
Abstract
Background:
A new age in communications began with the entry into use of cell phones and their applications. Cell phones and their various applications must be actively used in patient monitoring in the healthcare system.
Introduction:
The purpose of this study was to determine the length of stay in the pediatric emergency department observation unit (PEDOU) based upon the notification of abnormal laboratory results (ALRs) via the short message service (SMS).
Materials and Methods:
Patients with ALRs notified through the SMS (April–May–June 2015: study period) were evaluated retrospectively, and those admitted to hospital after such notification were enrolled as the study group (SG). Patients presenting to the pediatric emergency department (April–May–June 2014: control period), whose ALRs were not notified through the SMS, and who were hospitalized for treatment, were enrolled as the control group (CG). Age, sex, length of stay in the PEDOU (min), admission diagnosis, and receiving department were recorded for both groups.
Results:
Number of patients monitored in the PEDOU was 8584 during the study period and 8507 during the control period (p = 0.27). Length of stay of patients monitored in the PEDOU during the control period (n = 8507) and study period (n = 8584) was 136.4 and 133.5 min, respectively (p = 0.92). One hundred forty-seven patients were enrolled as the SG and 154 as the CG. Length of stay in the PEDOU was 221.1 ± 86.9 (65–542) min in the CG and 154.8 ± 76.6 (15–442) min in the SG (p < 0.001, 95% confidence interval: 47.5–84.8).
Conclusions:
Notification of ALRs through the SMS does not affect length of stay in the PEDOU. Use of this method reduces length of stay of patients who require more rapid hospitalization.
Introduction
A new age in communications began with the entry into use of cell phones and their various applications. The use of cell phones is increasing by the day in Turkey and worldwide. The number of cell phone subscriptions worldwide rose from 2.2 billion in 2005 to 6.9 billion in 2014. 1 The short message service (SMS) is a widely used application that entered into daily life together with cell phones. SMS allows a message consisting of 160 characters to be sent. 2 Some 9.6 trillion SMSs are now being sent worldwide every year. 3 SMS is used in all areas of life to provide services such as interpersonal communication, advertising, mass notifications, and Internet banking security codes. It is also not surprising that cell phones and their applications are actively used in health services.
Various factors such as age, characteristics of diseases, racial disparities, triage degree, emergency department structure, and overcrowding affect the length of stay in the pediatric emergency department observation unit (PEDOU). 4 –6 Overcrowding directly impacts on children because they exhibit higher visit rates than any other age group. 7 Length of stay in the emergency department observation room is also naturally affected by overcrowding in the emergency department. Commencement of treatment is, therefore, delayed and mortality rates rise as length of stay in the emergency department observation room increases. 8 Our observations show that monitoring of patients' laboratory test results is also difficult for physicians because of overcrowding.
The purpose of this study was to determine the effect of notification of abnormal laboratory results (ALRs) through SMS on length of stay in the PEDOU.
Materials and Methods
This research was planned as an observational study investigating the periods immediately before and after commencement of notification of ALR by means of SMS in the pediatric emergency department (PED). Written approval for the study was obtained from the Adiyaman University Biomedical Research Ethics Committee (No. 2016/2-11) and from the hospital administration.
This study was performed in the PED of a tertiary hospital with a total bed capacity of 600. The pediatric clinic has a total bed capacity of 118 (pediatric ward 65 beds, pediatric intensive care unit 11, neonatal intensive care 25, and PEDOU 17). On weekdays, two pediatric interns and one assistant professor of pediatrics are on duty in the PED from 08:00 to 16:00 h and also two primary physicians and one pediatric intern from 16:00 to 08:00 h. At weekends, two primary physicians and one pediatric intern work a 24-h shift in the pediatric intensive care unit. According to official figures, the population of the central part of the province served is 225,000, rising to 602,000 when the outlying districts are included. Trauma patients are not served in our hospital's PED.
In our hospital, the laboratory results unit has been integrated with physicians' cell phone numbers. Normal limits for test results in the laboratory were first uploaded to the system. The moment that the system perceives any result confirmed in the laboratory as an ALR, this is reported to the patient's physician through SMS. The SMS sent contains the patient's name and the ALR concerned. Our hospital purchased the SMS notification system at the same time as the software our hospital currently uses. The SMS examined in this study involved no extra costs for the hospital, and the procedure is a routine one in our institution.
Notification of ALR through SMS in our hospital began on April 1, 2015. This study constitutes a retrospective review of SMS records reporting ALR during the 3-month period between April 1 and June 30, 2015 (the study period). Patients hospitalized for treatment after notification of ALR were enrolled as the study group (SG). Patients hospitalized from the PED between April 1 and June 30, 2014 (the control period) were enrolled as the control group (CG). However, ALR notification through SMS was not used during the control period. Age, sex, length of stay in the PEDOU (min), admission diagnosis, and receiving department were recorded for both groups. The number of admissions to the PED, number of patients received by the PEDOU, length of stay in the PEDOU, and number of patients hospitalized from the PED during the study period and control period were also evaluated.
