
Abstract
Background:
Telemedicine systems are gaining attention nationwide as a means for providing care in remote areas and allowing a small number of providers to impact a large geographic region. We systematically reviewed the literature to identify the efficacy and implementation challenges of telemedicine systems in ambulances.
Methods:
A search for published studies on Web of Science and PubMed was completed. Studies were selected if they included at least a pilot study and they focused on feasibility or implementation of telemedicine systems in ambulances.
Results:
A total of 864 articles were used for title and abstract screening. Full text screening was completed for 102 articles, with 23 being selected for final review. Sixty-one percent of the studies included in the review focused on general emergency care, while 26% focused on stroke care and 13% focused on myocardial infarction care. The reviewed studies found that telemedicine is feasible and effective in decreasing treatment times, report a high diagnosis accuracy rate, show higher rates of positive task completion than in regular ambulances, and demonstrate that stroke evaluation is completed with comparable accuracy to the standard way of delivering care.
Conclusions:
Although this review identified life-saving benefits of telemedicine, it also showed the paucity of the scientifically sound research in its implementation, prompting further studies. Further research is needed to analyze the capabilities and challenges involved in implementing telemedicine in ambulances, especially studies focusing on human-system integration and human factors' considerations in the implementation of telemedicine systems in ambulances, the development of advanced Internet connectivity paradigms, additional applications for triaging, and the implications of ambulance location.
Introduction
Telemedicine, the use of telecommunications technology to provide access to healthcare when geographical barriers make face-to-face consultation impractical, 1 –3 is being integrated into such wide-ranging aspects of patient care as home health monitoring, 4 out-of-office hospital consultation, 5 and ambulances. 6 This growing field began in the 1960s when telephone communications and microwave signals were first introduced for transporting data, 7 followed by the second generation in the 1990s with the creation of the Internet and the World Wide Web, both of which relaxed the constraints of time and geography. 8 The third and current generation focuses on the use of mobile networks to transfer data, including video and voice communication, across vast distances. 9 Feasibility, pilot, and clinical studies using this third generation have explored both the benefits and limitations of this growing field, 6,9 –26 finding that these systems require low interference and a high level of functionality and usability to facilitate seamless interaction.
Emergency care, specifically that given in ambulances, is one area where telemedicine has the potential to play a critical role. Past research, 6,9,11,12,19,24,27 found that its use can decrease treatment time by completing diagnosis steps in pre-hospital transport with a high level of diagnosis accuracy. For example, several studies 18,19,25,28 have found that stroke evaluation completed by teleconsultation in conjunction with Emergency Medical Services (EMS) personnel can improve the level of care given before admittance to the hospital; this is especially important because according to a recent review, 29 74% of stroke cases died outside of the hospital. 30 Given that 99.1% of hospitals in the U.S. alone have a recombinant tissue plasminogen activator (rt-PA) treatment rate of 10% or less, 31 in most instances caused by the time to treatment being longer than the 3-h window from symptom onset, 6,24 reducing transport time using telemedicine holds a large potential for increasing stroke survival rate. 32 Integrating telemedicine systems in ambulances may reduce fatalities from not only strokes, but also other cardiovascular diseases. Given the importance of this area of research on healthcare worldwide, this systematic review focuses on the lifesaving benefits that telemedicine in ambulances can provide by identifying how it is implemented and exploring the efficacy of this implementation. Furthermore, it summarizes the results from the research reviewed and identifies the challenges, best practices, and opportunities for further research.
Materials and Methods
Institutional Review and Human Subject Determination
This study was exempted from approval by Clemson University's Institutional Review Board, as it did not involve active human subject research. No individual patient participated in this study.
Data Sources
We searched Web of Science and PubMed for articles published between the years 2000 and 2016. Duplicates were identified using Endnote and searching manually. An additional search was made through citations of articles selected for review for relevant studies published within the same time frame, but none were found to be useful for review.
Search Terms
We searched the databases using keywords “Telemedicine AND Ambulance” (retrieved 134 articles from PubMed; retrieved 140 articles from Web of Science), “Telemedicine AND emergency healthcare” (retrieved 8 articles from PubMed; retrieved 14 articles from Web of Science), “Emergency Telemedicine” (retrieved 57 articles from PubMed; retrieved 55 articles from Web of Science), and “Telemedicine AND Emergency Medical Services” (retrieved 396 articles from PubMed; retrieved 72 articles from Web of Science), and selected titles and abstracts that incorporated telemedicine systems into ambulances, testing the system's feasibility in any patient category.
