
Abstract
Background:
Although the use of telepractice in speech–language therapy for assessment purposes is well documented, its effectiveness and potential for rehabilitation in poststroke aphasia remain largely unknown. The purpose of this study was to investigate the effectiveness of a remotely delivered synchronous pragmatic telespeech language therapy for improving functional communication in aphasia.
Methods:
A pre-/post-test design was chosen in which each participant was his or her own control. Using a telerehabilitation platform and software (Oralys TeleTherapy) based on the Promoting Aphasics' Communicative Effectiveness (PACE) approach, 20 participants with chronic poststroke aphasia received 9 speech therapy sessions over a 3-week period.
Results:
Teletreatment with the PACE pragmatic rehabilitation approach led to improvements in functional communication, marked by (a) an increase in communication effectiveness, reflecting significantly improved autonomy in functional communication; (b) a decrease in communication exchange duration, meaning that the treatment made communication faster and more efficient; (c) a decrease in the number of communication acts, meaning that, after treatment, less information was needed to be efficiently understood by the communication partner; and (d) an increase in the number of different communication strategies used, meaning that the treatment fostered the use of a variety of alternative communication modes.
Conclusions:
This study provides additional arguments about the benefits of telerehabilitation for poststroke patients with aphasia. It showed that multimodal language therapy delivered through synchronous telerehabilitation had positive effects on functional communication in chronic aphasia.
Introduction
Aphasia, an acquired language disorder after brain injury, most commonly stroke, has dramatic repercussions not only on the affected person's quality of life but also on his or her family. 1 Aphasia causes difficulties in language comprehension and/or production, which compromises the communication skills of the person. Aphasia also reduces the individual's social interactions, 2 which leads to significant and often long-standing personal limitations. The potential impact of language therapy for persons with aphasia is, therefore, of great interest.
The prognosis of aphasia depends on several factors, including its etiology and the impact of speech therapy. In poststroke aphasia, this therapy is based on a collaborative care approach that usually begins at the hospital in the acute phase, continues in intensive rehabilitation programs, and ends at home or during weekly visits to an outpatient clinic. However, getting to an outpatient clinic is sometimes difficult or impossible because of mobility difficulties, the need for support from a family member, the distance between home and clinic, and so on. Home therapy could be an interesting option for these patients, but is rarely available in language rehabilitation services. In Quebec and Canada, home services cannot currently meet demand because of personnel and financial constraints, particularly in speech–language pathology. New strategies for delivering these services are, therefore, needed to increase access to speech therapy rehabilitation. Telerehabilitation is a new approach in the field of rehabilitation that allows patients to receive treatment in the comfort of their own home and without the practitioner having to travel. This innovative way of providing rehabilitation services could help increase accessibility in both rural and urban areas. 3
In speech–language pathology, this service delivery method was successfully used for the assessment of various clinical populations presenting with dysarthria, 4 speech and voice impairments, 5 apraxia of speech, 6 aphasia, 7 etc. Telerehabilitation was also used in a few studies on aphasia treatment. For example, we used a custom videoconferencing system to remotely deliver language treatment to three individuals with chronic aphasia. 8 After 6 weeks (twelve 1-h sessions) of telespeech therapy, their performance on confrontation naming of trained items improved significantly and they had high scores on a satisfaction questionnaire. The accelerated development of new technologies gives clinicians the opportunity to offer innovative and intensive treatments, in which the person with aphasia is autonomous or needs less support. However, the effectiveness and potential of telerehabilitation for language rehabilitation in aphasia remain largely unknown. There are only a few studies, and those published to date are heterogeneous in terms of software and remote techniques, clinical presentations of participants, and treatment methods. Therefore, further studies are needed to document and establish the clinical value of telespeech therapy for the management of aphasia. In this context, the main objective of this study was to investigate the effectiveness of a remotely delivered pragmatic treatment for improving functional communication in individuals with chronic aphasia.
Methods
Design
A quasi-experimental pre-/post-test design was used, in which each participant was his or her own control. The study had four main phases: (a) Phase 1 included a general background assessment of language designed to verify selection criteria (T0), (b) Phase 2 involved baseline measures administered twice (T1, T2); (c) Phase 3 encompassed the 3 weeks of telespeech therapy (T3 measure); and (d) Phase 4 consisted of follow-up measures, 6 weeks after the end of the intervention (T4). Clinical outcomes were also recorded at each session throughout the treatment, allowing for analyses of changes in performance during the treatment.
