, stroke, and dementia. As the population ages and caregivers become more technologically savvy, Internet-based tools to support caregivers may show even greater promise. While the numerous interventions indicate that online support is feasible, there is still little high-quality evidence to demonstrate effectiveness. Likewise, there is little evidence to specify which intervention components and which platform are most useful. We identified no large-scale, rigorous randomized controlled trials testing the effect of Internet group support on caregiver social support, self-efficacy, or burden. The advantage of meta-analysis is that it allows us to combine the effect of small studies for a more precise estimation of the effect.
Another issue related to online group support involves guidelines for managing groups and the skills required of group facilitators. None of the 10 studies addressed this issue. Little research addresses helpful policies and processes to facilitate Internet group support. While growing evidence supports positive outcomes, the next steps are to build evidence on the most effective methods by which to conduct these groups. Furthermore, it seems likely that the skills required to facilitate an online group are likely different than those for a traditional face-to-face group. Additional evidence is needed to determine the necessary skills for online support group facilitation.
Study Limitations
Given the menu of intervention components in each study, it was not possible to determine the effectiveness of any individual component, only the total effect. Questions on the effect of individual components (e.g., chat, message boards, and so on) cannot be answered in this meta-analysis. Likewise, the studies identified may not be all inclusive, given the initial systematic review inclusion criteria. Finally, the results of this meta-analysis are only as strong as the studies contributing the data. Most of the studies included in our review had moderate risk of bias impacting generalization of findings. In addition, more than half of the studies involved caregivers of individuals with cognitive impairment or dementia creating the potential for selection bias as it is possible that caregivers of those individuals may have unique needs, thus limiting the generalizability.
Conclusions
Internet group support interventions have the potential to be effective at improving social support and self-efficacy in caregivers of adult patients with chronic diseases. Further research using larger, randomized controlled trial studies are needed for wider generalization of results. In addition, studies comparing individual intervention components and online group facilitation practices and processes are essential. Finally, research to identify unique skills required of online group facilitators is necessary.
Footnotes
Disclosure Statement
No competing financial interests exist.