
Abstract
Background:
Insomnia is a common complaint of individuals presenting to healthcare providers and is associated with decreased quality of life and higher healthcare utilization. In-person cognitive behavioral therapy (CBT) is an effective treatment for insomnia but is hindered by cost and limited access to treatment. Initial research suggests that Web-based CBT may mitigate these obstacles.
Introduction:
This study tests the effectiveness of a Web-based program for insomnia based on principles of CBT and stress management.
Materials and Methods:
We conducted a randomized trial with wait-list controls among adults with primary insomnia (n = 88). Two hundred sixty-three adults with comorbid insomnia were also included and analyzed separately. The intervention was a 6-week online program, and effectiveness was measured via the Insomnia Severity Index (ISI).
Results:
Baseline ISI score for the intervention group (n = 43) was 17.0; 16.6 for the control group (n = 45). At first follow-up, the intervention group (n = 25) had a mean change from baseline of −7.3 (95% CI: −9.0, −5.6), sustained through second follow-up, while the control group (n = 35) had a change of −1.3 (−2.7, 0.1). The between-group difference was statistically significant (p < 0.001). Participants in the comorbid insomnia group had a baseline ISI score of 16.7 with improvement similar to the primary insomnia group (−6.9; −7.6, −6.2).
Discussion:
We observed clinically meaningful improvements in insomnia severity in adults with primary or comorbid insomnia. Sustained improvement over 4 months underscores the effectiveness of a well-constructed online CBT for insomnia program.
Conclusions:
Go! to Sleep© offers a potentially effective treatment option for adults with insomnia by eliminating geographical barriers to care.
Introduction
Approximately 10–30% of the adult population is affected by insomnia, either a primary sleep disorder or one comorbid with medical, psychiatric, or other sleep conditions. 1 –7 Chronic insomnia reduces quality of life and is tied to higher healthcare utilization and healthcare costs. 5,7 –9 Insomnia is frequently associated with fatigue, irritability, depressed mood, and difficulty concentrating, and untreated insomnia elevates the risk for chronic pain and other conditions such as hypertension, diabetes, and cardiovascular disease. 7
Insomnia is predominantly managed with hypnotics and other medications despite the effectiveness of and patient preference for cognitive behavioral therapy for insomnia (CBT-i). 10 –12 Web-based CBT-i is a practical alternative to in-person CBT-i and can mitigate obstacles to in-person versions including cost, a scarcity of trained clinicians, and inaccessibility to treatment. Web-based CBT-i provides self-management solutions to help individuals learn psychological and behavioral techniques that improve sleep quality and decrease insomnia symptoms. Success of such programs is demonstrated by improvements in daytime functioning and sleep efficiency and decreased insomnia severity scores. 13 –18
We developed a 6-week Web-based program, “Go! to Sleep©” (GTS) to provide accessible and comprehensive insomnia care to employees and patients within the Cleveland Clinic Healthcare System. GTS incorporates a stepped-care approach to be used by primary care providers, allowing them to treat as many insomnia patients as possible with the least intensive treatment needed to achieve clinically significant outcomes, reserving more intensive resources for those who require enhanced care. 19,20
We evaluated GTS efficacy through a randomized controlled trial targeting adults with primary insomnia (i.e., without comorbid illness). Due to its increased prevalence relative to primary insomnia, we also included a concurrent confirmatory effectiveness test sample among individuals with comorbid insomnia.
Materials and Methods
Study Design
The first study was a two-arm, parallel, randomized control trial (Fig. 1) with the primary aim to assess the impact of GTS on improving insomnia symptoms, as measured by the Insomnia Severity Index (ISI), by comparing active treatment with GTS to wait-list control and a secondary aim to assess the impact of GTS on sleep efficiency and total sleep time (TST) collected from daily sleep logs. Once eligibility was confirmed at baseline, patients were randomized in a 1:1 ratio to intervention or wait-list control, with the latter group given the option to obtain the program for free after study participation. The second study (Fig. 1) was an observational, nonrandomized, treatment-only confirmatory effectiveness test sample that enrolled participants excluded from the randomized trial due to comorbid conditions but otherwise with identical primary and secondary aims as the main study.
