
Abstract
Background:
With the introduction of online health screenings, guidelines describing how to communicate about a person's health need to be adapted for a digital setting. This study aimed to uncover older adults' preferences regarding such online messages.
Materials and Methods:
Thirty older adults (aged 65 to 75 years) viewed four versions of the results message of a screening aimed at identifying frailty: a standard, empathic, tailored, or both empathic and tailored message. After each version, they were interviewed about what they (dis)liked about the message. They also ranked the four versions according to preference. Ranks were analyzed with a Friedman's test and a Wilcoxon's signed-rank test.
Results:
There was no significant difference for message-type preference when the outcome was positive. For the prefrail or frail outcome, message-type preferences differed (χ2 = 10.51, p = 0.02 and χ2 = 13.56, p < 0.01, respectively). Overall, for the prefrail and frail outcome, the tailored version was appreciated most. Participants commented that the tailored version made them feel appreciated more as a person. Some found the empathic additions comforting, others found these unnecessary.
Conclusions:
When communicating the results of an online health screening to older adults via the Internet, one should primarily tailor the message toward personal characteristics. The effect of empathic elements in results messages appeared to be limited. Whether a message should be adapted depends on whether the outcome is positive or negative.
Introduction
Informing patients about their health status is an integral part of many healthcare professionals' work, and this topic is addressed in depth during their education. Especially in case of bad news (“news that results in a cognitive, behavioral, or emotional deficit in the person receiving the news that persists for some time after the news is received” 1 ), the mode of delivery is highly important, since proper delivery results in higher patient satisfaction and patient trust, and in an increase in the patient's ability to deal with the consequences of the news. 2,3 As a result, there are many guidelines for informing a person about his or her health status, particularly for delivering bad news. Girgis and Sanson-Fisher 4 listed 16 principles for breaking bad news, including that one should provide accurate and reliable information, that one should use eye contact and body language to convey warmth, sympathy, encouragement, and reassurance, and that one should be sensitive to a person's culture, race, religious beliefs, and social background.
Another set of guidelines, called PATIENT, 5 emphasizes the need to make communication toward patients personal, clear, timely, as informative as possible while taking into account the literacy level of the patient, reliable, instructive, and easy to remember. Perhaps the most well-known set of guidelines is SPIKES, 6 a six-step protocol for delivering bad news. According to SPIKES, one should (1) set up a meeting (ensuring privacy, connecting with the patient); (2) assess the patient's perception about his or her situation; (3) obtain the patient's permission to provide information; (4) provide the information in understandable language; (5) address the patient's emotions with empathy; and (6) discuss next steps and summarize the meeting. All of these guidelines were created under the assumption that news would be delivered in a face-to-face setting with a high degree of interactivity, where tailoring and empathy play an important role.
Now that online health screenings have been made available, these guidelines need to be adapted for use in a digital setting: How should one inform a person about his or her health status when the results that were assessed via an online service are also presented in a digital environment? The cues upon which care professionals are advised to react cannot be observed and acted upon easily when the news is provided in a mediated manner, if these can be acted upon at all. And while there is an abundance of articles discussing how to draft general online health information, guidelines for creating online personal messages with the results of a health screening are nonexistent. One study that does address the topic focuses on communicating the results of tests on sexually transmitted diseases, to men who have sex with men, via an Internet site. 7 Overall, these men liked the option of receiving these results online, but the preferred communication style depended on the impact of the disease; an empathic style was only preferred above an informative style in case of a high-impact serious disease. Of course, the results of this single study cannot be generalized toward all patient types and all types of medical conditions.
In this article, we report on a study that aims to uncover older adults' preferences regarding online messages with the results of a health screening. More specifically, we focus on the role that tailoring and empathy play in communicating health-screening results online. The results of this study will have important implications for designing online health screenings, which are becoming increasingly popular due to the possibilities they offer for easily screening large numbers of people at low cost with immediate result for the person being screened. 8
Materials and Methods
We conducted this study within the context of “langgezond.nl” (Dutch for “healthy for a long time”). 9 Langgezond.nl is a service that aims to detect and prevent frailty among older adults; frailty being a state, in which an older adult's health slowly deteriorates, and which leads to functional decline and a lower ability to deal with adverse health events. Frailty is an unknown concept among older adults and it develops unnoticed. Therefore, it is important to identify the development of frailty early on and to provide services to revert this trend, for example, by means of physical training, cognitive training, or dietary advice. Langgezond.nl offers a general health check for adults between 65 and 75 years of age. This general screening can be completed on paper or online. Older adults are invited for this health check by their general practitioner, who sends a standardized invitation to all of his/her patients in the age range of 65–75.
