
Abstract
Background:
Digital inclinometer applications using data from embedded sensors on smartphone/multi-purpose pocket computers or “smart digital inclinometers” (SDIs) are now used to clinically assess range of motion (ROM).
Objectives:
The objectives of this study were to assess, compared with a biomechanical gold standard (GS), the trueness and minimal detectable change (MDC) of shoulder range of motion (SROM) measurements obtained from an SDI.
Methods:
Twenty-five (n = 25) asymptomatic healthy participants performed three trials of shoulder flexion (SF), shoulder abduction (SA), and shoulder external rotation (SER) at full-range and mid-range.
Main Outcome Measures:
SROM was measured concurrently from sensor data (pitch, yaw, roll angles) from an iPod Touch installed on the posterior aspect of the humerus and 3D orientation of the upper arm obtained from an optical motion tracking system GS.
Results:
The mean level of bias between SDI and the GS across all SROM measurements was 3.4°, with a 95% confidence interval varying between −8.9° and 15.8°. The mean and standard deviation absolute difference of SDI measurements with the GS were 5.8° ± 3.7° for SF, 8.7° ± 5.2° for SA, and 1.7° ± 1.4° for SER. The trueness of these values varied according to the movement. MDC was 1.9° for SF, 2° for SA, and 0.3° for SER.
Conclusions:
SROM measures in SER with an SDI seem to be accurate and robust for clinical use. However, SROM measures in other planes of motion should be interpreted with caution depending on the evaluation objective, the plane of motion assessed, and the range of ROM measured.
Introduction
Recently, the wide availability of smartphones and multi-purpose pocket computers (e.g., iPod) embedded with inertial sensors has fuelled the emergence of digital inclinometer applications. These applications, or “smart digital inclinometers” (SDIs), are used clinically to assess range of motion (ROM). 1,2 Although studies have shown that SDI are equal to, if not more reliable than standard goniometers (SG) for ROM measures at different joints, 3 –8 their trueness has not been rigorously studied. Trueness is essential to the validity of a measure and refers to the closeness of agreement between the average value obtained from a large series of test results and an accepted reference value (i.e., gold standard [GS]). 9 Optical motion capture systems typically used in biomechanical laboratories are considered the GS for assessing the kinematics of motion. No studies have looked at the trueness of shoulder range of motion (SROM) measurements with SDI. The objectives of this study were to assess, using an optical motion capture system as a GS, the trueness and minimal detectable change (MDC) of SROM measurements from an SDI.
Methods
The study was approved by the CIUSSS–CHUS Ethics Review Board. SROM measurements were performed by one trained individual using a standardized protocol in the biomechanical laboratory of the Research Centre on Aging. A sample of 25 asymptomatic healthy participants (12 men and 13 women, mean age: 30.92 ± 10.05; mean height: 1.70 ± 0.08 m; mean weight: 75.04 ± 15.86 kg) was recruited. Participants were seated on a chair and asked to successively complete, at full-range (FR) and mid-range (MR), three trials of shoulder flexion (SF), shoulder abduction (SA), and shoulder external rotation (SER). For each trial, they were instructed to start from an anatomical resting position and move to either FR or MR. Once at M/FR, the position was maintained and measurements were taken.
Participants were instrumented with an armband positioned on the middle third of the participant's dominant arm on the posterior aspect (triceps) for SF and SA measures (Fig. 1A) and on the anterior portion of the forearm for the SER measures (Fig. 1B). The armband contained a fifth generation iPod touch with an embedded gyroscope program called Gyroscope (11), which measured the relative rotation of the device over time in three axes (Pitch, Yaw, and Roll [PYR]). PYR orientation values at the starting position and at the final position were extracted visually from the interface of the software application, consigned to the experiment's log book by the assessor, and converted into quaternions (a quaternion is an angle-axis representation of the attitude of a rigid body). Quaternion differences between initial and final positions were computed as SROM for motions performed in SF, SA, and SER. A second armband containing a rigid body with four active markers was positioned distally from the iPod touch armband on the bottom third of the posterolateral aspect of the humerus (Fig. 1). The 3D orientation of the upper limb from the starting position to the final position was captured by tracking the rigid body in space using an optical motion tracking system (Optotrak®) with four camera towers. The 3D orientation of the rigid body attached to the participant was extracted as quaternions, relative to the fixed laboratory coordinate system. SROM in SF, SA, and SER from the optical motion tracking system was computed as differences in quaternions between initial and final positions and considered as the GS of SROM.