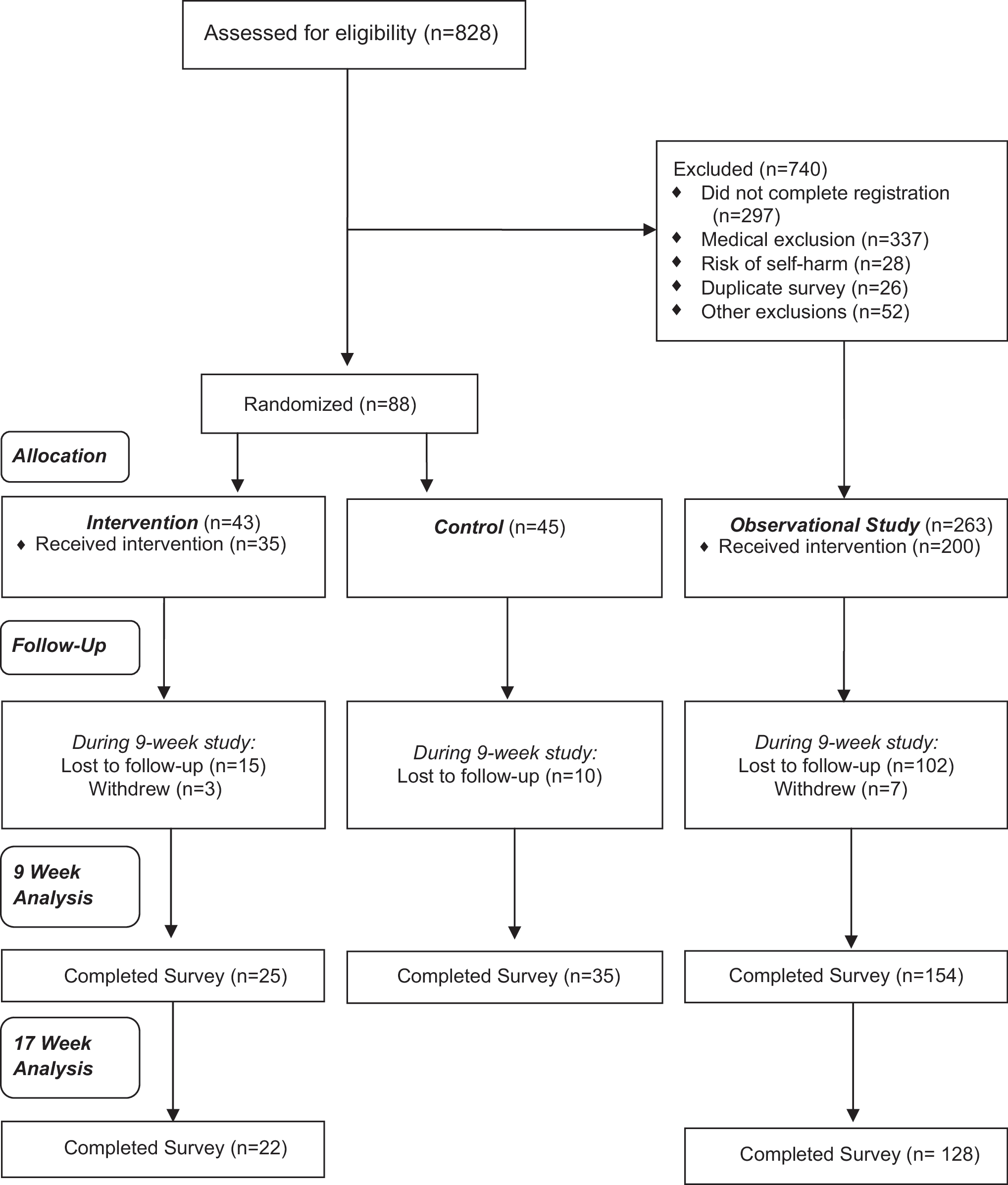
Study flow of patients into randomized clinical trial and observational study.
