
Abstract
Background:
There have been few trials of interventions to facilitate recovery following mild traumatic brain injury (mTBI) in adolescence. To address this gap, we developed and piloted a novel Web-based intervention, entitled Self-Management Activity Restriction and Relaxation Training (SMART), and examined its impact on symptom burden, functional disability, and executive functioning during the month following mTBI in adolescents.
Materials and Methods:
Open-label, single arm study. Adolescents with recent mTBI and a parent were recruited from the emergency department and provided access upon discharge to SMART—a Web-based program designed to facilitate recovery via self-management and education about symptoms and sequelae associated with mTBI. Symptom burden, functional disability, and executive functioning were rated by both the adolescent and the parent initially and at assessments at 1-, 2- and 4-weeks postinjury. Mixed models analyses were used to examine trajectories on these outcomes.
Results:
Of the 21 adolescent/parent dyads enrolled, 13 engaged in the program and reported significant improvement in symptoms over the 4-week program (adolescent, p = 0.0005; parent, p = 0.004). Adolescents spent a median of 35.5 min (range 1.1–107.6) using the program. Parent ratings of the adolescent's functional disability and executive functioning significantly improved over the 4-week period from baseline (p = 0.009 and p = 0.03, respectively), whereas adolescents themselves did not report significant changes in either outcome. All participants improved and there were no adverse outcomes.
Conclusion:
The SMART program, a novel Web-based intervention, may serve as a self-management tool for adolescents and their parents to assist with the recovery following a recent mTBI.
Introduction
During adolescence, mild traumatic brain injuries (mTBIs), or concussions, pose a substantial societal burden due to their high incidence, associated loss of productivity, and risk of longer term morbidity. Many adolescents initially present to the emergency department (ED), accounting for over 280,000 ED visits annually in the United States and many more seek care in other settings. 1,2 For most, symptoms resolve within 2 weeks; however, up to 30% of adolescents will endure persistent somatic, cognitive, and/or behavioral symptoms beyond 1 month. 3 –5 Despite this burden, there is a paucity of interventions to facilitate postinjury symptom monitoring and management, particularly for adolescents. Consequently, national and international governing organizations have called for more trials investigating treatments to decrease morbidity associated with mTBI and improve quality of life. 2,6
The dearth of high-quality studies of interventions on mTBI is highlighted in three recent systematic reviews. 7 –9 Only three clinical trials targeting adolescents acutely after the initial injury were identified, 10 –12 all of which focused on early anticipatory guidance primarily in the form of educational pamphlets, with two trials demonstrating decreased symptom burden compared to controls. 10,12 Cognitive and physical rest followed by a graduated return to activities is also a cornerstone of management after the injury, although evidence regarding effectiveness is lacking. 13 –15 In addition, there is support for the benefits of cognitive behavioral therapy and relaxation training following mTBI in adults. 9,16 Current ED care typically incorporates provision of written discharge instructions focused on anticipated symptoms and guidance on return to activities. 17 This is usually followed by biweekly outpatient visits until symptom resolution. This approach fails to provide real-time tracking and individualized guidance based upon symptom burden and does not elicit or impart information in an engaging, age-appropriate, easy-to-use platform. Furthermore, it is time-consuming and inconvenient, contributing to diminished productivity for both parents and adolescents.
Web-based self-management programs may fill this critical gap by providing timely, sensitive, and readily accessible resources to address the varied consequences of mTBI. Successful self-management platforms incorporate fundamental information, as well as dynamic and multidimensional processes to enhance symptom recognition and promote self-awareness and metacognition. 18,19 Attendant behavioral changes are expected to improve disease control and reduce service utilization. Online self-management programs are promising for adolescents with migraines and with more severe TBI, yet a Web-based intervention to assist with postinjury self-management following adolescent mTBI has not been tested. 20 –24 In the case of mTBI, a program delivered early designed to improve self-efficacy around managing recovery has the potential to reduce economic burden related to medical visits, enhance quality of life, facilitate return to daily activities, and mitigate stress on families and patients. A key aspect to successful integration of the program will be to ensure it does not adversely affect recovery.