The results of the screening are provided immediately after the screening (when completed online). A general message is presented, which explains how the older adult scored on different aspects of the screening: general health, physical functioning, cognitive functioning, and dietary habits. The combined scores on these aspects lead to three possible results. The older adult is (1) robust, and will be invited for a new screening a year later; (2) prefrail, and is invited for a second screening on-site with physical and cognitive tests and eventually to training services; or (3) frail, and is referred to his/her general practitioner for further investigation.
For this study, we have taken the existing screening-results message as a standard baseline, and designed three variants for each of the three possible following results: 1. An empathic version, to which, following Baile et al.,
6
elements were added that reflect on the (likely) feelings of the older adult, validate these feelings, and explain why these feelings are valid (e.g., for the message in which a person is told he or she is frail: “Maybe this result comes as a surprise to you […] This reaction is understandable, but there is no reason to worry. This test gives an impression about your health and the General Practitioner will examine the results more extensively.”); 2. A tailored version, to which elements were added that make the message geared toward the characteristics of the older adult. As suggested by Kreps and Neuhauser,
10
we included the older adult's name, age, email address, and the name of his or her general practitioner. Then, we added elements that referred to answers that the older adult had provided during the screening (e.g., when cognitive health was found to be fine: “You have indicated, among other things, that you don't have trouble with remembering your appointments. […] Therefore, we conclude that the health of your brain is good.”); 3. An empathic and tailored version, in which empathic and tailored elements were combined.
See Figure 1 for an empathic and tailored screening-results message.
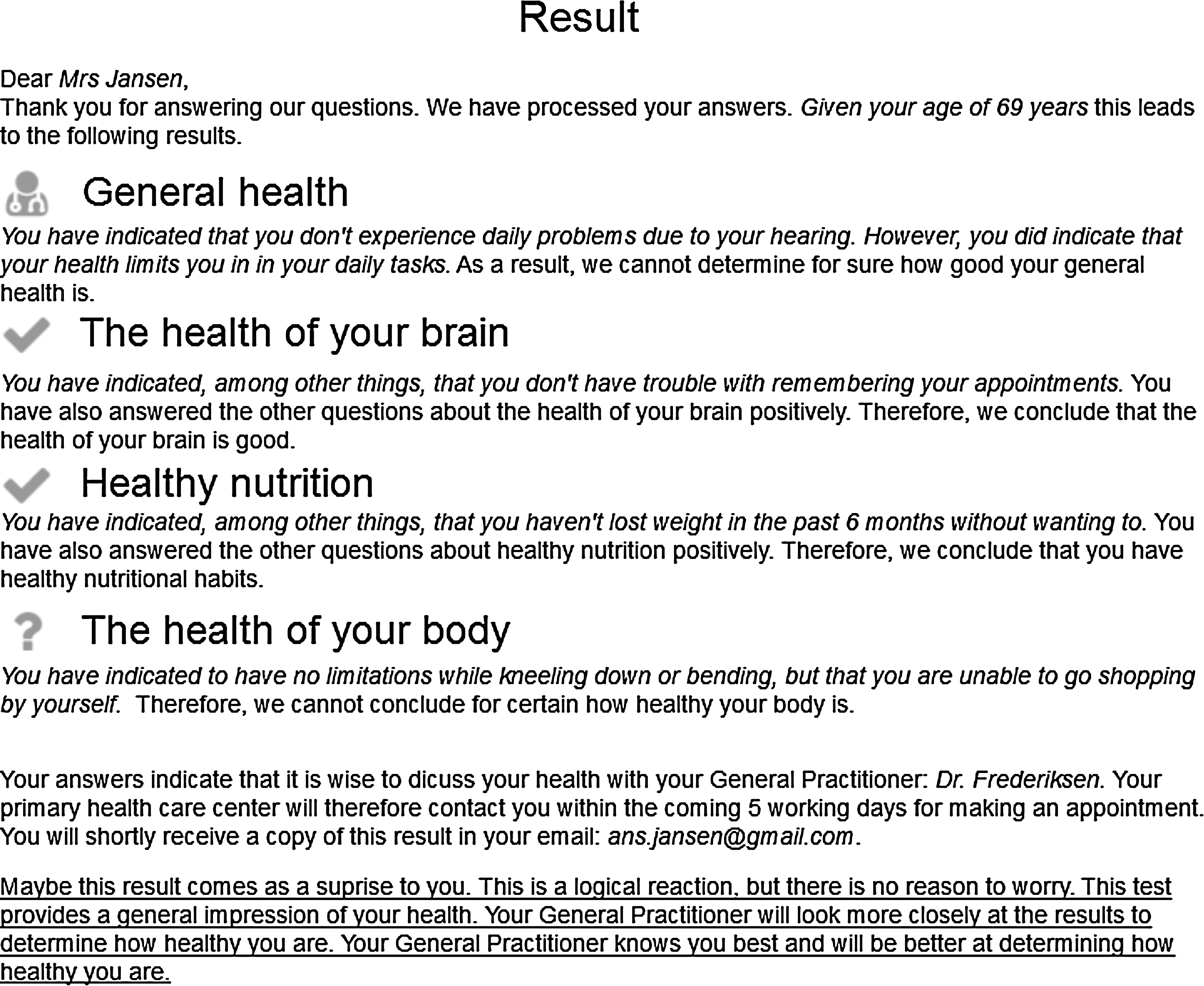
An empathic and tailored screening-results message (empathic elements are underlined, tailored elements are in italic).