Participants
The sample was composed of individuals with chronic poststroke aphasia, recruited through lists and referrals of patients from the Centre hospitalier universitaire de Sherbrooke, Institut de réadaptation en déficience physique de Québec, Centre de réadaptation Estrie, and Association québécoise des personnes aphasiques. The study was approved by the local institutional ethics committees for the safety of human subjects, and written informed consent was obtained from all participants.
Inclusion and exclusion criteria were formulated to exclude potential spontaneous recovery and ensure a stable neurological profile. Participants had to present with chronic aphasia secondary to a first and unique left hemisphere stroke. They had to be at least 1 year poststroke to avoid any influence of spontaneous recovery 9 and present moderate to severe anomia (score ≤20/31 on the picture naming subtest of the Montréal-Toulouse Aphasia Battery [MTAB]). 10 Finally, a family caregiver was needed to be available during the speech therapy sessions. Exclusion criteria included (a) comprehension deficits severe enough to impair comprehension of treatment tasks (score ≤6/9 [words] and ≤18/38 [sentences]) on the designation subtest of the MTAB, (b) unawareness of communication difficulties (score ≤3/5 on the anosognosia subtest of the Protocole Montréal d'Évaluation de la Communication [MEC]), 11 (c) receiving conventional speech therapy at the same time as participation in the study, (d) impaired and uncorrected hearing or vision (questionnaire), and (e) other neurological disease (e.g., dementia and Parkinson disease). Eligibility for the study was verified during Phase 1 (T0).
Principles of the Promoting Aphasics' Communicative Effectiveness Approach
There are many different approaches to the treatment of aphasia. 12 Some of them aim to restore communication abilities, whereas others draw on compensatory or pragmatic strategies to enhance functional communication. Among the pragmatic strategies, the Promoting Aphasics' Communicative Effectiveness (PACE) approach 13 is one of the most commonly used discourse-level treatments. This approach is used to improve conversation in persons with aphasia through clinical activities containing all the elements of face-to-face communication (i.e., equal participation of clinician and client, exchange of new information, use of all communication channels, and feedback aimed at working out the client's message). 14 The efficacy of PACE was demonstrated in studies exploring naming abilities 15 as well as functional 13 and referential communication. 16 This approach has many advantages: it provides individuals with the experience of communicating successfully, is suitable for any aphasia type, can be tailored to individual needs, and aims at generalization effects rather than item-specific effects.
Selection of Treatment Stimuli and Baseline Measures
After the recruitment interview (T0), each participant was administered a picture naming task comprising 380 stimuli from 2 picture data sets. 17,18 Items for which naming was incorrect, absent, or delayed (+10 s) were selected and presented again for naming at the second session, before baseline 1 (T1). This method was used with each participant to select 60 items for which naming was consistently impaired.
Baseline measures with the 60 selected items were taken twice using the PACE approach, 13 in which participants were instructed to pick the picture card of each item in random order and give the evaluator enough information about it for him or her to be able to identify the item. No precise rules were given, other than that participants could use any means available, including pen and paper. The evaluator had to guess the name of the item whenever he or she was confident about its identity. If the participant initially failed to give enough information, the evaluator gave general feedback regarding his or her inability to identify the item (e.g., “I'm not sure, can you give me more information?”). If the item still could not be identified, the evaluator gave specific feedback suggesting a type of information that could help him or her identify the item (e.g., “I'm still not sure, could you draw it?”). If after all these tries the evaluator still could not identify the item, the communication exchange was considered to have failed and the next item was selected. Scoring the communication effectiveness for each trial depended on the involvement of the evaluator required in the exchange. Table 1 details the scoring procedure, adapted from Davis. 19 In addition to the effectiveness score, other variables measured included communication exchange duration, number of communication acts, and variety of communication strategies used (alternative modes/number of pieces of information).
Promoting Aphasics' Communicative Effectiveness Scoring Procedure
This PACE approach was followed at each baseline (T1 and T2) on these same 60 items presented in random order. Using the communication effectiveness score and number of communication acts produced, the items were then divided into two 30-item lists of comparable performances. One of the lists was selected for the treatment, whereas the other served as a control list. The same procedure for the 60 items was used in the post-treatment evaluation (T3) and follow-up session (T4).
