
Abstract

Dear Editors:
We write in regard to the integration of the Walking Tests (WTs) in Telerehabilitation, which today is hampered because of the lack of automation. We discuss the introduction of the WTs in physical medicine and both the challenges and opportunities relevant to their introduction in telerehabilitation. Finally, we present a proposal to eliminate the points of weakness of the WTs in telerehabilitation.
WTs from the Fitness to Rehabilitation
WTs have been widely used in the past decades both to assess fitness and to estimate the metabolic consumption (on the basis of properly designed algorithms compared with gold standard based on several assessed parameters, usually embedding also the heart rate). During the Apollo missions to the moon, astronauts participated in WTs. These tests followed one of the following concepts: • First, a known distance (d) is defined for the exercise and then the time (T) to perform the distance is assessed. • First, a known interval of time (T) to perform the exercise is defined and then the distance (d) is assessed.
A nonexhaustive list of WTs 1 –13 includes the following: (1) one mile test, (2) Cooper test, (3) Six-minute test, (4) Bruce test, and (5) Balke test.
Over the past two decades, the importance of these tests has increased, particularly in sports medicine, which has concentrated its interests in WTs for the assessment of fitness properties both for the athletes and for the subjects with pathologies in several medical sectors. Today, WTs are used in the fitness and in medicine as for example in Sports Medicine and/or Rehabilitation Medicine.
In particular, simple WTs are widely used for the assessment of functional status in patients with cardiorespiratory/pulmonary/neurological disorders. These tests require far less instrumentation than formal cardiopulmonary exercise tests, but they do require standardization of procedures to achieve reproducible results.
How to Improve the Use of WTs in Telerehabilitation
These tests could be useful in telerehabilitation, including the field of cardiology, neurology, and pulmonary rehabilitation. Usually these tests are performed using (1) simple instrumentation such as one chronographer and one heart-rate monitors/recorders and (2) one Tapis roulant.
During these tests, there is a need to manually record information in a medical log. The use of the Tapis roulant, furthermore, shows the following problems that can hamper the outcome: 1. It is impossible to change the rigidity of the soil (important parameter, for example, in fall-risk analysis). 2. It is impossible to modify the trajectories (important parameter in neurology). 3. There is the risk of a false model of walking. Everyone who has used the Tapis roulant is aware that after some trials, it is easy to learn how to expend less energy than in a normal walking path in an open space.
For these reasons, physicians sometimes prefer to perform the WT directly in an open space with a known distance, that is, to perform the test in the so called In the field mode. To allow the use of the WTs in telerehabilitation, there is a need to improve the automation of the procedure and to emulate the In the field mode. Therefore, it is possible to use WTs in a patient's home and transmit data to physicians and/or hospitals and/or Rehabilitation Centre for management and analysis.
The Proposal of a Kit for the WT Monitoring
