
Abstract
Introduction:
Telemedicine care models for managing advanced chronic obstructive pulmonary disease (COPD) may benefit from the addition of motion sensing, spirometry, and tablet-based symptom diary tracking.
Methods:
We conducted a feasibility study of telemedicine in the home setting using multiple activity sensor monitoring equipment. Deployment and monitoring were supported by home health nurses with technical advice from the equipment makers as needed. Data analytics for motion sensing was provided by the research sponsor, but was not used for care decisions. On study intake, a health risk assessment, Quality of Life (SF-36) survey, and the St. George Respiratory Questionnaire were administered to assess patients' self-perception of quality of life, activities of daily life function, and difficulty living with COPD.
Results:
Twenty-eight patients were enrolled and data were gathered for a minimum of 6 months and maximum of 9 months. The researchers demonstrated that augmentation of traditional telemedicine methods with motion sensing, spirometry, and symptom diaries appears feasible. The technical, process, logistics barriers, and solutions required for system deployment are described. The researchers demonstrated that augmentation of traditional telemedicine methods with motion sensing, spirometry, and symptom diaries appears feasible.
Conclusions:
Further exploration will be needed to determine the value of this information in preventing outcomes relevant to patients.
Introduction
Chronic obstructive pulmonary disease (COPD) is a major disease in the United States. It is the third leading cause of death 1 and is responsible for large consumption of resources. 2 –5 In addition, exacerbations of COPD can lead to more rapid progression of disease and worsening quality of life.
Monitoring patients who are chronically ill becomes a necessity in early detection and intervention. This is one of a number of chronic diseases that imposes a great burden on the healthcare system. The quality of life of patients with COPD is significantly reduced, creating a unique challenge for healthcare systems, with returned visits for treatment of acute exacerbations. COPD is the third most frequent cause of hospital readmission within 30 days. Beginning in October 2015, Medicare reimbursement was reduced for acute care hospitals whose rates for COPD readmission exceed a predetermined threshold. 6 In light of the potential financial ramifications and to underscore improved patient outcomes, healthcare systems have committed to substantial resources to help develop systems and programs that are designed to reduce readmissions.
It can be exceptionally challenging for clinicians to assure the stability of COPD patients after discharge, especially those in the later stages of the disease. To prevent COPD-related rehospitalization, clinicians need a clear understanding of the root causes that lead to readmission. Several predictors of readmission in clinical studies include prior hospital admission, nonadherence to prescribed oral corticosteroids, use of long-term oxygen therapy, poor health-related quality of life, and a lack of routine physical exercise. 7
With the prevalence of home telemonitoring programs and systems available, it becomes more evident that clinicians need to understand how to use the tools provided and how the technology can impact care for patients. Reviewing current literature on home health monitoring clearly indicates that a number of studies have been dedicated to comprehending and implementing such rollouts.
Telemedicine has made major impacts in various areas of healthcare and is rapidly expanding across multiple healthcare settings. Outstanding outcomes have been observed, including remote ICU programs, 8 –11 remote surgical operations, 12 –16 and direct consultations with patients at home. 17 –21 The impact on chronic disease has been mixed, with some studies suggesting positive impact 22 and others unable to demonstrate differences. 23 Interpreting the literature can be difficult because of significant variability because of rapid improvements in monitoring and communications technology, the type of monitoring studied, the disease entity and severity studied, and variations in the process of care brought about by the telemedicine intervention.
Integrating telemedicine into practice has allowed clinicians to intervene earlier and prevent complications, 24 but can create the challenges of alarm frequency and response if not implemented with workflow impact addressed up front. The transmission of the data to the healthcare team, although straightforward in theory, can be impacted by cellular access issues in rural areas. It is critical, in planning a telemedicine implementation, that the data flow and workflows in response to the data are all designed up front.