Since there is no previous research on the topic of communicating about a person's health status via the Internet, we took an in-depth approach. Thirty participants in the age range of 65 to 75 years were interviewed face-to-face. They were recruited throughout the Netherlands via a snowball sample. Each participant was assigned to one of three screening-outcome conditions: robust, prefrail, or frail. After having provided informed consent, each participant was told the story of the fictitious character Ans Jansen, who completed the first screening online and immediately received her screening outcome. Using such a scenario and character allows older adults to imagine a new concept and to provide meaningful feedback. 11 For the condition a participant was allocated to, he or she was shown all four versions of the results message in random order. After each message, the participant was interviewed about his or her thoughts about the message. Finally, each participant was asked to rank the four versions according to his/her preference (the first choice received four points, second choice three points, third choice two points, and fourth choice one point). Preference points were accumulated to determine a total score for each version in each condition.
To determine whether differences existed among the preferences, we conducted a Friedman's test for each condition. For the conditions, in which a significant difference was found, we performed a post hoc analysis by means of the Wilcoxon's signed-rank test to determine which message version was preferred over the other. Since we made many comparisons during the post hoc analyses, we applied the Benjamini–Hochberg procedure to prevent so-called false discoveries. In short, one calculates a threshold for each obtained p-value from the post hoc analysis, which the specific p-value should not exceed. If this does happen, the result of the post hoc test should be considered insignificant, regardless of the p-value. When calculating the Benjamini–Hochberg critical values, we applied a control value of 0.10.
Interviews were transcribed and analyzed by means of inductive thematic analysis. 12 Since there were no existing coding schemes available, we scrutinized the transcriptions for reasons for a preference; the creation of the coding scheme was data driven. This resulted in 11 reasons (or codes), such as “More friendly,” “Not comforting,” and “Vague.” In total, 168 fragments were coded by one researcher. An external researcher then recoded 62 items to determine intercoder reliability. The resulting Cohen's kappa was 0.70, which stands for good agreement. 13
Results
Table 1 shows the characteristics of the participants per condition. As can be seen, more women than men participated in the study.
Participant Demographics
After having viewed the four result messages for an outcome, the participants were asked to rate their preference by awarding points. The results can be found in Table 2. As there were 10 participants per condition, a maximum score of 40 points could be achieved, while the lowest score amounted to 10 points. Friedman's tests showed that for the “robust outcome,” there were no differences among the preferences (χ2 = 5.24, p = 0.12). For the other two conditions, there were differences with respect to the preference points that were awarded to the message versions (prefrail condition: χ2 = 10.51, p = 0.02; frail condition: χ2 = 13.56, p < 0.01). The results of the post hoc analysis can be found in Table 3 (prefrail condition) and Table 4 (frail condition).
Preference Points for the Different Message Versions
There were no differences among preference points for the robust condition (χ2 = 5.24, p = 0.12); there were differences among preference points for the prefrail and frail conditions (χ2 = 10.51, p = 0.02 and χ2 = 13.56, p < 0.01, respectively).
Results of the Post Hoc Test for the Prefrail Condition
Results of the Post Hoc Test for the Frail Condition
Based on the Benjamini–Hochberg procedure, we accepted the three lowest p-values for the prefrail condition, and the four lowest p-values for the frail condition. In sum, for the prefrail condition, we found the following: - The tailored message was preferred over the standard message and the empathic message; - The message in which empathy and tailoring were combined was preferred over the empathic message.