To address this gap, we developed and beta-tested a Web-based intervention to promote concussion recovery for adolescents through education and training in self-management and effective coping. The program, entitled Self-Management Activity Restriction and Relaxation Training (SMART) is comprised of two components: (1) daily symptom and activity monitoring, along with personalized feedback and probes to promote tailored self-management of symptoms, and (2) educational modules incorporating principles of anticipatory guidance, problem-solving training, and stress management/relaxation training. The results of usability testing and preliminary feasibility have been reported previously. 25 –27 The current pilot study reports symptom burden and functional disability during the initial month following participation in SMART.
Materials and Methods
Study Design
This was a prospective open pilot study involving adolescents, ages 11–18 years, who presented within 96 h of a mTBI to the ED affiliated with a large children's hospital between October 2013 and August 2014. The Institutional Review Board approved the study.
Participants
Eligible patients had a Glasgow Coma Scale (GCS) score of 13–15 on presentation and sustained either a witnessed blow to the head, an injury with acceleration/deceleration movement of the head, or a self-reported injury with evidence of head trauma. Additional criteria included loss of consciousness < 30 min, amnesia, or any alteration in mental state at the time of the injury (e.g., agitation, irritability, sleepiness, lethargy, slow to respond, or asking repetitive questions). 28 Patients were required to be English-speaking and have Internet access at home. Patients were excluded if they had more than one extracranial injury with an Abbreviated Injury Severity Scale > 4 to that region, 29 presented with an altered mental status due to the ingestion of substances that may impair cognition, or had preexisting neurologic, psychological, or developmental delays. Patients with attention-deficit/hyperactivity disorder on two or more medications were also excluded.
Study Procedures
Research coordinators screened patients based on age and related chief complaints, verified inclusion and exclusion criteria with the medical team and patient's family, and obtained parental consent and adolescent's assent. Study measures were collected using the Research Electronic Data Capture (REDCap) platform, a free, Web-based application for collecting structured, secure data for research studies. 30 Patient demographics (age, sex, and race), injury descriptors, and obtainment of computed tomography (CT) neuroimaging were documented to characterize the cohort. Routine clinical care was directed by the ED provider. Upon ED discharge, both the adolescent and their parent received unique log-on IDs, passwords, and instructions on how to access and use the program.
