
Abstract
Background:
Chronic heart failure (HF) causes significant morbidity, mortality, and cost. Managing HF requires considerable self-management skills and self-efficacy. Little information exists about feasibility and potential impact of a mobile monitoring intervention to improve self-efficacy and quality of life (QoL) among minority patients with HF.
Materials and Methods:
We developed a mobile phone-assisted case management program and tested its impact on outcomes in minority patients with HF in a 2:1 randomized controlled trial. We evaluated self-care efficacy, knowledge, behavior, and QoL at baseline and 3 months.
Results:
We enrolled 61 participants: intervention 42, usual care 19; mean age ± SD: 55 ± 10 years; 64% male; 75% white Hispanic, 25% African American; and 56% high school education or less. Comparison of the two groups with respect to changes from baseline to 3 months showed significant differences for Self-Efficacy for Managing Chronic Disease (2.09 ± 2.32, p-value = 0.005); health distress scale (−1.1 ± 1.5, p-value = 0.017); and QoL (Role Physical, 23.6 ± 44.5, p-value = 0.042, and General Health, 11.1 ± 14.2, p-value = 0.012).
Conclusions:
A mobile phone-based disease management program may help improve self-care efficacy and QoL in a minority population and offers a modality to help reduce ethnic disparity.
Introduction
Heart failure (HF) is a complex disease that affects over 5 million people in the United States. 1 HF is a leading cause of hospital admissions and readmissions, reduced quality of life (QoL), and increased mortality; it poses an increasing burden and cost as the population ages. 2,3 Some evidence suggests that frequent monitoring can lead to early detection of decompensation, resulting in early intervention and thereby reduction of readmissions. 4 The American College of Cardiology/American Heart Association Guidelines for the Management of HF recommend daily weight monitoring as the cornerstone for the management of patients with HF. 5 Innovative methods to follow changes in weight and symptoms may improve the poor outcomes in HF patients.
HF patients who are actively involved in their own care and adhere to treatment regimens are more likely to have improved survival and decreased readmission rates and experience better QoL. 6,7 Previous studies on traditional telemonitoring of HF patients have suggested its potential to reduce hospitalizations, costs, and mortality, as well as to improve QoL and self-care, but the results have been inconsistent. 5,8 –11 Mobile phones are ubiquitous, low cost, and scalable 12 and offer a unique opportunity with automated interactive features for text messaging, data gathering, reminders, and alerts. However, few HF disease management programs have used a mobile phone system. 13,14
There is still a critical gap in the feasibility and effectiveness of mobile phone-based HF programs overall, specifically in minority populations. Our study was funded as a technology transfer–commercial partnership grant to develop a usable cellular phone-based HF monitoring system and to conduct a randomized controlled trial to assess its effect. The main hypothesis was that daily monitoring using an automated system of mobile phone-based text queries, using simple yes–no responses related to key HF signs and symptoms, would improve patient self-care efficacy, knowledge, and QoL. The usability outcomes and challenges will be discussed in a separate article.
Materials and Methods
We implemented a mobile phone technology system offering automated daily monitoring of weight and symptoms of HF and conducted a proof-of-principle study. The University of Miami IRB approved this study before commencement.
Study Design
We designed a randomized, controlled prospective study in HF patients. The primary endpoint was change in Self-Efficacy for Managing Chronic Disease (SECD), a well-described measure of chronic disease self-management, 15 administered at enrollment and after the 3-month intervention along with other surveys. Demographic and clinical data were obtained through chart review. We administered all questionnaires in English or Spanish as per patients' choice.
Participants
Seven hundred and eighteen patients receiving care from the Heart Failure Clinic at Jackson Memorial Hospital, a county hospital in Miami, were prescreened and 296 of them met the eligibility criteria. Eligible participants were community-dwelling ambulatory patients diagnosed with HF. Other eligibility criteria included age ≥18 years; ability to speak and read English or Spanish; anticipated survival ≥6 months; no previous history of unstable coronary syndromes; no end-stage HF; and no heart transplantation. Of the 296 eligible patients, 184 were screened in person for their interest in the study, ability and willingness to operate the mobile phone, and read, comprehend, and respond to the mobile phone-based text queries. At the screening visit, 123 patients declined to participate in the study. The most common reasons were not enough compensation, too much time commitment, not motivated, and others just said no. We randomized the remaining 61 patients in a 2:1 ratio to two groups: Mobile phone Intervention (n = 42) and Usual care (n = 19). Figure 1 shows the CONSORT diagram.