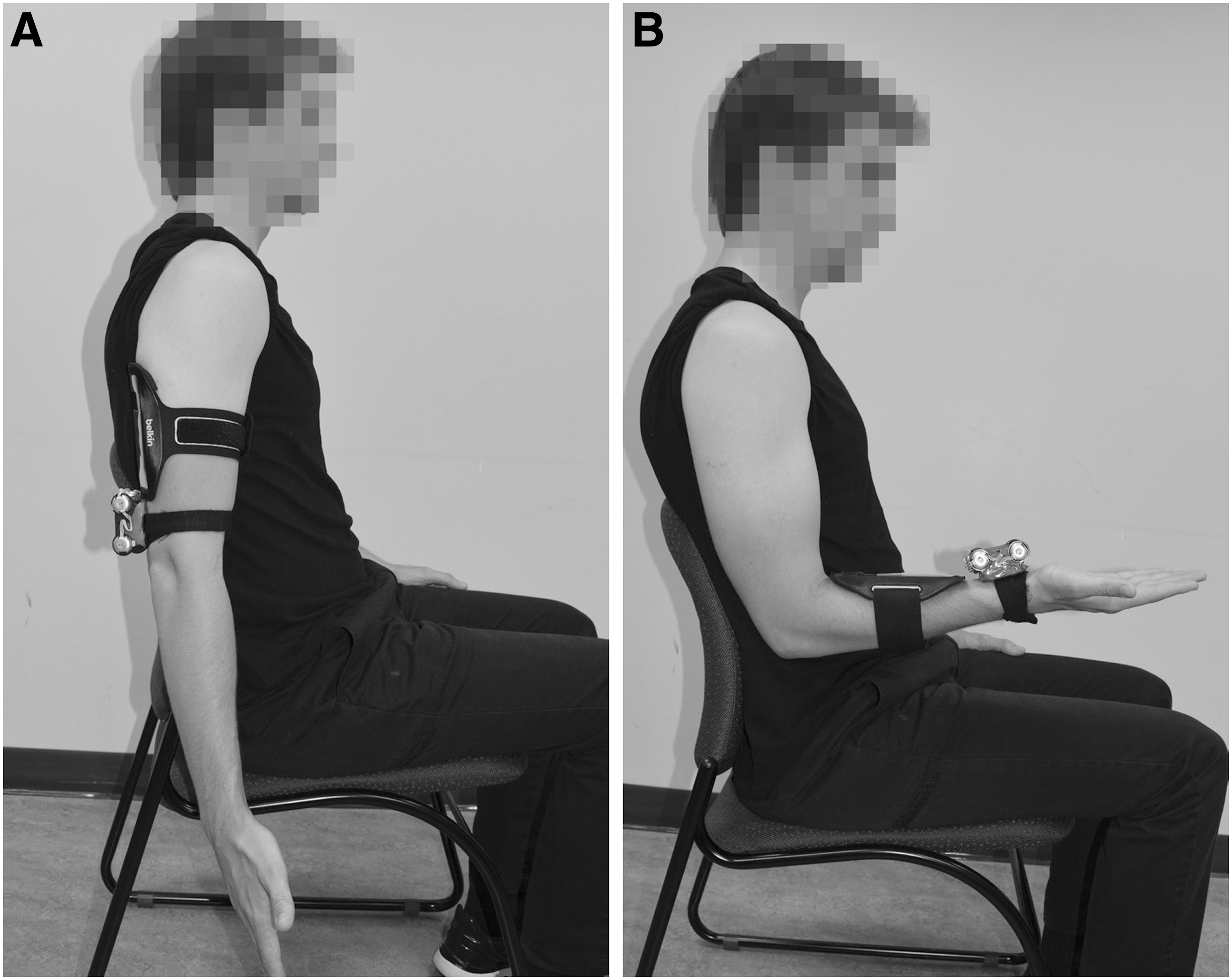
Experimental setup and measurements systems.