The Smart Program
The SMART program consists of two components: (1) symptom and activity monitoring to promote self-management; and (2) educational modules providing education and skill training as detailed in Figure 1.
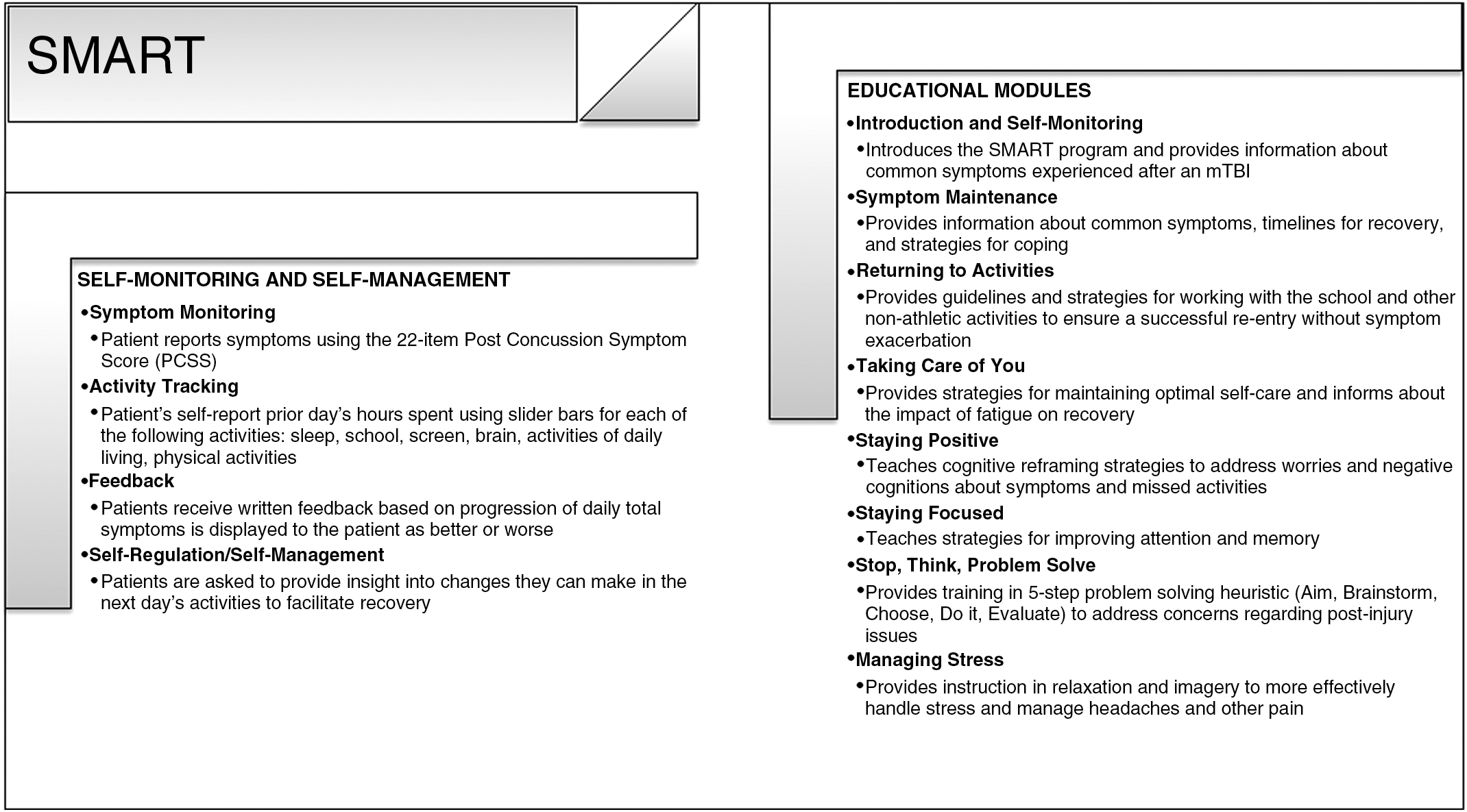
Overview of the SMART program. SMART, Self-Management Activity Restriction and Relaxation Training.
Self-management component
At each logon, adolescents rated their daily symptoms using the Post-Concussion Symptom Scale (PCSS)—a scaled severity rating of 22 common symptoms (total range 0–132), 31 and a self-report log of the prior day's activities in the domains of brain/cognitive, screen time, sleep, school, activities of daily living, and physical activity. Adolescents received feedback regarding whether their symptoms were better, the same or worse, based on changes in their PCSS scores. To promote awareness and facilitate self-management, they were asked how they could change their activities the next day to help with recovery (e.g., more sleep).
Educational modules
After completion of the self-management component, adolescents were prompted to complete educational modules that provided anticipatory guidance and techniques to effectively manage these consequences using cognitive reframing, relaxation training, and problem solving. Materials included videos, graphics, and written didactics with audio-voice over. Order and rate of module introduction were based on logic created by two of the authors (L.B. and B.G.K.) who integrated initial symptom burden, daily symptom burden, and time since injury, in conjunction with normative data 32 and physician consensus (L.B. and B.G.K.). Availability of modules was dependent on symptom burden; for adolescents with lower severity of symptoms, all modules were made available within 48 h after injury, whereas those with higher initial severity and/or high daily symptom burden, modules were introduced over a 1-week period. We categorized symptom burden as: no or very mild (PCSS score ≤8), mild (score 9–14), moderate (score 15–30), severe (score 31–49), or very severe (score 50–132). During the latter weeks, participants received an email after completion of the PCSS to complete modules that had not been completed and refer to earlier modules to refresh skills. All modules were open for parents from the initial log-on and they also received online information regarding graduated return to activities and return to school/academics. Based on prior testing, each module required 5–10 min to complete with the entire program taking 40–80 min.