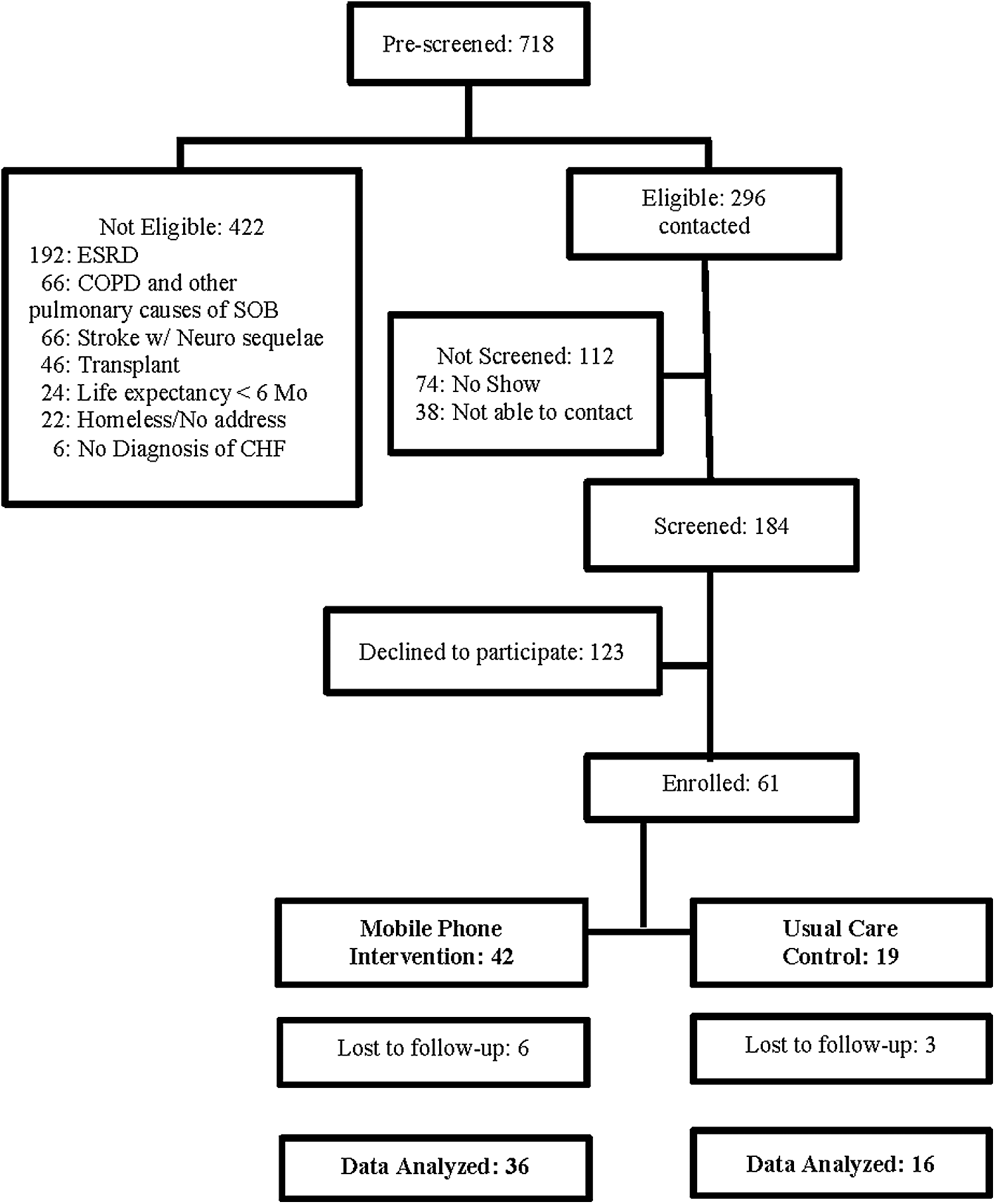
CONSORT Diagram.