A verbal fluency test (MEC's three fluency conditions: free, semantic, and orthographic) 11 was also administered to the participants as a control task at T2 and T3. The aim of this task was to verify that no linguistic improvement unrelated to the treatment occurred in the participants, just by being more exposed to communication situations over a 3-week period. This specific task was selected because verbal fluency involves spoken production but requires different abilities than those required in the PACE treatment.
Telerehabilitation System
To use the PACE approach in telerehabilitation, a speech TeleTherapy software platform was developed in collaboration with a private company (Oralys, Inc.). This software (Fig. 1) implements a PACE session by displaying an array of images on both the clinician and client sides, randomly selecting an image and managing the turns, providing tools (chat area and drawing area) and research metrics (number of visual, written and gestural cues used in a sequence, and number of general and specific hints required to correctly guess the image, success/failure of the turn). Audio and video interactions during interventions are supported by a videoconferencing system (Tandberg 550 MXP), which uses h.264 video codec and integrates a pan-tilt-zoom wide-angle camera and omnidirectional microphone. The system is mounted over a 25.5-inch Touchsmart embedded computer, which displays the video received from the other end, and enables user interaction with the Oralys TeleTherapy software.

Telerehabilitation platform and software interface. Published with permission.
Telespeech Therapy Using the Pace Approach
During the 3-week intervention period, participants attended three therapy sessions per week, for a total of nine sessions (S1–S9). Three different speech therapists took it in turns to provide treatments to reduce habituation to the patient.
The intervention was tailored to each participant by using the 30-item list individually compiled at baseline. The general goal was to encourage alternative communication strategies using an adapted procedure based on the PACE pragmatic rehabilitation approach. 20 Thus, during a session, therapist and participant alternated as transmitter and receiver to guess the chosen item from verbal (words and description) or nonverbal instructions (drawing, writing, and mime). For each turn, the software randomly selected six images from the list and displayed them on both sides (participant and clinician). One of the images was randomly chosen by the software as the current work image, ensuring that it had not already been selected in the current session. Using visual aids (drawing area with a stylet used with the touchscreen, keyboard typing area, and camera for gestures) and audio aids (for speech), clinician and patient are able to communicate to get the other party to guess the selected image they have on their side for each of the 30 turns in the session.
The clinician's version of the software recorded all of the same variables as those measured in the pre-/postevaluations. Only the turns in which the participant was the transmitter were used for the analyses; the clinician's turns served only as a communication model.
Outcome Measures
The following outcome measures were taken during both the evaluations and the nine telespeech therapy sessions. All these measures were directly derived from the PACE administration manual. 19 The primary outcome of interest was the PACE communication effectiveness score. For each transmitted image, participants received a score out of 4, based on the scoring procedure detailed in Table 1. Communication exchange duration, expressed in seconds, was also measured because this variable reflects communication speed, which is also an indicator of communication effectiveness. The average number of communication acts (i.e., number of communication acts needed to transmit the message) is another variable pointing to the quality of communication exchanges. Stability or an increase in this average number could reflect the inefficacy of telespeech therapy, whereas a decrease could be interpreted as an improvement in communication effectiveness (less information needed to be efficiently understood). Finally, the variety of communication strategies used (i.e., spoken message, written message, and gestures) is also one of the outcome measures in the study. It was calculated by dividing the number of strategies used for any given item by the amount of information transmitted.
The participants' performance in the three conditions of the verbal fluency test was measured at T2 and T3. In the free condition, participants were asked to close their eyes and produce as many words (no proper names or numbers) as they could in 2 min. 30 sec. In the orthographic condition, participants had to produce as many words as possible beginning with P in 2 min. Finally, in the semantic condition, they had to generate as many words as possible from the clothing category in 2 min.
Statistical Analyses
The effects of treatment (pretreatment, T1 and T2 vs. post-treatment, T3 and T4) and treatment list (treated vs. untreated) on each variable in the study were analyzed using a mixed-model analysis of variance. Treatment and treatment list variables were entered in the model as random factors, based on an unstructured covariance matrix, which allowed for unequal variance between each repeated measure. 21 Participants were entered in the model as a random factor based on a scaled identity covariance matrix. Finally, all the dependent variables (communication effectiveness, communication exchange duration, average number of communication acts, variety of communication strategies used, and performance [number of words] in the three conditions of verbal fluency) were analyzed using the treatment variable and treatment list as fixed factors.