The trial was registered on
Study Population
Participants were recruited between September 2011 and August 2013, primarily through emails to individuals registered to receive Cleveland Clinic Wellness Institute educational and marketing materials in addition to recruiting via physical and online advertisements, employer-employee communication, physician referral, and social media.
Participants were informed of the study risks and benefits and given an online consent form before registering. Eligibility criteria included being ≥18 years of age, having regular Internet access, being willing to log on regularly for 3 to 7 months, keeping daily sleep logs for 2 months, and being willing to be randomly allocated into a wait-list control group. An online screening survey with additional inclusion and exclusion criteria based upon self-report (Table 1) was then used to determine final eligibility. Participants needed to report symptoms of at least 3 months of insomnia as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) to be included, thus excluding participants with short-term, or acute, self-resolving insomnia. 18
Insomnia Inclusion and Exclusion Criteria
Intervention
GTS is a 6-week, online, interactive, CBT-based program designed to foster best sleep practices, sleep restriction, and stimulus control. It teaches cognitive and behavioral approaches to manage sleep and educates on lifestyle and bedroom factors that impact sleep quality and quantity. 11,22 Similar to other Web-based programs, GTS utilizes strategies from CBT-i, but it also has a broader focus on overall health and wellness. The program emphasizes general stress management techniques with a strong focus on helping the user learn relaxation and meditation strategies to decrease the mental and physiological arousal that occurs with insomnia and stress.
Daily program access was encouraged via daily email reminders to complete a sleep log based on the prior night's sleep pattern. After completing the sleep log, the daily lesson is made available to the participant. Delay in completing a daily log prompts the program to be temporarily suspended to allow for participant flexibility and ensure complete exposure to the program content. Thus, the program completion time varied depending on the frequency of log completions. The daily sleep logs included 13 questions regarding prior night sleep patterns including sleep onset latency, TST, waking after sleep onset, and number of awakenings. This information was used to calculate and display average sleep time per night and a sleep efficiency score, providing daily progress as an engagement tool. Having the user keep a daily sleep log was done to encourage daily user participation and decrease the potential for retrospective recall bias that may occur when not completing the sleep log consistently and on a daily basis.
Sample Size Estimates
The prespecified primary outcome was absolute change in ISI score at 6–10 weeks (first follow-up). With an alpha of 0.05, power of 0.80, standard deviation of 4.5, and a conservative 50% drop-out, we needed 56 participants in each of the two study arms to detect a clinically meaningful difference of five points on the ISI. 14,20 We aimed to enroll 60 participants per arm. There were no sample size estimates performed for the observational cohort, and it continued for the duration of the clinical trial.
Outcomes
Baseline questions included participant demographic characteristics, sleep patterns, insomnia history, sleep-related lifestyle habits, and medical history. Participants completed the PHQ-9 measure of depression 23 and the CAGE Questionnaire for alcoholism 24,25 to assess clinical trial eligibility and then again postintervention to measure change in insomnia and stress in both intervention and observational groups. The first follow-up was at approximately week 9, although actual time varied between participants, and ranged from ∼7 to 12 weeks given the variable individual start and completion dates. Sustainable changes in insomnia or stress symptoms were evaluated through a second follow-up at approximately week 17, or 8-weeks postcompletion, with a range of 15 to 20 weeks.
Standard questionnaires at these follow-ups included the ISI (primary outcome), which is a seven-item self-report measure that assess an individual's self-reported insomnia symptoms on a four-point Likert scale, with higher scores indicative of more severe insomnia. 26 Psychometric assessment revealed that it is a valid and reliable measure of both sleep difficulties and changes in sleep difficulties following treatment.