Mean level of agreement and 95% confidence interval (CI) between the GS and the SDI SROM values were computed by using Bland-Altman. The mean and standard deviation absolute difference of SDI measures with the GS in degrees were computed for each plane of motion for all data and per ROM (MR, FR). The minimal detectable change (MDC) SROM from single-axis or multi-axis sensor data was computed by using the following formula:
with r computed between values from the GS SROM and SROM values from the SDI. An ANOVA was used to assess differences in trueness with the GS measures according to planes of motion (SF, SA, and SER).
Results
Figure 2 presents a Bland-Altman plot comparing ROM values computed from the GS with ROM computed from the SDI for all measures. The mean level of bias between SDI and the GS across all SROM measures was 3.4°, with a range of 27.7° (95% CI −8.9° to 15.8°). Mean absolute difference per plane of motion for each ROM (MR and FR) and for all measures (combined) between SDI SROM and GS SROM, Pearson's r coefficient, and MDC values are shown in Table 1. The trueness of the SDI was significantly different depending on the plane of motion measured (p < 0.001, Welch's F). Trueness of SER was significantly better than SF and SA, whereas trueness of SF was significantly better then SA (p < 0.001, Games-Howell post hoc). MDC values were all below 2° (1.9° for SF, 2° for SA, and 0.3° for SER). Differences in trueness were observed, and statistical differences in trueness for a given plane of motion varied according to the ROM (MR or FR) measured (p < 0.001, Welch's F).
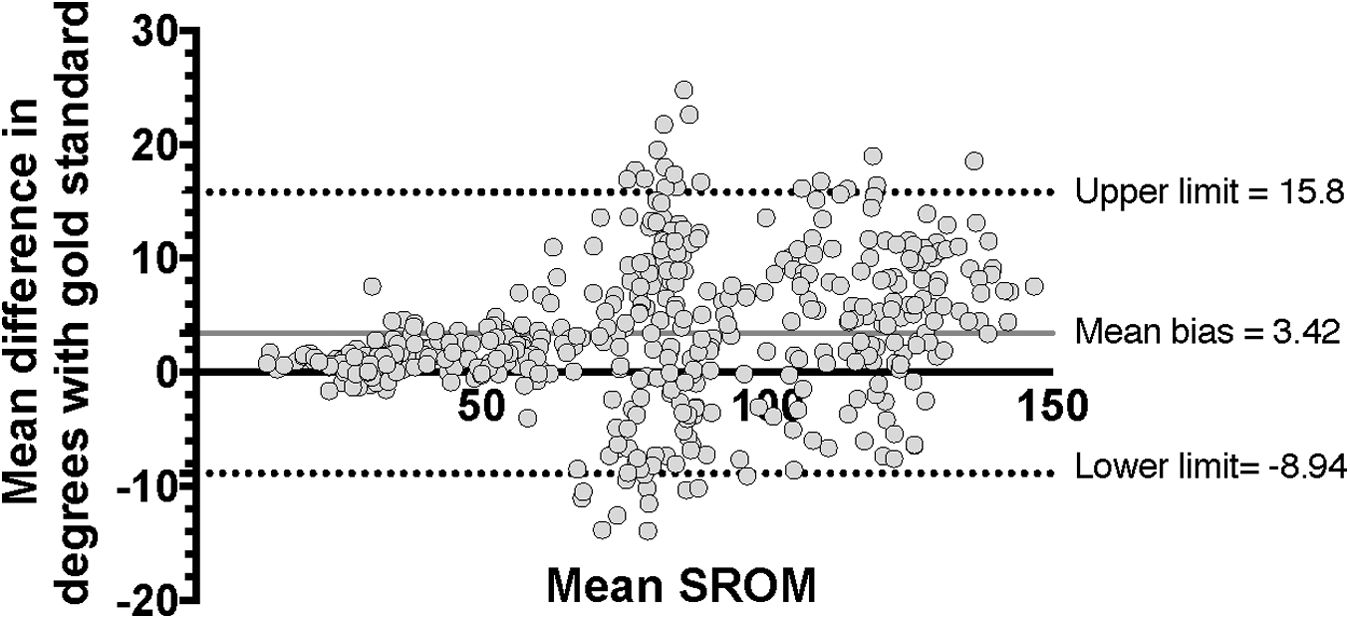
Mean difference values of smart digital inclinometer with optical motion capture gold standard. Full line is the mean bias. Ninety-five percent confidence intervals are reported as dotted lines. SROM, shoulder range of motion.