For the within-treatment analyses, only the effect of treatment progression (S1–S9) on each variable was analyzed. A similar mixed-model procedure was used. Because there was just one list of treated items during treatment, only the progression of the treatment was entered as a fixed factor. When appropriate, post hoc analyses (pair-wise comparisons) were conducted on the repeated measures using Bonferroni corrections.
As mixed-model analyses typically yield greater significance values because of their greater sensitivity, a statistically significant threshold of p < 0.01 was used in this study. All statistical analyses were done using SPSS v.20 (IBM Corporation, 2011). The mixed-model procedure used in this study followed guidelines suggested for speech and language research using repeated measures to avoid statistical problems. 22
Results
Description of the Sample
The sample was composed of 20 participants (14 male), with ages ranging from 49 to 78, and time poststroke from 2 to 29 years. Demographic data and initial language performance for the participants are presented in Table 2.
Demographic Data and Initial Language Performance for Participants
Montréal-Toulouse Aphasia Battery, naming subtest.
Montréal-Toulouse Aphasia Battery, word comprehension subtest.
Montréal-Toulouse Aphasia Battery, sentence comprehension subtest.
Data Pooling
Preliminary analyses showed no statistical difference for any of the variables between the two baseline measures and between the two post-treatment measures. This result indicates that the participants were in a stable condition before treatment and that treatment outcomes were still present 3 weeks after the last treatment session. Subsequent analyses were thus done pooling the data obtained at baseline (indicated as “pretreatment” from now on) and the data obtained after the treatment (indicated as post-treatment).
Pre-/Post-Treatment
Figure 2 displays group results on the four analyzed treatment outcome measures averaged before and after treatment, for both lists (when applicable). Regarding the average PACE communication effectiveness scores (Fig. 2a), statistical analyses indicate a significant effect of treatment, with an increase in communication effectiveness after treatment: F(1.20) = 27.07, p = 0.000043. No significant list (p = 0.02) or list × treatment interaction (p = 0.02) effects were found. These results indicate that the improvement in communication effectiveness was treatment specific, and this outcome was generalized to the untreated list. On the individual level, all participants except one (C17) followed the group trend (95%).
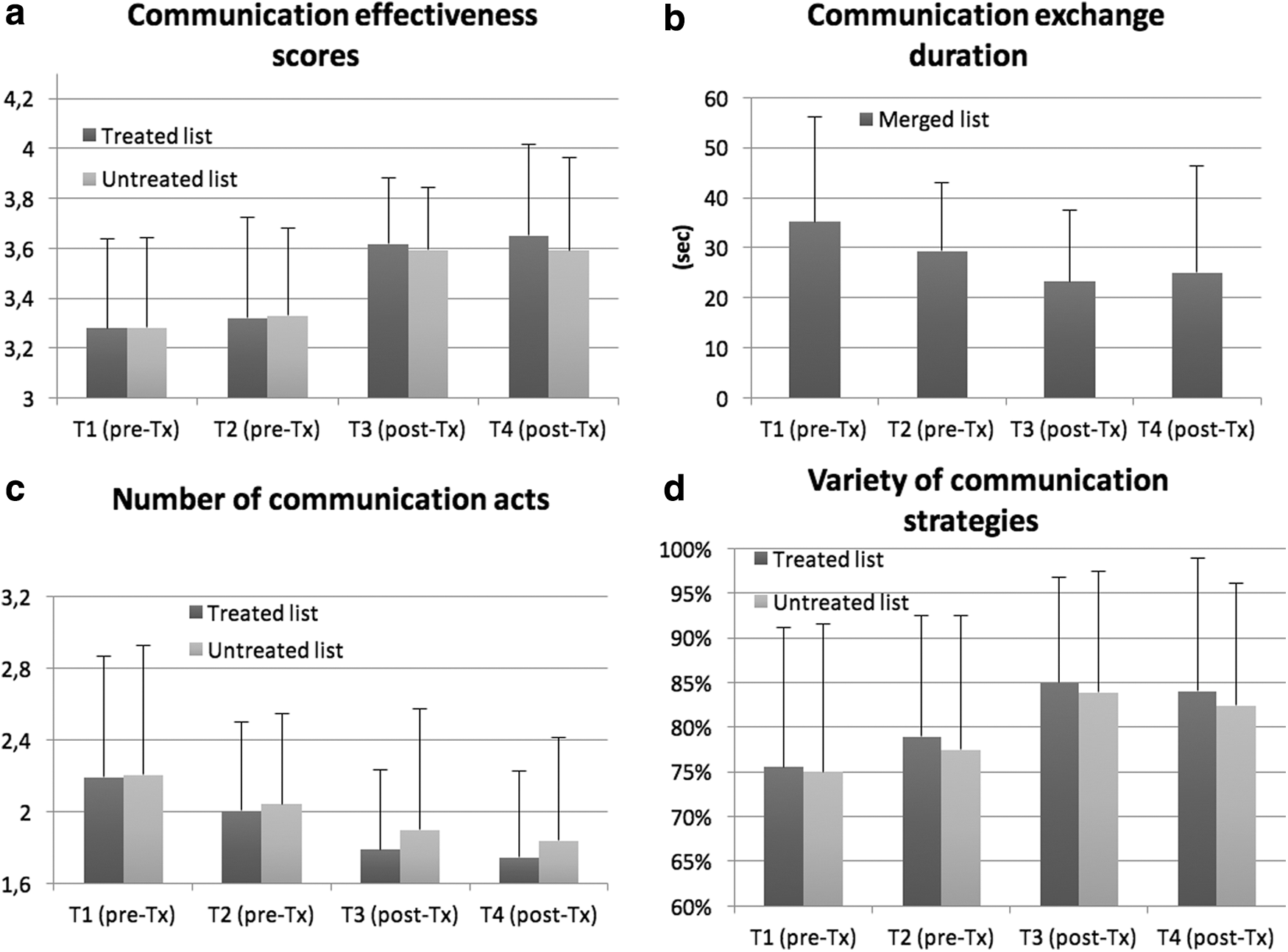