Outcome Measures
Primary outcome measures included symptom burden, measured by the Health and Behavior Inventory (HBI) 33 ; functional disability, measured by the Functional Disability Inventory (FDI) 34 ; and executive functioning, measured by the abbreviated version of Behavior Rating Inventory of Executive Functioning (24-items, brief-BRIEF). 35,36 Higher scores on each of these measures reflect greater impairment. The HBI assesses the frequency of 20 symptoms over the past week, each rated as 0 = never, 1 = rarely, 2 = sometimes, and 3 = often. In the ED, these measures were completed by parents as a proxy to preinjury baseline assessment. The adolescent HBI completed in the ED assessed acute symptom burden. The HBI and the FDI were completed again by both the parent and adolescent at 1, 2, and 4 weeks following injury. The brief-BRIEF was completed by both the parent and adolescent again at 2 and 4 weeks. Measures were not administered at 3 weeks to limit respondent burden given the expectation that most recovery occurs during the initial 2 weeks. Secondary measures, assessed only twice, in the ED as a preinjury baseline and again at 4 weeks, included behavior problems on Child Behavioral Checklist (CBCL) and Youth Self Report (YSR) 37 ; and parent and adolescent concussion knowledge on the 10-item CDC Head's Up concussion quiz. 38 PCSS, assessed at every log-on, was used to measure severity of symptoms and assist with self-regulation, not to assess program effectiveness. 27 Adolescent usage was based on number of log-ons and time spent at the site. Parent time spent on the Web site was not able to be extracted due to a programming error.
Analysis
Participant demographics were characterized using descriptive statistics. We compared characteristics of participants and nonparticipants using t-tests and chi-square analyses. Linear mixed models were used to assess change over time for adolescent- and parent-reported outcomes, with premorbid functioning included as a covariate when available. For the HBI, the parent-report from the ED served as a proxy for preinjury symptoms in analyses of adolescent-reported HBI because it is impractical for acutely concussed adolescents to rate preinjury symptoms and modest agreement between dyads on the HBI at other time points has been reported. 39 Spearman correlation analyses assessed associations between parent and adolescent report on the HBI, FDI, and brief-BRIEF. We performed all analysis using SAS/STAT software (version 9.3; SAS Institute, Inc. Cary, NC). p-Values of <0.05 were considered statistically significant.
Results
Of the 546 patients screened for eligibility, 47 were eligible and approached (see Study Flow Diagram; Fig. 2). Twenty-one adolescent-parent dyads consented and completed study measures in the ED, and 13 adolescents logged into the SMART program. The remaining eight adolescents did not access SMART and were unable to be contacted for follow-up, hence causes of inactivity are unknown. Three parents logged into the system a single time, although their child did not logon. Adolescents who used the program had similar demographic characteristics to those listed in Table 1 and baseline scores on outcome measures collected in the ED to those who did not use the program (all p > 0.05), except those who used the program were more likely to be white (p < 0.05). The median number of interactions was 6 (range 2–11) and the median time spent using the program was 35.5 min (range 1.1–107.6). Parents of users had a median of 4 interactions (range 0–8) with SMART.

SMART study flow diagram.
Characteristic of Patients Engaged in the SMART Program
CT, computed tomography; ED, emergency department; GCS, Glasgow Coma Scale; SD, standard deviation.