Two additional questionnaires (secondary outcomes) collected at follow-ups were the Pittsburgh Insomnia Rating Scale 20-item version (PIRS20) 27 and the 10-item Perceived Stress Scale (PSS). 28 The PIRS20 is a self-report questionnaire of daytime symptoms and sleep parameters as an overall measure for insomnia severity. It was derived from the PIRS65 with the help of Item Response Theory analysis to include items across the spectrum of insomnia severity. Each item is scaled 0–3, convenient for summary scoring. Preliminary validity pointed to discriminant validity against sleepiness and partial correlation with scales for depression, anxiety, and fatigue, with overall one-factor structure. The PSS measures a person's perception of, and response to, daily hassles and stress, resulting in a total stress score of 0 (best) to 40 (worst). Additional secondary outcomes were TST and sleep efficiency, as reported in daily logs. Neither study participant nor investigative team was blinded to study group assignment.
Statistical Methods
Descriptive statistics of baseline characteristics were generated using means and standard deviations for continuous measures and frequencies with percentages for categorical factors. Participants who failed to complete the first follow-up were compared at baseline to those who completed the first follow-up on basic demographics and baseline survey scores using two-sample t-tests and Pearson chi-square tests. The primary analysis was based on the intent-to-treat principle, comparing ISI, PIRS, and PSS score changes across groups. This analysis was performed using mixed-effect models, assuming an autoregressive correlation structure for observations from the same participant over time. Least square mean estimates were calculated and summarized with 95% confidence intervals. The observational cohort was analyzed similarly, although only within-group changes were evaluated. As a sensitivity analysis, a per-protocol analysis was performed using similar methodology including just the participants who completed the first follow-up survey.
Mixed models were used to evaluate patterns of change in patient-reported TST and sleep efficiency using averaged weekly measures from the 6 weeks of active online participation among participants in the intervention group and observational study. Contrasts to test for linear trends in these measures over time were performed. Analyses were performed in R version 3.1.0 and SAS 9.3 software (SAS Institute, Cary, NC).
Results
Randomized Controlled Trial
We randomly allocated 43 study-eligible participants to the intervention and 45 to control arm. In the intervention and control arms, 25 and 35 participants provided data at the first follow-up respectively and 22 in the intervention arm provided a second follow-up (Fig. 1).
Within the intervention arm, three participants withdrew (reasons not provided), eight did not provide a single daily sleep log and thus did not receive the intervention, and seven were lost from the study despite follow-up attempts by study staff. Twenty out of 23 participants who provided at least one daily sleep log and completed the first follow-up survey completed the entire online program. There were no serious adverse events reported. In the intervention arm, three participants reported sleeplessness as a result of following the sleep restriction recommendation and one reported waking more frequently during the night due to concern about completing the daily log.
We observed no significant differences at baseline between the intervention and control arms (Table 2). The mean age of participants was 54 years, over 80% were women, and on average, overweight with a mean body mass index of 27. More than half of the participants reported sleep difficulty for more than 2 years. There was a broad range in frequency of sleep latency and sleep maintenance difficulties; however, all participants suffered from at least one of the following inclusion criteria: difficulty falling asleep ≥3 nights/week (49% of participants), difficulty staying asleep ≥3 nights/week (64%), or waking early with inability to return to sleep ≥3 nights (52%). Twelve (28%) participants in the control arm and 16 participants (36%) in the intervention were at risk of obstructive sleep apnea with three or more positive responses on the STOP-BANG questionnaire. 29
Baseline Characteristics of 88 Randomized Controlled Trial Study Participants with Primary Insomnia
Percentages may not total 100 given missing values (1 in control and 2 in intervention).
For BMI, 70 of 88 participants provided data.
Participants with scores greater than 14 excluded from randomized controlled trial.
SD, standard deviation.
Analysis of change in sleep patterns and perceived stress is shown in Table 3. There were significant improvements in ISI score, PIRS and PSS, in the intervention group compared to control. At first follow-up, a mean ISI score decrease of 7.3 (95% CI: −9.0, −5.6) was observed in the intervention group compared to a 1.3 (−2.7, 0.1) reduction in the control group (p < 0.001). Sustained ISI improvement in the intervention group was observed at second follow-up (17.0 at baseline, 9.8 at first follow-up, and 8.9 at second follow-up) with similar improvements for PIRS and PSS scores. We observed commensurate patterns when only the 60 participants who provided both baseline and first follow-up data (per-protocol analysis) were analyzed. There were no significant baseline differences between those who completed the first follow-up and those who did not, with the exception of ISI scores: 16.3 for completers versus 17.9 for noncompleters (p = 0.044).