Pre-/post-treatment outcome measures: Communication effectiveness scores
Regarding the average communication exchange duration (Fig. 2b), statistical analyses show a generally significant effect of treatment, with a decrease in duration after treatment: F(1.20) = 15.24, p = 0.0009. This result indicates that the reduction in exchange duration (improvement in communication speed) was treatment specific. On the individual level, all participants except one (C01) followed the group trend (95%). We should note that the testing procedure did not allow us to measure average exchange duration independently for the treated and untreated lists.
Regarding the average number of communication acts (Fig. 2c), statistical analyses indicate a generally significant effect of treatment, with a decrease in number after treatment: F(1.20) = 16.60, p = 0.0006. No significant list (p = 0.20) or list × treatment interaction (p = 0.17) effects were found. These results indicate that the reduction in the number of communication acts (less information needed to be efficiently understood) was treatment specific, and its outcome was generalized to untreated material. On the individual level, all participants except two (C06 and C07) followed the group trend (90%).
The last variable reported in Figure 2d is the variety of communication strategies used. Statistical analyses indicate a generally significant effect of treatment, with an improvement in strategy diversity after treatment: F(1.20) = 15.93, p = 0.0007. No significant list (p = 0.12) or list × treatment interaction (p = 0.88) effects were found. These results indicate that the increase in the variety of communication strategies used was treatment specific, and its outcome was generalized to untreated material. On the individual level, 15/20 participants (75%) followed the group trend. Individual participant data of pre-/post-treatment outcome measures are presented in Appendix Table A1.
Within Treatment
Analyses were also conducted on the data collected throughout the nine treatment sessions (S1–S9). The same four variables were collected automatically by the Oralys TeleTherapy software at the end of each session. Owing to occasional technical failures with the software and/or server, outcome data for 29 of the 180 sessions (16%) are missing. These missing data were randomly distributed.
Figure 3a displays the average communication effectiveness score over each treatment session. Statistical analyses indicate a generally significant effect of treatment on communication effectiveness: F(8, 13.88) = 6.70, p = 0.0009. Post hoc analyses indicate that this significant increase occurred between the second (S2) and third treatments (S3).