Previous COPD home monitoring studies gathered various vital signs and identified some symptoms tracking, 12 but have not used spirometry, motion sensing, or activity sensors worn by the patient. Spirometry has been used to track the progress of COPD over time, 25 –28 and to identify acute exacerbations. 29 Although peak flows have been used in asthma for home detection of exacerbations, 30 –33 few studies have attempted to deploy spirometry in the home monitoring of COPD. 34 This research was designed to integrate spirometry transmitted to a tablet device, which, in turn, transmits to the monitoring center (Fig. 1).
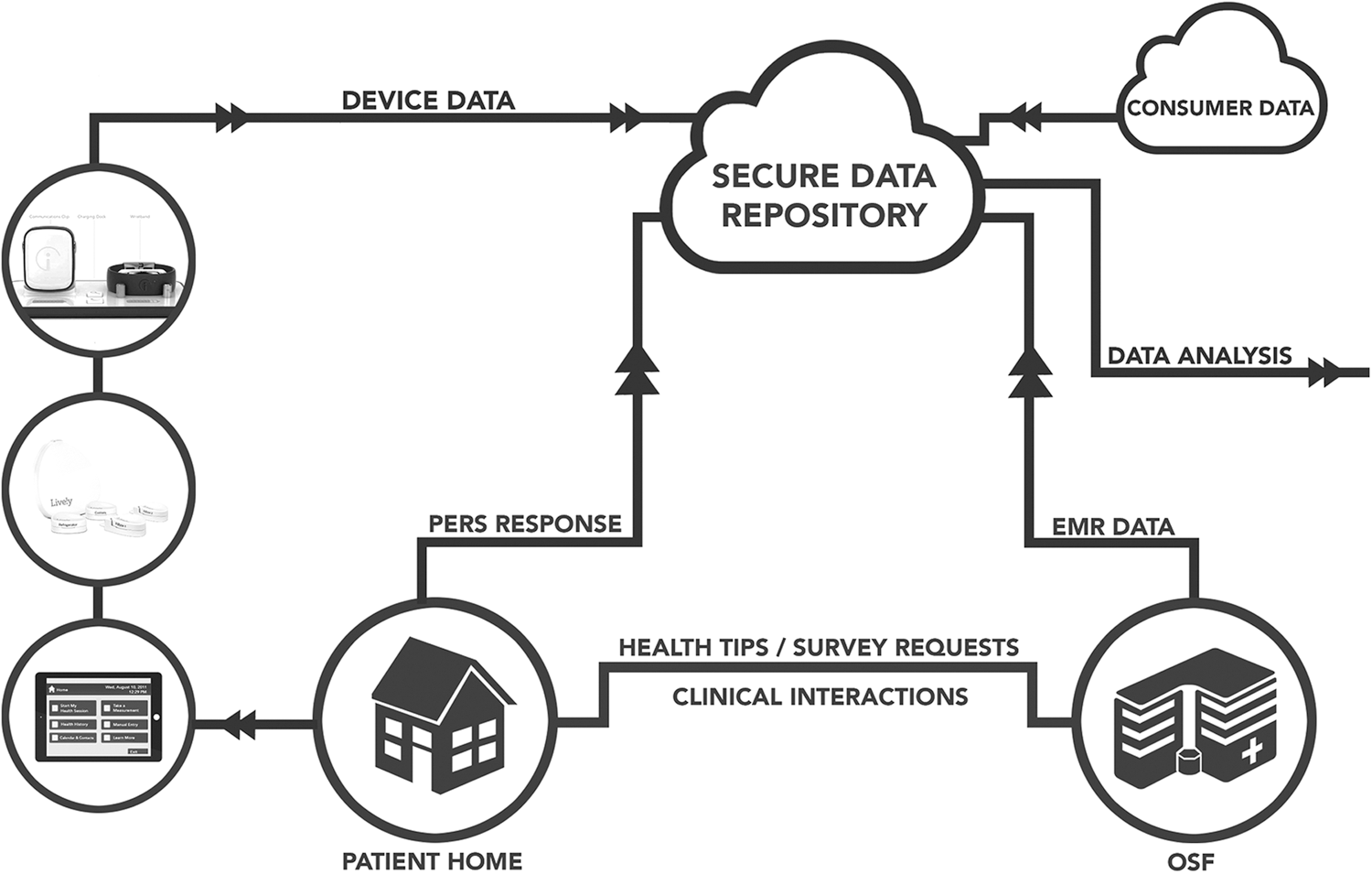
Data flow diagram.