After statistically controlling for parent preinjury ratings, symptom burden as rated both by the adolescent and parent declined over time as shown in Table 2 (HBI-adolescent, p = 0.0005; HBI-parent, p = 0.004). For adolescents, the primary difference was between the first and second weeks, and there was a significant decline in symptoms between the first week and each later visit. Forty percent and 66.7% of adolescents were below parent-reported preinjury levels on the HBI at 2 and 4 weeks respectively. With respect to FDI, there was a significant decline in the parent ratings (p = 0.009) and a nonsignificant decline in adolescent ratings (p = 0.07), over time. Similarly, parents, but not adolescents, noted improvements in executive functioning (brief-BRIEF) over the 4-week period (p = 0.03). Between the dyads, there were strong correlations on the ratings of the HBI post-ED (r = 0.69, p < 0.001) and moderate correlations on both the FDI (r = 0.5, p = 0.0003) and brief-BRIEF (r = 0.35, p = 0.03). 40 The ratings on the HBI conducted in the ED were not correlated, as parents rated preinjury symptoms and adolescents rated their symptoms at the time of injury.
Outcomes for Patients That Engaged with the SMART Program
At each follow-up time point, the number stated here is the highest number that completed some measure at that point.
Change over time controlling for premorbid baseline assessment of measures collected in the ED.
brief-BRIEF, abbreviated version of Behavior Rating Inventory of Executive Functioning; CBCL, Child Behavioral Checklist; FDI, Functional Disability Inventory; HBI, Health and Behavior Inventory; YSR, Youth Self Report.
Improvements in adolescent-reported HBI, FDI, and brief-BRIEF were not associated with usage as defined by number of interactions with SMART. Similarly, improvements in FDI and brief-BRIEF did not significantly differ as a function of time on the spent program. Although nonsignificant, examination of the interaction between follow-up visit and time spent on the program was associated with decreased HBI scores (p = 0.06), indicating that greater time spent on the program was associated with quicker recovery or at least, unlikely to worsen recovery. Additional assessments of behavior problems (parent CBCL, adolescent YSR) and concussion knowledge did not change significantly from baseline to the 4-week assessment (Table 2).
Discussion
Results from this open-pilot indicated declining symptoms following mTBI during usage of a novel Web-based intervention that combined symptom monitoring, activity self-management, and educational modules. Functional disability and executive functioning of the adolescents as reported by parents improved significantly during the period of engagement with SMART; however, adolescents themselves did not report significant improvements. Importantly, the initiation of the SMART program early after injury was not associated with worsening of symptoms or increased disability, indicating that delivery of a Web-based intervention soon after injury is likely safe and feasible. Our prior work indicated that the program was easy to use and intuitive. 25 To our knowledge, SMART is the first Web-based intervention initiated in the ED to help adolescents and their parents cope with mTBI symptoms. SMART is unique in its use of real-time, tailored guidance to promote gradual return to daily activities. The small sample size, inability to fully characterize the enrolled children that did not initiate the program, and lack of a control group preclude our ability to assess the effectiveness of this intervention as compared to natural disease progression and recovery. Nonetheless, this type of Web-based management program addresses the call for interventions and offers the advantages of being personalized, low-cost, accessible, and scalable.
More frequent use of SMART was not associated with more rapid recovery; however, there was a trend toward significance in the interaction between use and the self-reported HBI. There may be an optimal time of exposure to the intervention content and symptom improvement, with both a lower limit and a plateau effect of the impact of SMART on symptoms and functioning. In our study utilization varied widely. The variation in program usage could be due to variations in recovery and symptom burden. Those with fewer symptoms and rapid recovery had little need for such a program; or conversely those with more severe symptoms may have deterred use of the program. Although it is assumed parents act as key care facilitators, the lack of capture of parental time interacting with SMART prohibits the assessment of the parental dose effect relationship of SMART. Some adolescents may have also avoided usage due to conflicting messages about avoidance of screen time postinjury; however, it is reassuring that program use did not exacerbate symptoms. Design and formatting issues may have contributed to lower than anticipated program usage. Specifically, reliance on a Web-based platform, text-heavy content, and the requirement to complete PCSS and activity ratings before accessing the psychoeducational content may have reduced engagement. Transformation into a mobile platform may promote adolescent participation since 74% say they access the Internet on cell phones and other mobile devices at least occasionally. 41
Two-thirds of adolescents were back to baseline by 4 weeks, which is consistent with the literature of rapid recovery for most adolescents following mTBI. 3 Although time since injury could affect symptom burden, the majority of our cohort were enrolled within 1 day of injury. Heterogeneity in injury severity even among those with mTBI may also affect symptom burden and trajectory, yet our cohort had substantial initial symptoms and almost half of them were judged to warrant CT imaging. As previously reported, both adolescents and parents rated the program as informative and useful, suggesting that participants may experience benefits other than symptom improvement, such as improved well-being and reduced worries about recovery. Subsequent studies should risk stratify the population targeting those at highest risk of persistent postconcussive symptoms 4 and include a usual care or attention control group to determine the impact of SMART in facilitating recovery and reducing injury-related fears.