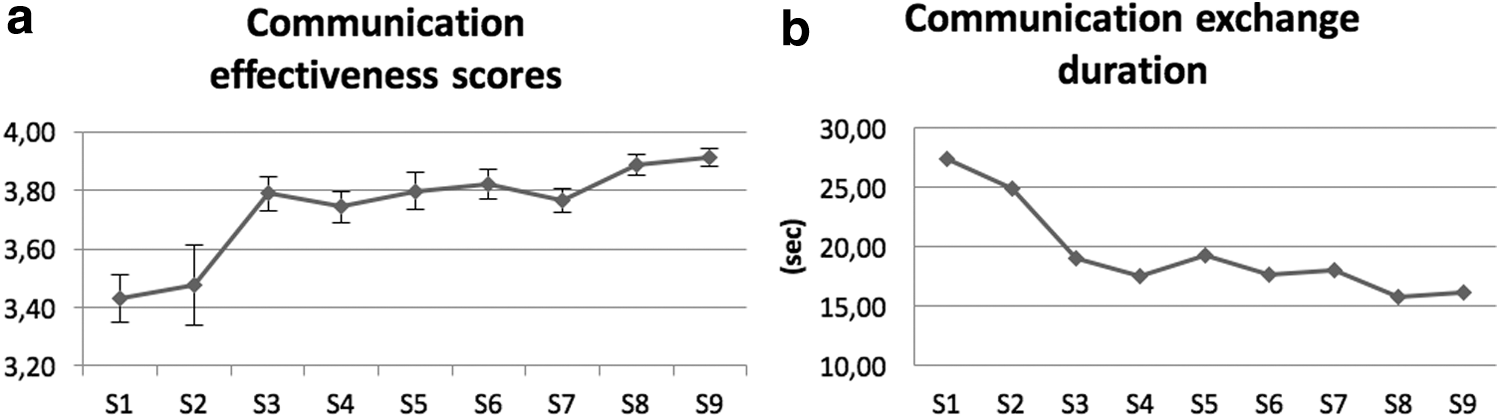
Communication effectiveness scores
Figure 3b displays the average communication exchange duration over each treatment session. Statistical analyses indicate a generally significant effect of treatment on exchange duration: F(8, 17.45) = 14.36, p = 0.000003. Post hoc analyses indicate that this significant decrease in duration also occurred between the second (S2) and third treatments (S3).
The same analyses were conducted for the number of communication acts and the variety of communication strategies used. These additional analyses, however, did not show a consistent pattern of change over the sessions and were not statistically significant (p > 0.01).
Control Task
Analyses were also conducted on verbal fluency task performance pre- and post-treatment, which served as a control task in which no change was hypothesized. Overall, no statistical difference was observed in the free [t(19) = 1.19, p > 0.01], in the orthographic [t(19) = 0.93, p > 0.01], or in the semantic [t(19) = 1.52, p > 0.01] condition.
Discussion and Conclusions
In this study, the therapeutic effect of a pragmatic treatment, remotely delivered through videoconferencing, was assessed in 20 participants with chronic aphasia. This treatment resulted in an improvement in functional communication effectiveness. More specifically, the adapted procedure based on the PACE approach 20 used in this study led to (a) an increase in communication effectiveness, reflecting significantly improved autonomy in functional communication; (b) a decrease in communication exchange duration, meaning that the treatment made communication faster and more efficient; (c) a decrease in the number of communication acts, meaning that, after treatment, less information was needed to be efficiently understood; and (d) an increase in the number of different communication strategies used, meaning that the treatment fostered the use of a variety of alternative communication modes. This improvement cannot be attributed to repeated exposure to the stimuli and repeated communication attempts because no improvement occurred on the verbal fluency control task.
Improvement was also observed on the untreated list of stimuli, supporting the contention that the effects of PACE are not item specific but rather “communication specific.” Indeed, this treatment method is known to entail general improvement in functional communication through clinical activities comparable with daily communication activities. 14,15 This study is the first to show that the PACE approach is also suitable for telespeech therapy, provided that the interaction is face-to-face and that various communication strategies can be used. However, a limitation of this study was the lack of an explicit measure of generalization of the gains of therapy to communication in daily life. This limitation is frequently reported in studies on language therapy in aphasia, and future studies should investigate the effects of telespeech therapy on language in people's daily and domestic living activities.