Measures
We collected clinical and sociodemographic information at baseline. HF knowledge, self-efficacy, self-care behavior, and QoL were assessed at baseline and at 3 months using validated instruments.
Sociodemographic characteristics
Participants reported age, gender, ethnicity, education, marital and employment status, current smoking and alcohol consumption status, and mobile phone use ( Table 2 ).
Clinical characteristics
We reviewed medical charts to abstract clinical data ( Table 2 ).
Instruments used in this study included the following:
1. Chronic disease self-management program scales: (
Other subscales included are Health Distress Scale (HDS), 17 Communication with Physicians (CP), 15 Fatigue Visual Numeric (FVN), and Shortness of Breath Visual Numeric (SBVN). 18
2. Heart Failure Self-Efficacy Scale–30 (HFSE-30). This 30-item scale assesses self-efficacy with HF overall and with medications, diet, symptoms, activity, and HF readmission. Using a Likert scale with item scores ranging from 0 to 10, the scale score is the mean of the items. 19
3. The European Heart Failure Self-Care Behavior Scale (EHFSC). This 12-item questionnaire assesses self-care behavior of patients with HF. 20,21 Using a Likert scale with item scores ranging from 1 to 5, scale score is the sum of responses.
4. The Dutch Heart Failure Knowledge Scale (DHFK). This 15-item questionnaire assesses HF knowledge in general, knowledge on HF treatment (including diet and fluid restriction), and HF symptoms and symptom recognition. 22 Each correct answer gets one point and the total score ranges from 0 to 15.
5. Minnesota Living with Heart Failure Questionnaire (MLHFQ). This validated 21-item questionnaire assesses HF-specific QoL. 23 Using a Likert scale with item scores ranging from 0 to 5, the scale score is the sum of responses.
6. The Medical Outcome Study 36-Item Short Form (SF-36). This validated 36-item QoL instrument consists of 8 domains. All domains are scored using weights derived from a national probability sample. 24 The total weighted score on each domain ranges between 0 and 100.
Procedure
After signing the informed consent and completing baseline questionnaires, each participant was randomized by the study coordinator, who was blinded to the randomization until then, using a sealed envelope from the statistician. All participants were given a weight scale UC-321 (A&D Medical) to weigh themselves daily. Both groups continued to receive usual care in the Heart Failure Clinic, which included visits determined by the clinic providers based on HF severity and medication optimization need. All participants received $10.00 in compensation at study completion.
Intervention group
Participants in the intervention group received a mobile phone (model FG 630) to be used for the 3-month period of the study for daily monitoring. The program covered all costs for data use on the mobile phone and 30 free minutes of calling every month. Participants chose their preferred time to receive the daily questions. They were asked to weigh themselves daily and use the mobile phone to answer 10 daily questions about their weight and HF symptoms (yes/no format) for 3 months ( Table 1 ). The daily responses took about 2–3 min. Patients received 3 messages, 15 min apart, if they did not respond to the first automated message. The server used the cell number for patient identification. The server did not transmit or store any identifying information on the mobile phone. The transmitted information was stored in the server database and immediately programmatically analyzed for triggers of any deterioration. If responses indicated possible worsening of the HF (based on preconfigured algorithms), the patient received a message asking to contact the study coordinator. The study coordinator was able to view the data on a secure Web site and received an alert on his/her mobile phone. He/she contacted the patient to ask additional questions to confirm if there was indeed a decline in the patient's status and helped him/her to coordinate his/her care with the Heart Failure Clinic, as needed. We contacted patients in the intervention group at least once a month and administered the scheduled questionnaires.
Daily Questions Sent Through Web Browser Messaging
Only 1a or 1b is asked based on the response to Question 1(only if weight changed by at least three pounds).
All others were asked daily.
Note that a 3-lb or greater weight gain or a “Yes” answer to any of the questions 1a or 1b or to questions 2–10 triggered an automated message to the study coordinator to call the participant.