Change in Sleep and Perceived Stress Among 88 Participants with Primary Insomnia
Mean (95% CI) shown.
ISI, Insomnia Severity Index; PIRS, Pittsburgh Insomnia Rating Scale 20-item version; PSS, 10-item Perceived Stress Scale.
Secondary outcome analysis of participants in the intervention group showed no significant change in sleep efficiency (from 83% during week 1 to 85% during week 6, p-for-trend 0.42) but a decrease in night-to-night variability (standard deviation during week 1 was 7.46% and 4.59% during week 6, p-for-trend 0.034). TST remained unchanged among those receiving intervention (6.2–6.6 h/night), although there was a nonsignificant decrease in night-to-night variability in TST (standard deviation during week 1 was 1.01 and 0.89 h during week 6, p-for-trend 0.16).
Confirmatory Effectiveness Test Sample
We enrolled 263 participants in the effectiveness sample (Fig. 1) and received data from 154 and 148 participants at the first and second follow-ups respectively. Seven participants withdrew from the effectiveness sample and the remainder were lost to follow-up. Sixty-three participants in the effectiveness sample did not receive intervention due to failure to log in and provide any sleep logs. Of the 140 participants who provided at least one daily sleep log and completed the first follow-up survey, 110 followed through to the end of the online program. There were no adverse events from the study intervention reported.
Baseline characteristics of the study participants in the effectiveness sample are shown in Table 4 and were similar to those in the randomized controlled trial. However, nearly half of participants in effectiveness sample (123, or 47%) were at risk of sleep apnea. Table 3 lists the major comorbidities of participants in the effectiveness sample, and often participants reported more than one. The two most common conditions were arthritis or chronic pain (24%) and diagnosed sleep apnea (19%). Of the 263 participants, 40% had a PHQ-9 score suggestive of mild depressive symptoms, while 32% had a score suggestive of moderately severe to severe depression symptoms. Twenty participants (7.6%) had two or more positive questions on the CAGE questionnaire, suggesting a possibility for elevated risk of alcohol abuse. Nearly one-third of participants (29%) were taking over-the-counter medications for sleep and nearly a quarter were taking medication for depression (23%) or taking care of young children, pets, or elders (23%) in a way that impacted their sleep.
Baseline Characteristics of 263 Study Participants with Comorbid Insomnia
Percentages may not total 100 given missing values (one in control and two in intervention).
One missing response.
OTC, over the counter; SD, standard deviation.
Improvements in ISI, PIRS, and PSS observed in the effectiveness sample group were similar to the primary intervention arm (Table 5). Secondary outcomes analysis revealed significant improvements in sleep efficiency (from 82% to 88%, p-for-trend <0.001) with decreases in night-to-night variability in sleep efficiency (standard deviation 8.69% during week 1 and 5.03% during week 6, p-for-trend <0.001). TST also improved (from 6.6 to 7.0 h/night, p-for-trend <0.001), and there was a decrease in night-to-night variability of TST (standard deviation during week 1, 1.26, and 0.96 h during week 6, p-for-trend < 0.001).
Changes in Sleep and Perceived Stress Among 263 Participants with Comorbid Insomnia
Mean (95% CI) shown.
Discussion
We observed clinically meaningful improvements in insomnia severity symptoms and perceived stress in adults with primary or comorbid insomnia undergoing a 6-week CBT-based online program. Sustained improvement over a 4-month period underscores the effectiveness of well-constructed online CBT-i programs, even in those with comorbid insomnia.
Our observed ISI reduction in the intervention group differed from previously published CBT-i studies, potentially due to differences in study population and design. 14,20,30 Surprisingly, sleep efficiency and TST were minimally affected in the intervention arm, possibly due to high baseline values limiting the range for improvement and ability to detect change.