The use of telespeech therapy for the treatment of poststroke aphasia was explored in recent years. In a few studies, an asynchronous type of telespeech therapy system was used successfully. 23,24 For example, in a recent study involving eight patients with chronic poststroke aphasia, Choi et al. showed that 4 weeks of telespeech therapy, implemented in a mobile application and asynchronously delivered on a smart tablet, had positive effects on various language domains. Telespeech therapy has also proven efficient in a few studies with individuals with aphasia in their home environment using a videoconferencing system. Recently, we successfully used such a system to remotely deliver language treatment to three individuals with chronic aphasia. 8 Furnas and Edmonds 25 administered the computerized version of the Verb Network Strengthening Treatment (VNeST) 26 through telespeech therapy over the Internet. VNeST, a treatment designed to improve lexical retrieval, was administered three times per week for 8 weeks in two individuals with chronic aphasia in a single-subject, experimental design. After treatment, both participants showed improvement on lexical retrieval during spoken and typed production of trained stimuli, and generalization to untrained words was also observed. Using two commercial platforms for online meetings (WebEx and GoToMeeting) with nine individuals with chronic aphasia, Steele et al. 27 explored the feasibility and effectiveness of a treatment, combining individual (3 h) and group (21 h) sessions remotely delivered as well as independent online therapy. The authors showed that the method was sustainable, beneficial, engaging, and attractive to participants. They also showed modest changes in mean scores on the Western Aphasia Battery—Revised, 28 whereas functional communication 29 improved significantly.
Researchers also compared conventional face-to-face therapy and telespeech therapy in poststroke aphasia. Fridler et al. compared the effects of telespeech therapy (14-session block) at home with the effects of conventional face-to-face (14-session block) therapy for naming in eight patients with aphasia. 30 They reported similar improvements in all participants on most outcome measures, regardless of therapy method, as well as greater improvement after telespeech therapy for the aphasia quotient score on the Western Aphasia Battery. 31 Recently, Agostini et al. explored the effectiveness and feasibility of telespeech therapy compared with a conventional face-to-face treatment of naming. 32 Five individuals with chronic poststroke aphasia were treated in-person on a word list and through Skype on another list using a phonemic cueing paradigm. The authors showed that both treatment methods yielded comparable positive results on naming performance. In a study conducted with two individuals with poststroke aphasia trained on personally relevant dialogue scripts, Goldberg et al. showed improvements in speech accuracy, grammatical productivity, speaking rate, and articulatory fluency after a treatment combining in-person meetings and videoconferencing. 33
This study provides additional arguments by showing that multimodal language therapy delivered through synchronous telespeech therapy had positive effects on functional communication in chronic aphasia. This result is of particular importance because there are few speech–language therapy services available to persons with chronic aphasia, at least in Quebec and Canada. In this context, it is essential to develop new service provision alternatives, without burdening scarce professional resources. Telespeech therapy is a promising approach in this respect because it has the potential to increase the frequency and intensity of treatment, which is a key determinant of success, as pointed out by Bhogal et al. 34
Telespeech therapy also alleviates the problem of the remoteness of healthcare facilities as well as the impact of mobility problems that often accompany poststroke aphasia. For optimal use of synchronous telespeech therapy, however, certain conditions must be met, such as technical requirements (high-speed Internet connection, webcam, videoconferencing system, etc.), support of information technology professionals, and assistance of a caregiver or family member. Research on the feasibility and effectiveness of telespeech therapy for the treatment of language impairments associated with poststroke aphasia is at a very early stage. Further studies are needed to determine the criteria for using a particular method or treatment approach according to the nature and severity of language impairments. Other clinical studies should also be conducted to determine the optimal intensity and frequency of telespeech therapy, the best time to begin teletreatments after or in combination with face-to-face rehabilitation, and the best candidates for telespeech therapy. The results of this study provide some answers to these questions by showing that telespeech therapy explicitly focusing on multimodal functional communication appears to be suitable and effective for individuals with various aphasia profiles.
Footnotes
Acknowledgment
This work was funded by the Canadian Institutes of Health Research (Grant No. MOP-102748).
Disclosure Statement
No competing financial interests exist.