Motion sensing has been a recent addition to the monitoring paradigm, having followed small motion sensors used for other purposes. Health applications for motion sensing have included sensors embedded in the home environment that are transmitted to the distributed data server and are available using a Web browser or visual program. The user received event messages through e-mail or mobile phone. 35 Motion sensing for home monitoring in the setting of advanced chronic disease in general has not yet been studied.
The larger project goal is to determine patient outcomes after monitoring patients for an extended period. The researchers hypothesize that home monitoring can improve care management programs by further reducing hospitalizations and emergency department (ED) visits, limiting exacerbations of COPD and improving costs and quality of life in patients with COPD.
Before this study could be conducted, the research team had to overcome technical, logistical, response coordination, and patient factors to deploy equipment in the home. Therefore, this study assessed the feasibility and acceptance of placing multiple home device sensors in patients with GOLD stage 3 or 4 COPD (as defined by the Gold Standard, reference
Methods
The first stage of development for this pilot study included an in-house evaluation/utilization of vital sign captures and activities of daily life (ADL) sensor data as early indicators of detrimental changes in home patient health. Although each device had been previously tested and, to some degree, marketed, all were relatively new and they had not been tested together as one monitoring solution.
The evaluation took place in the simulated home setting at Jump Simulation and Education Center in Peoria, Illinois. The home setting and a standard patient actor representative of the target population were used for evaluation of ease of setup, consent, workflow, and recommendation for sensor use and responses. Specific recommendations for monitoring parameters in the COPD population were made by the principal investigator (W.T.), who is a pulmonary critical care physician. A peak flow meter and home spirometry, pulse oximeter, and individually identifiable activity tracker were added to the daily measurements and customized questions related to exacerbations of COPD symptoms. A full list of recommendations and updates was provided to Intel-GE Care Innovations™ for implementation before protocol development. Since peak flow meters do not perform well in the COPD population, home spirometry was chosen knowing the difficulty in use in the home setting.
This study was approved by the Peoria Institutional Review Board (PIRB; Internal No. 649795), pursuant to 45 Code of Federal Regulations (CFR) 46.111 and 21 CFR 56.111 under expedited criteria. Written consent was obtained from each prospective subject.
After enrollment, the research team corrected technology issues, whereas the home health telemedicine team supported deployment and clinical response. This team included pulmonary clinic nurses, home health nurses, the research team, and the lead investigator pulmonologist. The research team developed detailed setup, registration, and installation procedures after testing and evaluation of the setup process in a simulated environment with a standardized participant (representative of the population of patients with COPD). The research team developed registration instructions for each piece of equipment and corresponding survey instrument. A series of equipment tests were performed to ensure that registration and connectivity were functioning properly, including testing each peripheral.
The following equipment was deployed: 1. Activity sensors: The activity sensor provides passive motion-sensing technology detecting patterns in ADL. It comprises a communications hub and several sensors that are placed on objects within the home. The hub captures motion signals from the sensors and transmits them through 2G cellular coverage (Fig. 2).