Inclusion and Exclusion Criteria
Domain
Articles were included from any domain as long as they focused on the implementation of telemedicine systems in ambulances.
Article format
Extended abstracts and posters were not included in this review, and studies were excluded if they did not contain at least a pilot study with simulated or real patients.
Language
Only articles published in English were included in this review.
Publication year
Articles were only chosen if they were published between 2000 and 2016. This time-period was chosen not only to keep studies relevant but also to document the beginning and development of the third generation of telemedicine, which is defined by the revolution of communication over mobile networks.
Article Selection
Four of the authors (H.R., S.A., S.N., and A.A.) reviewed titles and abstracts of all articles found in initial search (864) to determine which could be included for full-text screening. Abstracts were not considered for full text review if they did not include any experimental results. With this screening process, 102 articles were chosen for full text analysis, which was completed by at least one of two authors (H.R. and S.A.). Articles were excluded if they did not test telemedicine system capabilities in some way to show feasibility or implementation benefits and challenges. As a result, 23 studies were selected for review; any conflicts in selection decisions were resolved through discussion between readers. Figure 1 describes the article search, screening, and selection in more detail.
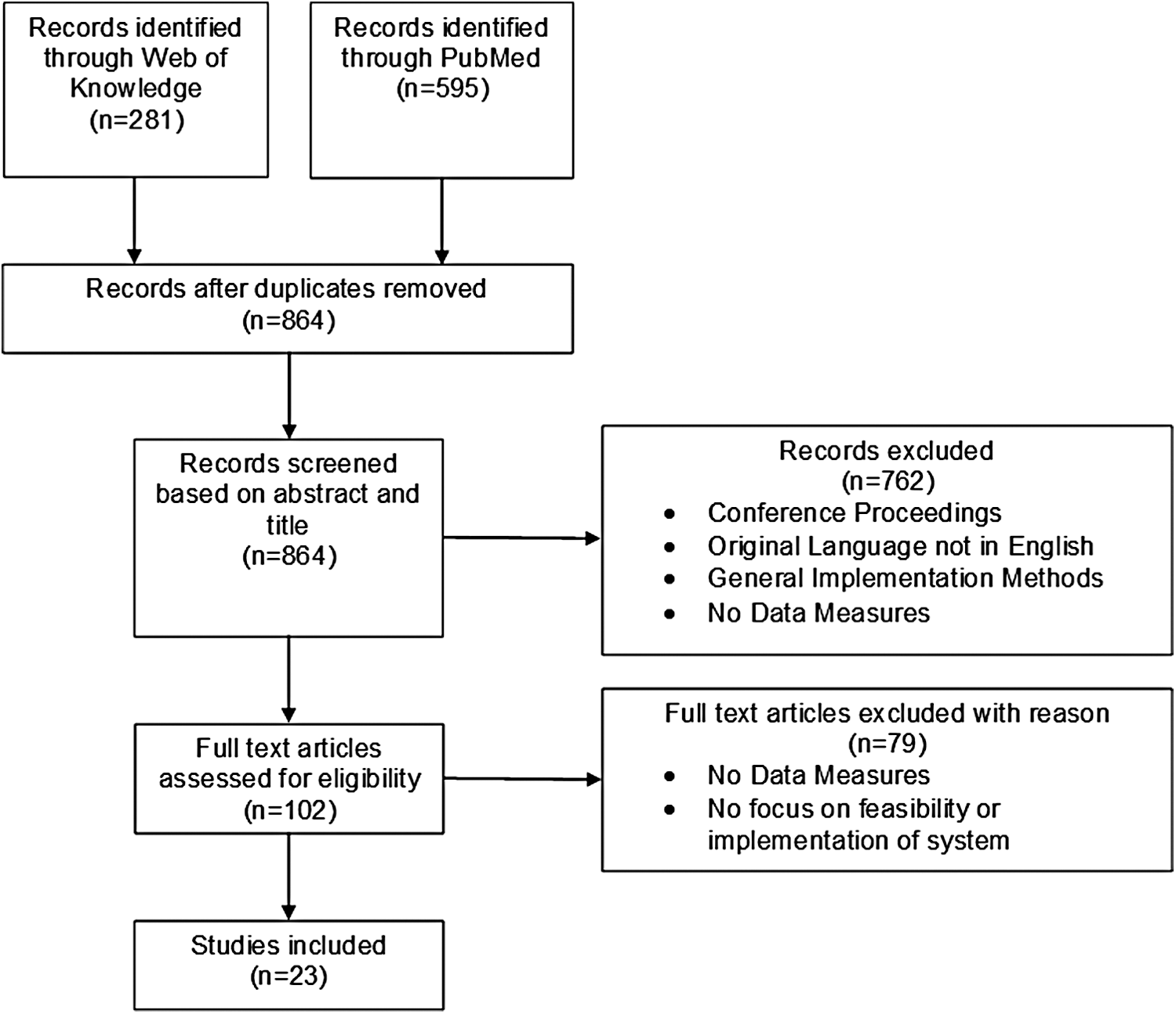
Selection flowchart.