And for the frail condition, we found the following: - The empathic message, the tailored message, and the message in which empathy and tailoring were combined were all preferred over the standard message; - The message in which empathy and tailoring were combined was preferred over the empathic message.
The participants were asked to explain their preference for one version over the other. For the robust condition (for which we found no significant differences among the preference scores), we found that about half of the participants found the standard version “too short.”
The empathic message received mixed responses. On the one hand, it was evaluated positively (more friendly and personal), while on the other hand, the empathic additions were considered unnecessary. The tailored message was quite frequently found to be “more personal” and “including more detail,” although some participants also found the tailored additions unnecessary. The message in which empathy and tailoring were combined was mostly considered to be “too long” and unnecessary.
For the prefrail condition, the standard message was considered “not comforting” and “too short.” The empathic version again received mixed results. Part of the participants experienced it as not comforting, while others thought it was; some older adults thought it was friendlier, while others found the additions unnecessary. The tailored version was considered to be “more personal” and “more detailed.” As one participant (woman, 67 years) worded it:
“It's a bit friendlier, because it is more personal. And that makes it friendlier. The standard version is fine as well, but this is nicer. Here, you don't have the idea you're a number; this is a bit more personal.”
When tailored and empathic elements were combined in a message for this condition, quite some participants found this unnecessary.
For the frail condition, finally, the standard message received quite some critique; participants found the message “not comforting,” “too general,” “too short,” and “vague.” The empathic message received more positive comments, and was perceived to be “more comforting” and including more details. One participant (man, 75 years) phrased it as follows:
“It comes across as quite comforting. If you've been somewhere and they refer you to your General Practitioner, it's always a bit scary, because they don't send you to the General Practitioner for no reason. If you have to, it means they have discovered something. In that case, the extra explanations are fine.”
The empathic additions were, however, also thought to be unnecessary by some. The tailored variant received contradictory comments and included, according to the majority of the participants, more details, while half of them also thought the message to be vague. A majority also found this message to be more personal. The message in which empathic and tailored elements were combined was found to be more comforting, providing more details, friendlier, and more personal on the one hand, while another part of the participants found the additions unnecessary.
Discussion
When communicating the results of an online health screening involving older adults via the Internet, we found that one should, first and foremost, tailor the message toward personal characteristics, including the person's name and age, mentioning his or her general practitioner, and explicitly linking the answers that a person provided with the resulting outcome leads to higher appreciation of the content of the message. This finding is in line with previous studies that showed the positive effect of tailoring health information for achieving behavior change. 14 The effect of including empathic elements in results messages appeared to be limited and scattered when combined with tailoring. The results of our study further suggest that the outcome of the screening influences the preference for a results message: when the news is “you are fine,” older adults seem to be okay with a simple, standardized message, but when the news is negative, older adults appreciate a more personal message. These results are in line with the results of a previous study on communicating results of a test on sexually transmitted diseases via the Internet, 7 which showed that an empathic style is appreciated for high-impact diseases, but not for less serious diseases.
Like any study, our work has some limitations. First, our sample size was relatively small. We opted for this size, because no previous work had been done on the topic, and we wanted to achieve an in-depth understanding via qualitative data analysis. A next step would be to test our findings among a larger sample, for example, via an online survey. Second, our study focused on the general population of older adults, who may have different expectations regarding online feedback about their health status than younger people, or people who have already been diagnosed with a medical condition. Third, in our study, we focused on the role of empathy and tailoring, while there are many other means that can improve result messages for online health screenings, such as adding more or other visuals to the text, 15 or tailoring the message toward the health-literacy level of the members of the target group. 16 Future research should explore their added value. And finally, we did not collect a full set of details about the participants, and therefore, could not assess whether the different groups that were assigned to a condition differed on issues, such as their health status or health literacy.
Online health screenings are becoming increasingly popular, due to their obvious benefits: the possibility to screen a large population quickly at low cost. Especially within the context of mental healthcare, these are frequently used. 17 Knowing how to automate the provision of screening results is therefore becoming an increasingly important topic. After all, the last thing one wants is participants to get worried unnecessarily and start contacting medical professionals. This study has made an important first step in developing design guidelines for online screening-result messages. In time, works such as these should enable us to move public health screening to online settings while providing a pleasant user experience and maximum ease of use.
Footnotes
Acknowledgments
This work was undertaken within the context of the PERSSILAA project (
Disclosure Statement
No competing financial interests exist. The sponsor had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.