The ADL sensor software determines activity patterns associated with areas that included refrigerator, kitchen drawer, key fob, pillbox, and nebulizers (as applicable), where medications, food and drink, bathroom, and other areas are accessed. 2. Remote care management system: Patients were supplied with a remote care management (RCM) system, which used a tablet-computing device provided by Care Innovations. The computer tablet enables vital signs (blood pressure, weight, pulse oxygen, and peak flow) and a series of questions related to COPD symptoms (wheezing, cough, and mucus production). A blood pressure cuff was provided and manual entry was taken by the patient. Both the pulse oximeter and scale measurements were obtained and transmitted wirelessly through Bluetooth. Specific, validated protocols were used and configured by the principal investigator for COPD patients. The computer tablet prompted patients daily to take regularly scheduled health sessions, data were then transmitted to a secured database where clinicians accessed conditions through a Web-based application. Thresholds were set per patient, and when conditions outside of those parameters were met, clinicians would contact patients directly to obtain more information. Any clinically significant alerts were then managed by the principal investigator (Fig. 3). 3. Body-worn activity sensor device: Recognizing the limitations of the general sensor activity, an additional body-worn sensor device was used to allow gathering of information about individual patients. A mobile personal emergency response system was used and response patterns were not part of this study, but because this system was designed with emergency response in mind, we believed it was ethically responsible to activate the system. The wristband includes an accelerometer, which monitors activity. Activity data were transmitted to a backend database, wherein researchers can retrieve and combine these data with other study data (Fig. 4). 4. Health risk assessment and surveys: A Health Risk Assessment and Survey tool was used to gather additional relevant patient information at the start and end of the study. Also, other survey tools known as the Short Form Quality of Life (SF-36) and St. George Respiratory Questionnaire were administered to assess patients' self-perception of quality of life, ADL function, and difficulty living with COPD. All questionnaires were completed at the beginning of the study and end of participation.

Activity sensors.

Remote care management system.
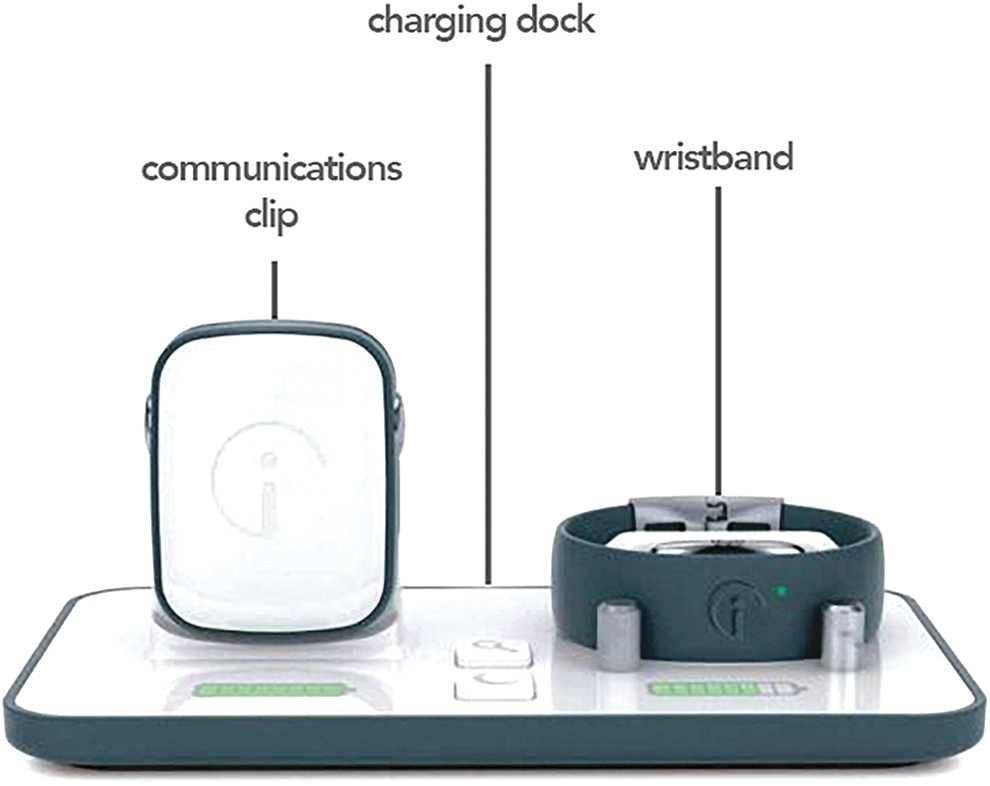
Body-worn activity sensor.
Deployment Protocol
Research teams registered patients in each of the four electronic device registrations. Installation and user guides for each technology included labeled photographs and written instruction used by all teams and patients during setup. All equipment was tested before deployment to the patient's home. Home health aides were provided training on setup and installation as well as individual checklists, decision trees, and troubleshooting information.