Data Abstraction
Data were taken from each article and placed into a table to organize results and details about each article. Two authors (H.R. and S.A.) identified method, sample size, objectives, technology, application, key findings, and limitations.
Results
Analysis of these 23 studies suggested three major domains of research: General Care, Stroke Care, and STEMI Care, with each study including the application, the technology explored, the data collection methods used, and an analysis of the data collected and the results found.
Application Overview
An analysis of the 23 articles found they represented three application categories. Most studies (61%) involved general emergency care, with the remaining 39% focusing on one type of emergency patient. More specifically, six studies focused on stroke pre-hospital care and three on ST Elevation Myocardial Infarction (STEMI) care. Table 1 categorizes the studies based on application domain.
Application Domain
Origin Overview
Thirty-five percent of studies were conducted in the United States, another 30% were conducted in Germany, and the remaining countries of origin have no more than two studies. Specifically, two studies were conducted in each of the following countries: Greece, South Korea, and Belgium, and one study was conducted in each of the following countries: Japan and Denmark.
Technology
The technology used most frequently in the studies reviewed was for the transmission of vitals or testing results over a network, a use case seen in all, but six, of the studies. 9 –11,13,15 –17,19 –24,26 –28,33,34 Such vital signs as blood pressure, blood sugar, body temperature, and electrocardiogram (ECG) were transmitted over various network types, with six studies using a GSM, 10 –12,17,20,23 nine using 4G LTE/3G networks, 6,9,13,16,20,22,24 –26 and two using a High-Speed Downlink Packet Access (HSDPA) technology. 18,21 The remaining studies either used radio links, 27,34 Wireless Broadband Internet, 14,15 or did not specify the network. 19,28,33 In addition to the transmission of vital data, all but 2 (9%) used some form of communication from the ambulances to either a hospital or an out-of-office location. 12,33 Sixty-seven percent of the studies used a cell phone system with a video feed or still pictures for communication with the hospital unit, 6,10,11,13,14,16,17,19,20,22,23,27,28,34 while the remaining 33% used a bidirectional video and audio system. 9,15,18,21,24 –26 Table 2 shows the technologies and networks used in each study.
Technology and Network
HSDPA, High Speed Downlink Packet Access.