Control group
We contacted patients in the usual care control group at least once a month to administer the resource use questionnaire.
Statistical Methods
We performed within and between-group analyses to compare baseline characteristics and assess changes from baseline to the end of the trial. Simple analysis techniques used included independent sample t-tests for variables with normal or approximately normal distribution; Mann–Whitney tests for variables with skewed distributions and for ordinal variables; and chi-squared tests or Fisher's exact tests for discrete variables.
General linear mixed regression models 25 were used for repeated measures analyses and assessment of covariates and time by group interactions. These models are appropriate for analysis of longitudinal data when there is variation in the number of observations per participant and they do not require imputation to replace missing data.
Software
All statistical analyses were performed using the statistical analysis software (SAS, Version 9.3; SAS Institute, Inc.). Reported in the results are 95% confidence intervals and p-values corresponding to two-sided hypothesis tests. Results of all tests with a p-value <0.05 were considered as statistically significant at the 5% alpha level.
Results
Baseline overall and group-specific sociodemographic, mobile phone use, anthropometric, and clinical characteristics of the participants are shown in Tables 2 and 3 . Overall, 75% of the participants were Hispanic; 25% were African American.
Overall and Group-Specific Sociodemographic Characteristics of Study Participants
Values shown in bold are statistically significant.
Married or in a marriage-like relationship.
Divorced, Widowed, Never Married.
Two-tailed Fisher's exact test.
Two-tailed Fisher's exact test ignoring missing data.
SD, standard deviation.
Overall and Group-Specific Anthropometric and Clinical Characteristics of Study Participants at Baseline
Two-tailed Fisher's exact test.
SD, standard deviation; BMI, body–mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; BUN, blood urea nitrogen; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides; NYHA, New York Heart Association Class; LVEF: left ventricular ejection fraction; Hx: history of.
Baseline Characteristics
There were no statistically significant differences between the two groups, except with respect to age. For patients in the intervention group, age ranged from 27 to 83 years with a median of 53.0, a mean ± SD of 53.0 ± 9.4, and a 95% confidence interval of 50.1–56.0. The corresponding values for the control group were (47–77), 60, 60.3 ± 9.0, and (56.0–64.7). The age difference between the two groups, although statistically significant using both parametric (t-test p-value = 0.006) and nonparametric techniques (Mann–Whitney test p-value = 0.002), was not of any practical relevance. Although the mean weight of the intervention group was 8 pounds more than the control group (201.2 ± 42.6 vs. 192.5 ± 59.9), the difference was not statistically significant (p-value = 0.574).
Outcomes
Table 4 shows the results of the assessments performed at baseline and at 3 months, as well as the corresponding changes.
Within and Between-Group Comparisons of Study Groups
Difference = Intervention–Control.
Change = 3 Months–Baseline.
p-Valuec = p-Value for the change within group.
p-Value = p-Value for the difference in change between groups; Possible range given in parentheses below the outcome variable; Arrows indicate desirable directions; Significant p-values are bolded.
SECD, Self-Efficacy for Managing Chronic Disease; HDS: Health Distress Scale; CP, communication with physician; FVN, Fatigue Visual Numeric Score; SBVN, Shortness of breath Visual Numeric Score; HFSE, Heart Failure Self-Efficacy Scale-30; DHFK, Dutch HF Knowledge Scale; EHFSC, European HF Self-Care Behavior Scale; MLHFQ, Minnesota Living with Heart Failure Questionnaire; PF, physical functioning; RP, role physical; RE, role emotional; VT, vitality; MH, mental health; SF, social functioning; P, bodily pain; GH, general health.
Within-Group Changes
For each of the variables in Table 4 , the Change refers to the mean of the differences in value at 3 months minus the corresponding value at baseline.
In the intervention group, there was a significant increase in self-efficacy as measured by both the SECD and the HFSE instruments with p-values of 0.05 and 0.003, respectively, and a borderline significant change in CP scores (p-value = 0.056). For QoL, there was a highly significant improvement of 11.89 ± 19.70 in the MH score (p-value = 0.001) and a borderline significant improvement in the GH score (p-value = 0.06).