Patients with ALR notified by SMS but who were not hospitalized were excluded from the study because of the absence of any equivalent subjects in the CG. Patients with ALR notified by SMS outside the PED (polyclinics, neonatal intensive care, and pediatric intensive care), subjects outside the pediatric age group (>18 years), and pediatric patients with ALR notified by SMS in the trauma emergency department because of trauma were also excluded.
The data obtained were analyzed on SPSS (IBM, version 21.0, Chicago, IL) software. Categoric data are expressed as number and percentage and constant variables as mean ± standard deviation. The chi square test was used to compare categoric variables, Student's t-test was used in the comparison of normally distributed constant variables, and the Mann–Whitney U test was used for non-normally distributed constant variables. Statistical significance was set at p < 0.05. The number of patients monitored in the PEDOU during the control and study periods, length of stay of patients monitored in the PEDOU, and number of patients admitted to other departments from the PED were analyzed using the two rate test.
Results
The PED received 30,180 presentations during April–May–June 2015 (the study period) and 30,340 during April–May–June 2014 (the control period). Number of patients monitored in the PEDOU was 8,584 during the study period and 8,507 during the control period (p = 0.27). Mean lengths of stay of patients monitored in the PEDOU during the control period (n = 8,507) and study period (n = 8,584) was 136.4 and 133.5 min, respectively (p = 0.92). Number of patients hospitalized from the PED was 1,213 during the control period and 1,164 during the study period (p = 0.37). Nine hundred sixty notifications of ALR were made by SMS for the pediatric section during the study period. Two hundred nine (21.7%) of these represented notifications for the PED. Patients with ALR notified by SMS represented ∼2.4% of the patients monitored in the PEDOU. Sixty-two (29.6%) of the 209 notifications in the PED were not hospitalized for treatment, and these were excluded from the study.
The remaining 147 (68.6%) patients were finally enrolled as the SG. Seventy-eight of the 147 patients in the SG were male and 69 were female. One hundred fifty-four patients were enrolled in the CG, 81 males and 73 females. Demographic data for the SG and CG, receiving departments, and admission diagnoses are shown in Table 1. Mean length of stay in the PEDOU was 221.1 ± 86.9 (65–542) min in the CG and 154.8 ± 76.6 (15–442) min in the SG. Length of stay in the PEDOU was significantly shorter in the SG than in the CG (p < 0.001, 95% confidence interval: 47.5–84.8) (Fig. 1).
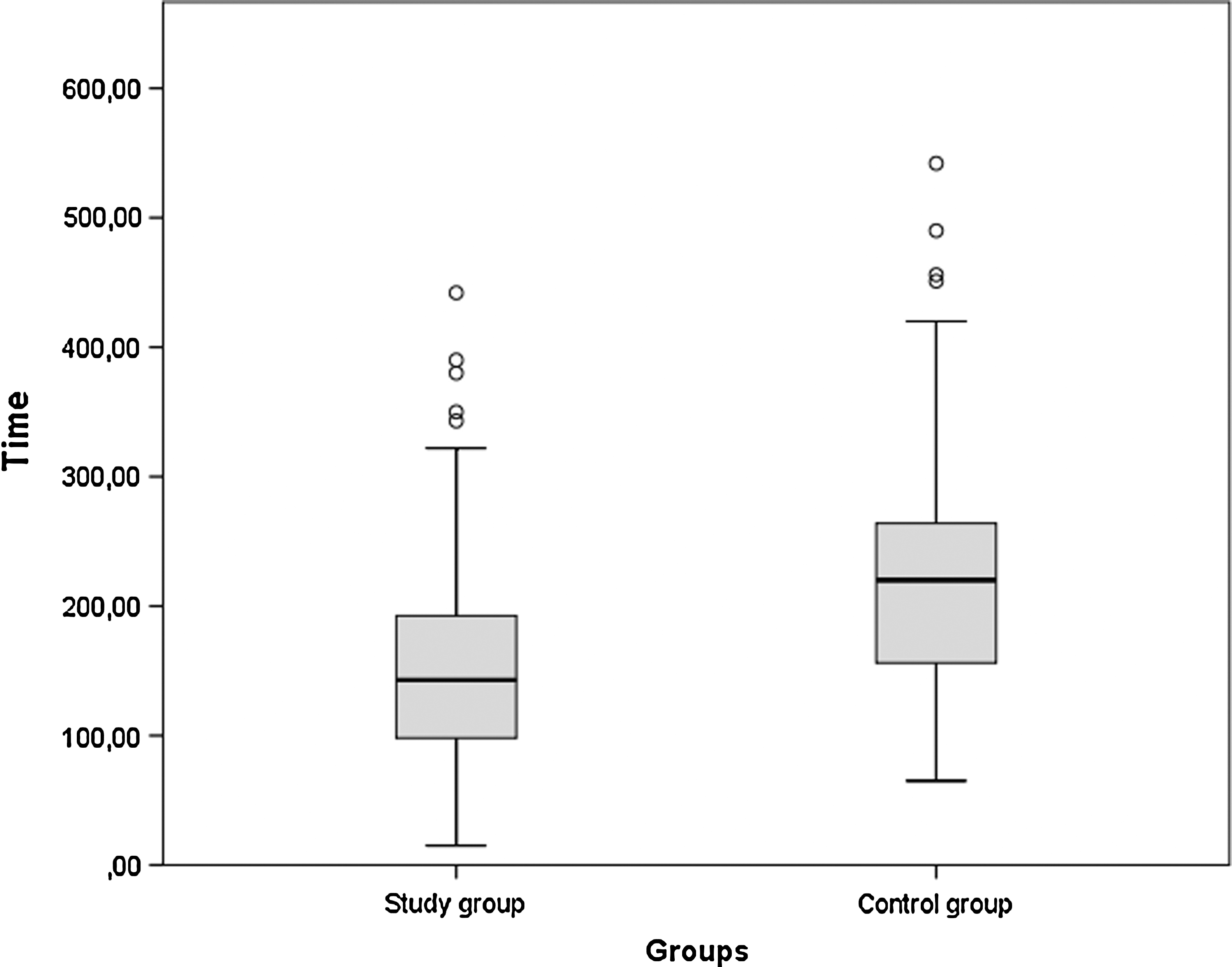
Length of stay in the pediatric emergency department observation unit in both groups (boxplot).
Demographic Characteristics and Data Concerning Admission Unit and Diagnosis for the Groups in the Study
Discussion
Communication through cell phones and SMSs is a simple procedure. SMS is a widely used system because it permits instantaneous communication and is also highly economical. Today's health system makes use of the new facilities provided by cell phone technology and uses SMS in various areas. Car et al. 9 reported using SMS to remind patients of medical appointments, Vervloet et al. 10 for compliance with regularly used medications, Horvath et al. 11 for compliance with antiretroviral therapy in HIV infection, de Jongh et al. 12 to support self-management of chronic diseases, Krishna et al. 13 for health results and care procedures, Dudas et al. 14 to monitor patients after treatment, Kwon et al. 15 to monitor blood sugar in diabetic patients, and Scheuermeyer et al. 3,16 for electrocardiogram and pulmonary X-ray consultation in the emergency department.