Monitoring Protocol
Patient selection was based on the most critically ill COPD patients (stage 3 or 4) to ensure that home health monitoring was necessitated, and also, to help demonstrate effectiveness of adopting this equipment in a group most likely to benefit from implementation. Each day, RCM systems would alarm the patients (individualized for patient preference) that they were due to take their daily measurements. The RCM system would walk the patient through the basic daily questions for COPD and then each measurement would be taken in sequential order. Individualized patient parameters were set to trigger alarms when data fell out of expected range per patient. Home health nurses provided support daily for initial assessment/inquiry on status, monitoring activity, compliance, and general troubleshooting with daily measurements.
The entire team, which included telemedicine nurses, home health nurses, an emergency physician, and a pulmonary critical care physician, created and modified the alert criteria based on literature review. These alert criteria were later refined based on team review of data, alerts, and the significance of the alerts. Alerts were modified to fit patient dynamics. For example, if a patient's baseline pulse was historically low, the parameter would be adjusted by the pulmonologist (Table 1).
Subject Characteristics and Vital Readings
COPD, chronic obstructive pulmonary disease.
Support Calls
Patients were instructed to call an 800 number for technical issues. Five subject phone logs were reviewed for the pilot period of 6 months for trends in support. The first five subjects were selected based on length of time in the study. On average, subjects were contacted 23 times for alerts. Five percent of calls resulted in clinically significant actions (i.e., clinic follow-up visit, ED visit, or change in medication or therapy). Other phone calls resulted in nonsignificant alerts such as irregular blood pressure, abnormal peak flow readings, or faulty use of peripherals that were corrected over the phone or referred to the patient's primary pulmonologist without intervention.
Results
The researchers were able to deploy home monitoring equipment for 28 advanced stage COPD patients. Each subject was monitored for a period of up to 6 months and a maximum of 9 months. With regard to technical challenges to initial deployment, issues were collected and resolved. The broader approach was to overcome technical, logistic, patient, and process issues as demonstrated in Table 2.
Technical Barriers to Implementation
≈ USB connections
□ Inaccurate readings/device malfunctions
€ Inconsistent data transfer
¥ Inefficient battery usage
≠ Step-dependent process
∞ Registration system difficulties
⌂ Lack of streamlined support
◊ Limited to participants with cellular coverage
∑ Triggered false alerts to home health teams
∂ Noted as physically uncomfortable for participant
⊠ Technical support not available in CST time zone
Motion Sensor Activity Example
Behavioral patterns were obtained for Patient 8. Although there were some gaps in the data collected, Link Mobile data were collected throughout the period of time being evaluated.
Figures 5 and 6 are graphical representations of Patient 8 for 1 month. These are 24-h radial charts for the average activity, by sensor, for the course of 1 month.

Hourly activity, Patient 8.