Appendix
Individual Participant Data of Pre-/Post-Treatment Outcome Measures
| COMMUNICATION EFFECTIVENESS SCORES (/4, SEE TABLE 1) | COMMUNICATION EXCHANGE DURATION (S) | NUMBER OF COMMUNICATION ACTS | STATEGY DIVERSITY USAGE | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PRE-TREATMENT | POST-TREATMENT | PRE-TREATMENT | POST-TREATMENT | PRE-TREATMENT | POST-TREATMENT | |||||||||
| ID | TREATED LIST | UNTREATED LIST | TREATED LIST | UNTREATED LIST | PRE-TREATMENT | POST-TREATMENT | TREATED LIST | UNTREATED LIST | TREATED LIST | UNTREATED LIST | TREATED LIST | UNTREATED LIST | TREATED LIST | UNTREATED LIST |
| C01 | 3.56 | 3.60 | 3.92 | 3.85 | 53.5 | 66.5 | 3.60 | 3.79 | 2.77 | 3.76 | 0.541 | 0.527 | 0.595 | 0.481 |
| C02 | 3.19 | 3.22 | 3.43 | 3.34 | 74.5 | 58.0 | 2.33 | 2.56 | 2.02 | 2.13 | 0.749 | 0.742 | 0.816 | 0.825 |
| C03 | 3.35 | 3.34 | 3.96 | 3.82 | 51.0 | 41.0 | 2.86 | 2.61 | 2.46 | 2.46 | 0.717 | 0.776 | 0.710 | 0.756 |
| C04 | 3.85 | 3.84 | 3.99 | 3.94 | 37.5 | 26.5 | 3.02 | 3.03 | 1.99 | 2.80 | 0.617 | 0.557 | 0.751 | 0.711 |
| C05 | 3.13 | 3.15 | 3.33 | 3.29 | 53.5 | 49.0 | 2.56 | 2.59 | 2.36 | 2.14 | 0.694 | 0.617 | 0.679 | 0.762 |
| C06 | 2.55 | 2.64 | 2.62 | 2.58 | 45.0 | 39.0 | 2.06 | 2.27 | 2.45 | 2.16 | 0.605 | 0.548 | 0.560 | 0.609 |
| C07 | 3.35 | 3.36 | 3.54 | 3.35 | 16.5 | 12.5 | 1.56 | 1.63 | 1.79 | 2.07 | 0.872 | 0.930 | 0.842 | 0.786 |
| C08 | 3.56 | 3.52 | 3.62 | 3.52 | 28.0 | 16.0 | 1.71 | 1.67 | 1.56 | 1.61 | 0.796 | 0.778 | 0.836 | 0.757 |
| C09 | 3.62 | 3.60 | 3.94 | 3.85 | 16.0 | 10.0 | 1.82 | 1.76 | 1.39 | 1.54 | 0.908 | 0.938 | 0.939 | 0.919 |
| C10 | 3.47 | 3.49 | 3.53 | 3.56 | 24.0 | 18.5 | 1.66 | 1.68 | 1.53 | 1.44 | 0.827 | 0.799 | 0.866 | 0.885 |
| C11 | 3.13 | 3.17 | 3.64 | 3.57 | 15.5 | 10.0 | 2.31 | 2.33 | 1.59 | 1.79 | 0.809 | 0.815 | 0.987 | 0.904 |
| C12 | 2.80 | 2.79 | 3.69 | 3.73 | 27.0 | 17.0 | 2.37 | 2.33 | 1.80 | 1.53 | 0.592 | 0.618 | 0.842 | 0.859 |
| C13 | 3.40 | 3.42 | 3.67 | 3.59 | 14.5 | 9.0 | 1.67 | 1.65 | 1.53 | 1.65 | 0.991 | 0.955 | 0.938 | 0.937 |
| C14 | 3.27 | 3.24 | 3.71 | 3.64 | 20.5 | 13.5 | 1.89 | 1.90 | 1.83 | 1.97 | 0.763 | 0.745 | 0.868 | 0.835 |
| C15 | 3.13 | 3.16 | 3.82 | 3.82 | 19.5 | 6.0 | 2.09 | 2.13 | 1.29 | 1.36 | 0.617 | 0.575 | 0.868 | 0.864 |
| C16 | 3.24 | 3.23 | 3.64 | 3.67 | 43.5 | 26.5 | 2.00 | 2.10 | 1.44 | 1.37 | 0.789 | 0.791 | 0.903 | 0.882 |
| C17 | 3.67 | 3.67 | 3.58 | 3.63 | 23.5 | 16.0 | 2.09 | 2.17 | 1.56 | 1.53 | 0.732 | 0.710 | 0.931 | 0.894 |
| C18 | 3.59 | 3.53 | 3.80 | 3.80 | 31.0 | 20.0 | 1.56 | 1.52 | 1.39 | 1.33 | 0.871 | 0.865 | 1.000 | 1.000 |
| C19 | 3.50 | 3.51 | 3.84 | 3.77 | 18.0 | 11.0 | 1.52 | 1.46 | 1.38 | 1.39 | 0.961 | 0.959 | 0.992 | 0.964 |
| C20 | 2.66 | 2.64 | 3.44 | 3.56 | 32.5 | 16.5 | 1.36 | 1.34 | 1.25 | 1.37 | 1.000 | 1.000 | 0.976 | 1.000 |