Emergency departments are units that attract large number of presentations, and various factors affect length of stay in them. Chaou et al. 4 reported that factors such as patient age and characteristics, time of day at presentation, and degree of emergency department triage determined length of stay in the emergency department. Brouns et al. 17 reported that more than one consultation and a large number of tests being requested prolonged length of stay. Handel et al. 18 showed that a high patient volume prolonged length of stay in the emergency department. Kocher et al. 19 identified requests for blood tests and imaging techniques as extending length of stay in the emergency department. Sun et al. 20 showed that large number of patients prolonged length of stay in the emergency department, while also increasing patient mortality and costs.
Our hospital's PED has a large patient capacity. Examination of the records showed that ∼330 patients per a day were examined in the PED during the study and control periods. It is probable that a number of ALRs will be missed in such a busy environment. Although there was no significant decrease in length of stay in the PEDOU when we notified ALR through SMS, the length of stay of patients hospitalized from the PEDOU was reduced to 66 min. We conclude that with the use of this application, patients requiring hospitalization were admitted and treatment was initiated more quickly. We think that the reason why notification of ALR by SMS did not affect time spent in the PEDOU is that patients with ALR notified by SMS represented only a very small proportion of all patients monitored in this unit.
No previous studies have investigated the effect of notification of ALR in the PED through SMS on length of stay in the PEDOU. Cho et al. 21 reported that if patients requiring consultation with a specialist physician are still receiving treatment in the emergency department 6 h after seeing the physician, they then issue an automatic reminder through SMS. They reported a 106 min shorter stay in the emergency department in that study. Bernstein et al. 8 reported that patient treatment was delayed and mortality rates increased when the emergency department was crowded. Seventy-four percent of the SG consisted of patients admitted to the neonatal intensive care and pediatric intensive care units. We also wish to note the presence of diseases such as early neonatal sepsis, acute kidney failure, and type 1 diabetes with ketosis, in which early treatment can be life saving, in this patient group. The treatment of these patients admitted for a shorter period will also probably be positively affected. This study is important as being the first of its kind and representing a model for busy hospitals.
Conclusion
Notification of ALR through SMS does not affect length of stay in the PEDOU. However, we recommend the use of notifications of ALR through SMS to identify patients in PEDs requiring more rapid hospitalization. Future long-term studies on this subject will elicit more valuable data about notifications of ALR through SMS in terms of mortality, morbidity, and economic costs.
Footnotes
Acknowledgment
We are grateful to Associate Prof. Nazif Calıs for support with the statistical analysis.
Disclosure Statement
No competing financial interests exist.