Participants who did not provide first follow-up data had slightly higher baseline ISI and PIRS scores than those who provided follow-up, suggesting that those with more severe insomnia may have dropped out due to lack of symptom relief and may require more intensive care. We were unable to directly compare our attrition and login rates to other reported studies given the varying measures of adherence. 14 Baseline age, gender, or insomnia severity were not associated with drop-out, but intervention-group participants were less likely to return the questionnaires, possibly due to fatigue from receiving daily emails during the program.
Web-based CBT-i may be an attractive option for patients with comorbid insomnia as it may mitigate polypharmacy and potential interactions of sleep medications with other medications. A study of Web-based CBT-i for comorbid insomnia in cancer survivors demonstrated a marked improvement in insomnia severity. 30 Another study including adults with stable comorbid sleep or psychiatric disorders reported results similar to ours, suggesting that online CBT-i may benefit a wide range of patients with insomnia and comorbid chronic health/psychiatric conditions. 14
Although psychological stress and major life changes are typical perpetrators of sleep disturbance, various maladaptive behaviors and dysfunctional thoughts can independently worsen the problem, often causing individuals to become nonresponsive to medications. 30 CBT-i exerts its benefit by changing thoughts and behaviors that perpetuate insomnia through five treatment components: sleep restriction, stimulus control, cognitive restructuring, sleep hygiene, and relapse prevention. 30 Evidence suggests that CBT-i is as effective in the short- and long-term as medications. 4
Our study has important strengths including a large sample size, valid and reproducible measures of sleep habits and stress, and a measure of sustainability of the intervention beyond program completion.
Study limitations include lower than anticipated enrollment, a short follow-up period, lack of data on sleep medication changes, temporal changes in insomnia treatment, or seasonal effects, although we expect the latter two to be randomly distributed in the data. 18 Sleep disturbance may be better captured through longer sleep diaries as opposed to a single night of objective sleep monitoring due to nightly variability in insomnia. 30 This was an un-blinded study, but the risk for bias in study performance was mitigated by limited and remote interaction with participants. Additionally, our largely white, middle-aged, and educated female population limits the generalizability of our results. Although the prevalence of insomnia is higher among women than men in the general population, our primary recruitment method of emails to individuals registered to receive Cleveland Clinic Wellness Institute educational and marketing materials also contributed to the high proportion of females in our study. Future studies should enroll larger and more heterogeneous samples to improve the generalizability of the findings. Moreover, we used a wait-list control, which does not control for all nonspecific effects, such as participant expectations and potential placebo response to attention/focus given to those receiving intervention. 20 Future studies should include a placebo control group/attention-matched control condition such as an Internet delivered program focused on healthy lifestyle strategies that does not include sleep related content. Although we cannot pinpoint the specific programmatic aspect that was beneficial, the benefits are unlikely due to a placebo effect given previous studies that demonstrate a lack of insomnia symptom improvement despite full participation in a credible non-CBT-i-based online program. 18
Another limitation is that we used self-report screening questionnaires to identify additional comorbid concerns without including a clinical interview or polysomnography to rule out sleep disorder pathology. However, to ensure real-world evaluation of the online intervention, participant enrollment and collection of eligibility and baseline data were obtained via Internet without face-to-face contact. Due to difficulty recruiting participants that met inclusion criteria for the intervention and control groups, study recruitment was ended before reaching our estimated sample size. This may have led to decreased power, which may have caused an underestimation of our findings.
The GTS program represents a safe, low-cost, promising and sustainable treatment alternative to medications to improve insomnia symptoms in a diverse patient population with primary and comorbid insomnia in a large healthcare system.
Footnotes
Acknowledgments
Internal funds were from the Wellness Institute, Cleveland Clinic. We thank Tom Gubanc for his assistance in the design of the online program and recruitment of study participants. We also thank Srividya Ramachandran, PhD for editorial assistance with this article (no compensation was provided for this service).
Disclosure Statement
Cleveland Clinic Wellness Institute sells the online program, Go! to Sleep©. No competing financial interests exist.