In the control group, there were also significant or borderline significant changes from baseline to 3 months, but some of these changes occurred in a deterioration direction. For example, instead of increasing, mean scores in this group showed a decrease in SECD (p-value = 0.058), RP (p-value = 0.029), and GH (p-value = 0.053). Similarly, instead of decreasing, mean values increased for HDS (p-value = 0.012) and FVN (p-value = 0.028). However, the DHFK score changed in the right direction with an increase of 2.2 ± 4.4 (p-value = 0.065).
Between-Group Comparisons
For each of the variables shown in Table 4 , the Difference refers to the mean of the differences in value between the intervention and control groups at the same time point.
At baseline, compared with the control group, the intervention group had significantly better mean knowledge scores (DHFK: 10.5 ± 2.6 vs. 8.8 ± 3.1, p-value = 0.038) and worse general health scores (GH: 44.9 ± 17.3 vs. 55.3 ± 14.4, p-value = 0.040).
At 3 months, there were no significant differences between the two groups with respect to any of the assessments performed.
Comparison of the two groups with respect to changes from baseline to 3 months showed significant differences for chronic disease self-efficacy (SECD, 2.09 ± 2.32, p-value = 0.005); health distress (HDS, −1.1 ± 1.5, p-value = 0.017); and QoL (RP, 23.6 ± 44.5, p-value = 0.042, and GH, 11.1 ± 14.2, p-value = 0.012).
Mobile Phone System Use: Thirty-six of the 42 patients (85.7%) used the mobile phone system and 6 patients (14.3%) never used it.
Discussion
This randomized controlled trial was the first of its kind, to our knowledge, to use a mobile phone Web browser messaging application that monitored daily weights and HF symptoms in a multiethnic, predominantly Hispanic, county hospital population for 3 months. The intervention improved self-efficacy and QoL among intervention participants compared with usual care.
Our mobile intervention improved the patients' chronic disease and HF-specific self-efficacy, their efficacy to communicate with physicians, and their QoL. It also improved health distress relative to the control group, in which health distress worsened. Earlier studies using nonmobile telehealth interventions show similar results. Dorsch et al. showed that a Web application used for symptom monitoring and links to HF goals and educational materials improved symptoms in systolic HF. 26 In two other studies, daily weight monitoring along with education improved knowledge and self-care implementation of daily weight monitoring. 27,28 However, these previous interventions used a combination of HF monitoring along with an educational component. 26 –28
Self-efficacy refers to the belief in one's ability to respond to challenges and carry out a behavior necessary to reach a desired goal. Increased self-efficacy is related to improved disease outcomes. 29,30 In fact, previous studies in diabetes and asthma have shown that self-efficacy rather than patient education or knowledge is vital in improving outcomes. 31,32 Our results are especially encouraging because improvement in self-efficacy occurred without a defined educational component in our mobile phone intervention. This suggests that a parameter-focused approach to symptom monitoring alone may reinforce the importance of daily monitoring and understanding of their condition among patients and promote good disease self-management skills and facilitate behavior change. It is also likely that increase in patient efficacy is not due to the frequent monitoring alone, but rather to the increased interactions with the healthcare system through the study coordinator, who contacted them whenever there was a response suggestive of deterioration of HF, such as weight gain, increased shortness of breath, or swelling in the feet. Our results are encouraging because they suggest that automated communications that trigger appropriate alerts and interactions with care providers in response to status changes may improve self-care efficacy. Seto et al. also evaluated the effects of a mobile phone-based telemonitoring system on self-care and clinical management of HF and showed that it improved QoL through improved self-care. 14 Our system was less automated compared with Seto's, with no automated feedback loop, except to ask participants to call their study coordinator and HF clinic. However, even our simple intervention of yes–no responses improved self-efficacy.