Mean Absolute Difference, Correlation and Minimal Detectable Change of Smart Digital Inclinometer with Optical Motion Capture Gold Standard
All, all measures of SROM; Mid, measures of SROM performed from starting position to mid-range of plane of motion; full, measures of SROM performed from starting position to angle > then mid-range of plane of motion.
MDC, minimal detectable change; SA, shoulder abduction; SD, standard deviation; SDI, smart digital inclinometer; SER, shoulder external rotation; SF, shoulder flexion; SROM, shoulder range of motion.
Discussion
Although the trueness for SDI SROM measurements appears acceptable (mean bias of 3.4° with GS), the range of the upper and lower limit of the 95% CI shows that it can be highly variable (−8.9° to 15.8°, range of 27°). That variability seems to mainly be driven by flexion and abduction results. The mean levels of agreement and 95% CI reported between GS and SDI ROM measures in three previous published studies tended to vary with the ROM measured and the GS criteria. Hambly et al. reported a range of 7.01° (−2.13°/+4.88°) for maximum active knee flexion (120°–145°) with an SG. 10 Ockendon and Gilbert reported a range of 15.2° (−8°/+7.2°) for knee flexion between 5° and 45° with SG. 4 Vohralik et al. reported a range of 2.8° difference for measurements of static angles from 20 pieces of timber between a digital inclinometer application and a magnetic motion tracking system. 7
The divergence in our results and others can be explained partially by the choice of the GS and the conditions of measures. These studies used SG and measured angles under constrained conditions at restricted ROM of the knee in one plane of motion or under artificial conditions. We used an optical motion capture system with a better resolution but also measured ROM in three planes of motion at mid and full ROMs. Since no studies have demonstrated the trueness of the SG with an optical motion capture system, comparisons are difficult to make. The other factor that might explain the high variability seen in SF and SA compared with SER might be related to the positioning of the instruments.
Although there is no clinically established acceptable level of trueness for measures of SROM, it can be speculated that to be able to ascertain SROM limitations and follow clinical evolution in SROM after an intervention, measures with a difference of more than 5° from a recognized GS of ROM have limited application clinically or at least should be interpreted with caution. Overall, SROM measured with the SDI in SER seem to be the truest and most robust, with mean differences and standard deviation below this 5°. The trueness for SF and SA measurements were not only above this threshold but also highly variable and affected by the ROM measured. Although the impact of the ROM measured on the trueness of SDI was statistically significant for all planes of motion with a mean difference varying between 0.2° and 1.7°, one could wonder about the clinical significance of this difference.
These disparities can be explained partly due to the assumption that sensors in the device are aligned orthogonally with the axis of motion and that this motion performed is pure (only in this axis) when using an SDI. Although this may be true for an articulation with a single degree of liberty such as the knee, the placement of the device on the upper arm and the motion performed by the shoulder joint (with 3° of liberty) in SF and SA have a potentially confounding effect on the trueness of the SROM measurements. To mitigate these impacts, quaternions were computed based on the recorded PYR values whereas ROM was evaluated as the global change in orientation computed from the difference between the quaternions at initial and final conditions. This approach unfortunately does not take into account possible errors induced by the SDI application algorithm when decomposing the motion into such PYR (e.g., mathematical error due to gimbal lock). A direct access to a quaternion-based orientation estimation algorithm would certainly make SROM measurement more robust.
In conclusion, SROM values computed from SDI applications should be interpreted with caution depending on objectives of the evaluation assessment, the plane of motion assessed, and the range of ROM measured.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of Kelly Bradbury to the revision of the article and Antoine Guillerand for the data collection and outcomes extraction. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' Contributions
P. B. conceived, designed the experiment, analyzed the data, and wrote the article. S.D.F. conceived, designed the experiment, collected and analyzed the data, and wrote and reviewed the article. K. L. conceived and designed the experiment, analyzed the data, and reviewed the article. M. B. collected and analyzed the data and reviewed the article. F. B. conceived, designed the experiment, and reviewed the article. Y.T.L. conceived, designed the experiment, and reviewed the article.
Disclosure Statement
No competing financial interests exist.