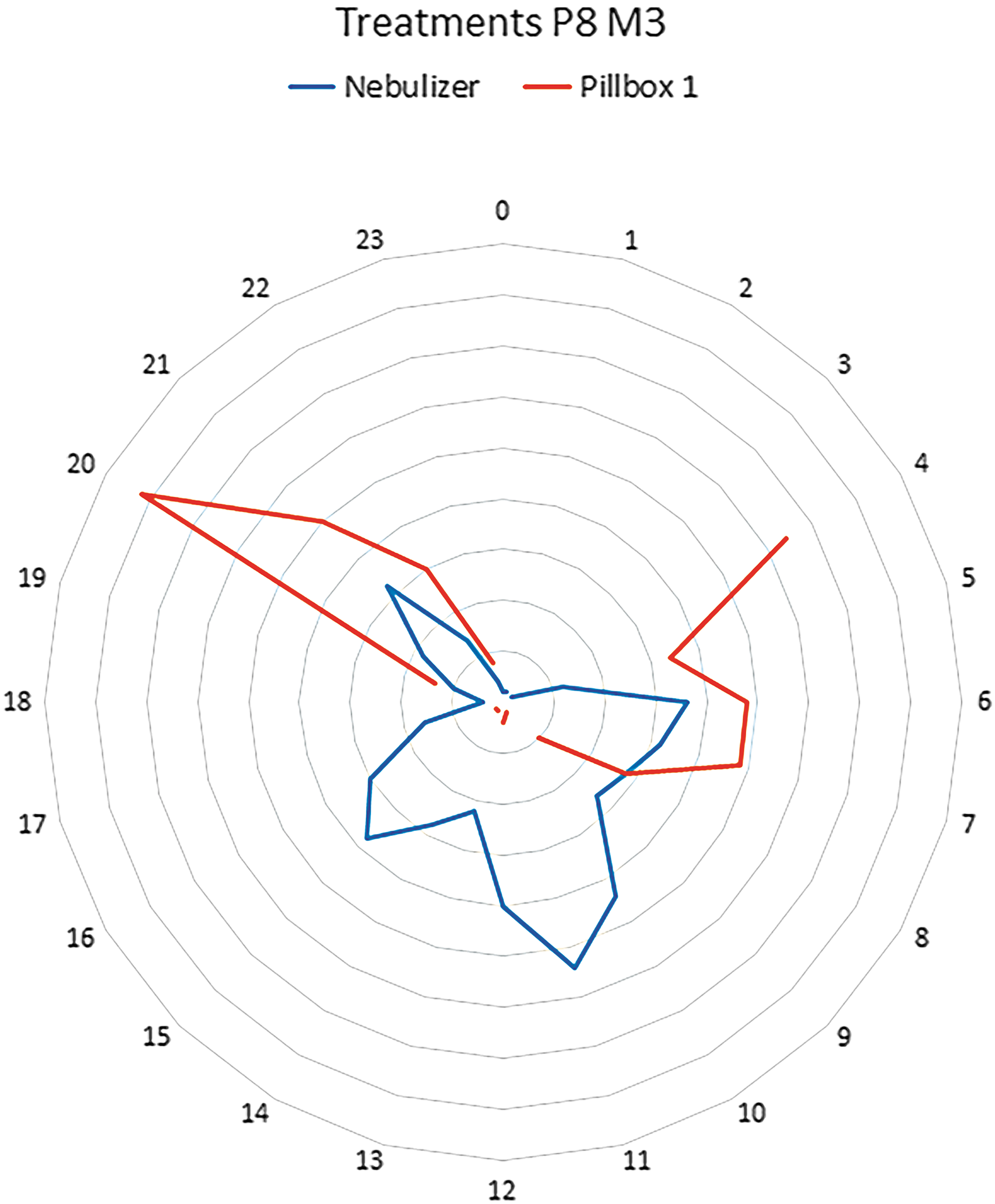
Treatments, Patient 8.
The highlights of information discovered include the following descriptions: • The top of each chart represents midnight and each hour of the day is represented by 0–23. • The blue line in Figure 5 on the left represents consistency in bathroom use between 6 am–7 am and 7 pm–8 pm. The orange line represents awake time at 5 am and bedtime between 8 and 10 pm. The gray line represents refrigerator activity between 5 and 6 am, at 11 am, between 5:30 and 6 pm, and around 9:30 pm. • The blue line in Figure 6 on the right represents nebulizer use. Most likely used at 11 am but also likely used at 5 am (when the patient first gets up), at 5:30 (before dinner), and at 9:30 pm. Orange line represents medication use at 4 am, between 6 and 7 am, and at 8 pm.
Figure 7 illustrates the average readings per day by sensor for Patient 8 during month 3.