SMART provided adolescents with graphic feedback about their symptom progression and recommendations for modulating participation levels based on whether symptoms were improving or worsening. Given the variability in individual symptom burden and timing of recovery, the SMART platform empowered adolescents to manage their own recovery, based on knowledge about their symptom levels. Although a paradigm in the management of adolescents with mTBI continues to be cognitive and physical rest for prolonged duration, there are several reports suggesting that prolonged rest may be in fact detrimental and increase symptom burden. 15,42 Thus, in designing the program, we sought to promote engaging in everyday activities as soon as possible. The impact of earlier re-engagement facilitated by this program on school absenteeism and parental productivity should be assessed in future studies.
This initial study has several limitations, in addition to those previously mentioned. Since patients with concussions present to the ED with diverse chief complaints the research coordinators screened using broad criteria, resulting in several ineligible candidates. We had lower than desired usage rates and the rate of recovery for the adolescents who did not use the program is unknown. Lack of assessments of preinjury functioning and use of ones completed in the ED as proxy measures may introduce recall bias, especially for the concussed adolescent. Using the parent-reported HBI-ED as a proxy for the adolescent's preinjury symptom burden may fail to accurately measure preinjury functioning, yet there was a strong correlation between dyads on the HBI at other time points. Functional disability, impairments in executive functioning and behavioral problems were minimal from the onset and were within the range for normal adolescents perhaps creating floor effects that limit our ability to detect improvements. 34,35 Similarly, preexisting knowledge about concussion was high. Inclusion of multiple measures to assess program effectiveness may contribute to evaluator fatigue and thereby diminish the real-world effectiveness of an intervention of this kind.
This open pilot sought to assess the impact of SMART on symptoms, functional disability, and executive functioning and to inform the design of a larger trial. Given the high incidence of mTBI and associated morbidity in adolescents, there is a need for an evidence-based self-management program for mTBI in this age group. Evidence suggests that the SMART program provides useful information in monitoring recovery from mTBI without hindering it, yet whether SMART actually promotes more rapid recovery will require further study.
Footnotes
Acknowledgments
Funding for this study was supported in part by the Ohio Department of Public Safety and Cincinnati Children's Research Foundation Place Outcomes Grant. During the grant period, Dr. Kurowski was supported by K23HD074683. We acknowledge the exemplary work of Nicole McClanahan, Sunny Thakkar, Alexandra Talks, and Stacey Raj for their assistance with the development of the program and the research coordinators in Division of Emergency Medicine of Cincinnati Children's Hospital Medical Center for their recruitment efforts. We would also like to acknowledge the assistance of Jennifer Collins, for the Division of Biostatistics for her assistance with data analysis.
Drs. Babcock, Kurowski, and Wade conceptualized and designed the study, obtained funding, conducted the study, analyzed and interpreted the data, drafted the initial article, revised the article, and approved the final article as submitted. Dr. Dexheimer assisted with program design, reviewed and revised the article, and approved the final article as submitted. Mrs. Dyas assisted with study conduct, reviewed and revised the article, and approved the final article as submitted. Dr. Zhang analyzed and interpreted the data, reviewed and revised the article, and approved the final article as submitted.
Disclosure Statement
No competing financial interests exist.