In previous studies, focused on daily telerehabilitation, a technology has been proposed for monitoring of a defined walking path of a defined distance, 14 or a cascade of walking path with defined lengths. 15 Using this technology, it is, for example, possible to assess the kinematic properties of a performed task at a known distance (time, velocity, etc.) and steps. The technology was based on a central unit, photodetectors, one properly designed step counter, 16,17 and software for the management of the trials. We are further developing technology to design an automatic kit to assess the WTs in the field mode. Figure 1 shows the components of the measuring chain of the kit:
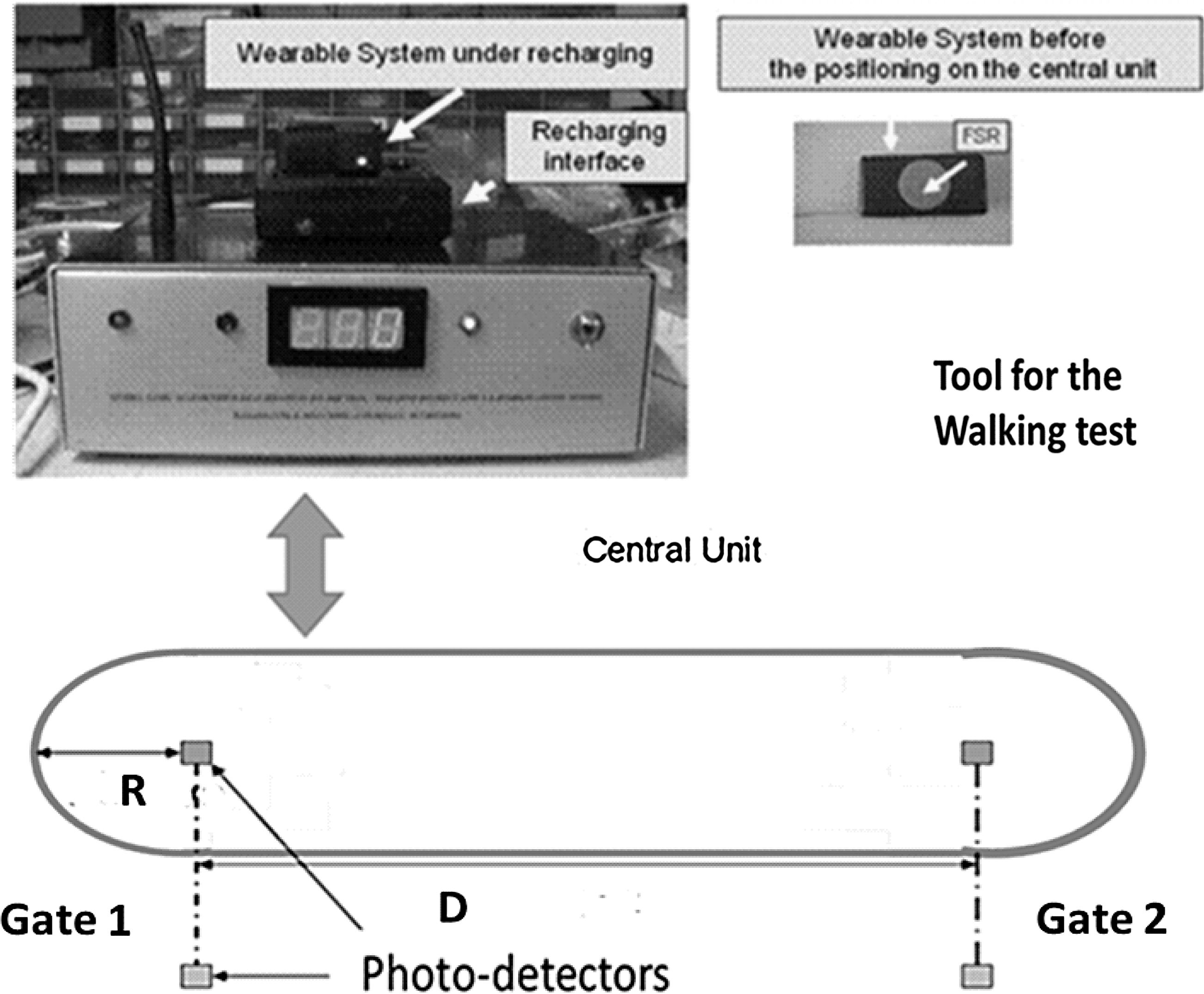
The components of the kit for the walking test.
1. One walking path with curves of radius (R) and one rectilinear path of length (D).
2. Two couples of photodetectors arranged to monitor the crossings of the subjects.
3. One central unit with one step counter, 16,17 connected by means of an A/D converter to the PC.
4. One step counter using the technology described in the literature. 16,17
The kit, on the basis of the two parameters D, R, and the time allows, through the detection of the crossing of Gate 1 and Gate 2, the monitoring of the trials of the WTs.
A prototype of the kit with software based on Labview 8.2 has been reported in the Congress SIAMOC 2012. 18 It allowed the monitoring of the trials, and thus, the selection of the WT and the exchange of the basic parameters.
The Design of the Clinical Tool Associated with the WT
Figure 2 shows the components of the clinical link embedding the kit for the WT.

The clinical link under development.
Currently, we are developing the clinical tool using the software Arduino 1.0.X (IDE).
The clinical tool is modular and in the final version will allow the following: 1. The management of the WT. In particular, the relevant module will permit, in a user-friendly way, the management of the trials and thus the selection of the WT (e.g., one mile test, Six-minute test, and Cooper test) and the exchange of the basic parameters (time, distance, and optional number of steps). 2. The exchange of information of the oxygen saturation assessed by means of the third party medical devices. This parameter generally is very important in many clinical applications, in particular it is basic in clinical monitoring of subjects with the chronic obstructive pulmonary disease both to check the physiological condition and to alert the physicians when it decreases under the defined thresholds. 3. Heart-rate monitoring. This parameter is very important in clinical monitoring both to assess the physiological conditions (as, for example, after stroke or heart failures) and to estimate the metabolic consumption by combining the assessment of the heart rate to the basic parameters obtained by means of the WT and other parameter functions of the subject (weight, height, sex, and age). 4. Direct metabolic monitoring, using third party medical devices. 5. Systolic and diastolic pressure monitoring. This parameter is useful to be monitored as, for example, after stroke or heart failures.
The e-healthcare participants will be able: (a) To check the parameters obtained by means of the WTs and compare them to reference tables that have been proposed in the literature
1
–13
for clinical use to indicate the health state of the subject. (b) To combine the parameters obtained by means of the WTs with the other parameters to obtain further clinical information, as, for example, with the heart rate to estimate the metabolic consumption. (c) To create a more complete clinical record of a subject by combining all the parameters already listed.
1
–5
(d) To create medical knowledge after data mining and data analysis of the parameters stored in step (c).