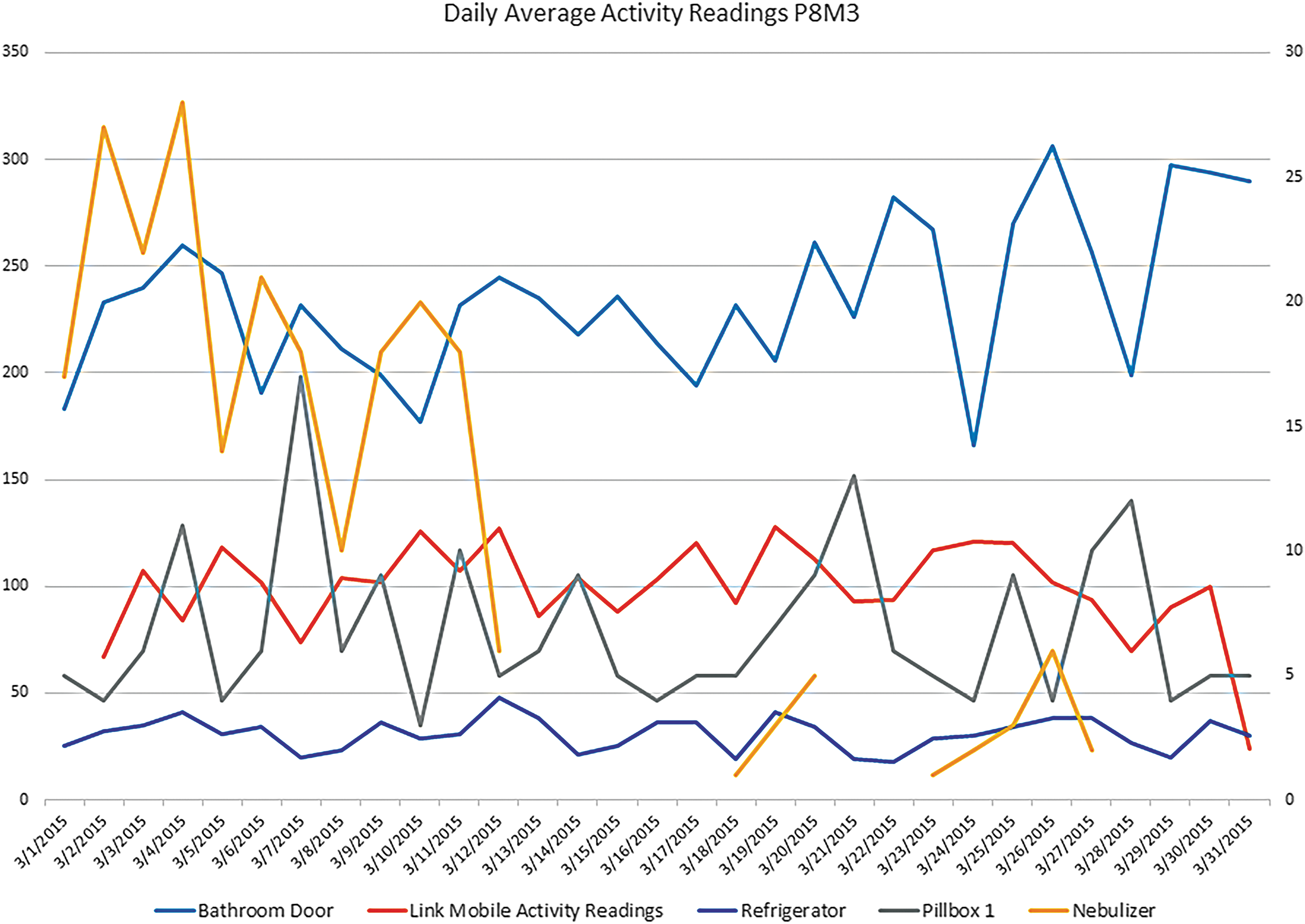
Daily average activity readings, Patient 8.
Patients were provided a patient satisfaction survey at the end of their participation related to comfort levels and ease of daily vital measurements, and results are presented in Table 3.
Patient Satisfaction Survey
The results are also largely qualitative because of the small sample size (n = 24), but do reveal some early patterns for understanding patient attitudes toward telemedicine.