To the best of our knowledge, this is the first study of its kind to evaluate the use and outcomes of a cellular Web browser messaging program to monitor daily symptoms and engage predominantly Hispanic patients with HF in self-managing their disease. Even though the study was not powered to detect differences in healthcare utilization, by increasing self-efficacy, interventions such as ours may possibly help HF patients avoid costly events such as emergency visits and admissions when implemented in the immediate posthospital discharge period. Lee et al. recently demonstrated that self-efficacy is a key component of HF care in a randomized controlled HF trial wherein intervention patients used a symptom diary with education and counseling sessions compared with usual care. More intervention patients had event-free survival compared with usual care (78.3% active group versus 47.6% usual care; p = 0.03). 33 Another study reported that HF patients more engaged in self-management had a 56% reduction in mortality and healthcare utilization compared with patients who were less engaged in self-management. 34
Our intervention did not target knowledge. Therefore, it was no surprise that knowledge scores did not improve in the intervention group. However, knowledge scores did improve in the control group. Upon enrollment, all participants in both groups received some basic HF education reminding them to weigh themselves and information on monitoring and reporting positive symptoms, etc. This likely impacted knowledge more positively in the control group than the intervention group because the control group had significantly lower mean knowledge scores at baseline.
There are inherent limitations in the study, in that we cannot exclude sampling bias, the Hawthorne effect, and repeated testing bias that may have occurred during the study. We enrolled minority patients from the Heart Failure Clinic at a large county hospital, who may not be representative of the general population with HF. However, we attempted to negate these effects by the wide range of outcomes measured and by having a control group. In addition, several participants in both groups were seen in the Heart Failure Clinic during the study. Self-management teaching at any of these contacts, or simply improvement in health status, may account for the observed improvements. However, the fact that improvements in outcomes occurred after the intervention implicates a causal link. The cause and effect relationship is also suggested by the fact that the change in the control group was in the negative direction for several outcomes, including SECD, GH, HDS, and FVN. Although the sample size is small, the results are still positive; it is likely that a larger study would reveal more robust outcomes. A limitation of the study is that the intervention was too short to elucidate the benefits of daily monitoring and perhaps a longer intervention would have shown a greater impact. Future studies should validate these preliminary findings in a longer, larger randomized trial offered postdischarge from the hospital and assess their impact on healthcare utilization and cost.
Implementation of a mobile monitoring and reminder system that can increase self-efficacy and identify deterioration preemptively would be immensely beneficial. These promising results underscore the unique scalable opportunity mobile phones present to address the ethnic disparity and digital divide in HF management. More work is necessary to understand the key ingredients of successful intervention programs. The role of technology (for monitoring and/or education) versus case management in such programs and the role each plays in patient education, medication adherence, and preemptive intervention need further elucidation. 35 Besides mobile interventions to improve patient self-efficacy, further research will need to focus on development of sophisticated sensitive and specific algorithms for automated analysis of home monitoring data and to close the feedback and care loop to make mobile monitoring effective and efficient.
Footnotes
Acknowledgments
This research was supported by the Florida Department of Health's James and Esther King Biomedical Research Program, grant number 09KC-01.
The authors thank Bernard A. Roos, MD, Anne E. Burdick, MD, MPH, Sara Czaja, PhD, and Herman Cheung, PhD, for mentorship and guidance; Sandeep Dayanand, MD, and Silvana Cobian, MS, for helping with patient recruitment, data collection, and study implementation; Carlos Gomez-Orozco, BSc, and Diana Ruiz, BSN, for help with data management and manuscript preparation. The authors also thank the providers and staff in the Jackson Heart Failure Clinic for allowing them to work with their patients and collaborating with them on their care.
The authors gratefully acknowledge the support of the Geriatric Research, Education, and Clinical Center (GRECC), Bruce W. Carter Department of Veterans Affairs Medical Center, Miami, FL, and the Miami VA Research.
Disclosure Statement
Stuti Dang, MD, MPH: No competing financial interests exist.
Chandana Karanam, MD: No competing financial interests exist.
Orlando Gómez-Marín, MSc, PhD: No competing financial interests exist.
Findings in this article were presented, in part, at the 64th meeting of the American Geriatric Society and the American Telemedicine Association in 2012, the mHealth Summit, and the Bio-Florida/FL CURED Annual Conference in 2011.