Conclusions
Our assessments of the results of the study primarily indicate an algorithm of ADL in a chronically ill population that may bridge to earlier intervention. This study demonstrated some key themes for implementation of telemedicine, including (1) the need for detailed instructions, (2) active participation among teams, (3) clear communication, (4) patient value assessment, and (5) a system for feedback. By tracking these patterns, one would conclude that the ability to identify divergent patterns is possible—providing insight into a potential change in a patient's health status. This study showed that combining multiple pieces of sensory equipment resulted in the need for significant adjustments to work instructions for the research and home health teams. Training on the equipment improved the comfort level of all teams to interact and troubleshoot with patients. Items such as location of buttons to turn on/off the devices, how to properly place a rechargeable piece, and equipment issue numbers were all included in a summarized manner for the patient. All survey participants responded “Strongly Agree” or “Agree,” addressing patient comfort with the telemedicine devices used in the study. Survey response data suggest that although patients were comfortable and accepted the technology in their homes, they failed to see a direct impact to their health. It will be important to develop a patient value proposition for telemedicine participation and to evaluate whether lack of perceived improvement of patient health affects a patient's long-term willingness to participate in telemedicine.
Communication among all team members and timeliness of response proved critical to the adoption of the program. Project planning efforts set expectations across multiple departments and pre-empted many barriers before implementation. Early meetings with stakeholders including telemedicine, pulmonary, home health, and research proved efficient for support and streamlining. We chose to send equipment with experienced home health aides rather than sending patients home with equipment and instructions.
Alert parameters must be sophisticated enough to detect a true change in health status when combined with other sensor data that requires clinical intervention. The alarm response represented a significant work burden by the monitoring nurses. As home telemedicine grows, the alert configurations must be standardized and highly sensitive to prevent alert fatigue. Sensitivity of alarms in many areas of medicine clearly represents human factor challenges. 36 These will aggregate to concerns that have policy implications for covering the cost of monitoring weighed against the costs of visits or admissions prevented.
From a technology standpoint, this pilot study gathered passive motion sensing and active body-worn sensor movement data. Both passive and active sensor methods face technical problems if there is more than one person in the home—the nonpatient individuals are also triggering the motion sensor, making it impossible to differentiate activity patterns between individuals. This can be overcome by adding a worn sensor, but eventually inferred data analysis will be able to characterize which individual is moving. 37
Telespirometry has been piloted in postlung transplant patients. 38 Some data suggest that spirometry results taken in general offices may differ slightly from those taken in pulmonary offices. 28,39 Likewise, it is presumed that some of the spirometry results done by unobserved patients in the home may also be invalid. Some of the pilot readings were clearly outside of an acceptable range for a stable state patient, and these have to be discounted. However, the benefit of home monitoring affords the opportunity to study trends as never before, and therefore, this is a limitation the researchers feel is worth accepting. The planned future randomized study of monitoring will attempt to determine the marginal value of these data, as well as compliance in a larger sample.
The researchers were able to overcome technical, logistical, and patient factors to deploy home monitoring equipment for patients with advanced stage COPD. Execution of the project required support from both telemedicine and home nursing, with refinement of an alert and response system. There are directional analytical relationships emerging from this study, which are providing insight into symptom changes through the integration of data from activity sensors, patient inputs, objective measures, and with clinical records. Positive feedback was received from study participants and clinical staff, prompting us to pursue future studies to measure the impact of monitoring on patient outcomes and resource utilization.
Footnotes
Acknowledgments
We would like to thank the following individuals for their contribution to this research study and for supporting this effort: Mindy Johnson, Kim Gleichman, Beverly Glidewell, Maria Herlihy, Maureen Glynn, Mounika Paravastu, Justine Milligan, Joe Gatuz, Connor Schuler, Julie Cheitlin Cherry, Alexandra Conley, Kathy Mayberry, and Kim Borge, and all the pulmonary physicians and nurses for their support on this project. This study was sponsored by Intel-GE Care Innovations™, a remote care management solutions provider, which provided FCC-cleared and FDA-listed devices for evaluation. As a non-FDA regulated trial, the study was not required or recommended for registration with
Disclosure Statement
No competing financial interests exist.