Data Collection and Analysis Methods
Of the studies reviewed, 61% included some form of user evaluation 9 –11,13 –15,17,18,20,21,23,25,26,34 to collect the data from the participants. This evaluation focused on usability of the telemedicine system, 9,10,13,14,25 the clinical value of the telemedicine equipment and its results, 14,23 the acceptance rate of the telemedicine system, 9,34 and/or the technical quality of the telemedicine transmissions. 11,15,17,18,20,21,23,26 In addition, network signal strength and data transfer speeds were used for data collection, with 4 of the 23 studies using this evaluation method. 9,10,20,24 Another two studies focused on comparing the tasks completed in a regular ambulance to those completed in a telemedicine-equipped ambulance. 16,28 Stroke care studies reviewed involved evaluating the possibility and reliability of stroke assessment 6,18,19,25 and measured the time to evaluate a patient with National Institutes of Health Stroke Scale (NIHSS) to validate the system's feasibility. 25,26 Time to treatment was a method used largely in Stroke and STEMI care studies, 6,11,19,22,27 with one general care study using this method. 12 Furthermore, diagnosis accuracy, the comparison of pre-hospital and final diagnosis, was used in three studies, 9,11,24 while one study used a heuristic methodology to evaluate a telemedicine system, with evaluators and EMS users analyzing the prototype iterations based on their usability characteristics. 33
Reported Results
The system user evaluations varied, with four studies measuring system usability 9,10,13,14 and five measuring the technical quality of the system. 15,17,20,21,23 A study measuring usability through a survey of users, asking them to rate their level of agreement with certain statements found high agreement with the statements, “the telemedicine system was easy to operate,” “the telemedicine system was easy to learn,” and “delays in sending videos posed few problems.” 10 Another study found that a new system has low usability and maintenance ratings, but had high clinical value. 14
In two studies, the quality of still images was rated as excellent to good in 73% 17 and 93% 23 of cases and video streaming was rated as excellent to good in 89% 17 and 92% 23 of the cases. Acceptance of the telemedicine system was assessed in two studies through user evaluation, with one study concluding high acceptance based on a 0% patient refusal rate. 34 In addition, three studies 9,14,23 measured the clinical value of telemedicine with the clinical value of pictures and video rated very helpful and helpful in routine use by 94% and 87% of the users, respectively, in one study. 23
Because of the limitations in bandwidth and signal at various locations, the user evaluation of the audio and/or visual quality of transmissions varied, with three studies 9,10,20 measuring signal strength and speed. One study determined median upload and download speeds of out-of-office hours at ∼200 kilobits per second (kbps) and 100 kbps and of in-office hours at ∼750 and 75 kbps with a transmission success rate of 73.2%. 9
Comparing traditional ambulance care to telemedicine ambulance care and survival rates, the studies reviewed here found that not only did emergency medical technicians (EMTs) in the latter complete more positive tasks in a simulation study but were also able to complete procedures, for which they had no previous training, successfully with the instruction of doctors through telemedicine using simulated patients; in addition, the telemedicine-equipped ambulance had a higher survival rate. 16,28 Pre-hospital diagnosis and final diagnosis agreement rates in studies comparing the two were high, with a K statistic of 0.98 and 0.92 for neurological and nonneurological disease, respectively, and 100% for stroke cases using the ambulance. 9
Heuristic evaluation decreased usability and heuristic violations by 42% and 50%, respectively, after one round of evaluation in one study. However, heuristic evaluation did not find all issues in the system during the four iterations of the design tested. An ethnographic test in this study revealed 48 usability problems, 21 being potentially catastrophic, with 6 of these 21 being verified in the heuristic evaluation. 33
For the NIHSS evaluation, agreement rates were measured by comparing different trained evaluator's ratings of a patient completed through teleconsultation and/or by comparing standard training video ratings, or in ambulance ratings to telemedicine system ratings; both of these studies revealed similar results. 6,18 In a study with three raters, the overall interrater reliability K statistic in the 12 scenarios tested were 0.78 in the telestroke group and 0.69 in the control. 18 In a different study evaluating the success rate in telemedicine NIHSS evaluations, the assessments were successfully completed in 10 of 11 real patient cases and 5 of 5 simulated patients, with the mean time taken to complete the assessment being 7.6 min. 25
When evaluating time to treatment in stroke application, one study found the mean time to be 33 min in the control group and 17 min in the telemedicine group. 6 The results from STEMI studies vary in the improvement in door-to-balloon time, but one study 11 found the mean door-to-needle time was 38 min faster than the control group. This study also found a mean transport time that was faster in the telemedicine group by 8 to 12 min depending on if a diagnosis was attempted (Table 3).
Key Findings
EMT, emergency medical technician; NIHSS, National Institutes of Health Stroke Scale.
Discussion
This review was executed to understand the current state of research and detail benefits and challenges faced in studies implementing or testing telemedicine systems in ambulances. Limitations of these studies were documented and are discussed in this section to gain insight on what further study needs to be completed to eliminate these limitations.
Growing concerns in healthcare information technology include the feasibility of using technology to assist in patient care, 35,36 especially in emergency situations. Of particular interest is how to ensure that this technology works seamlessly with healthcare professionals to limit interference with patient care. 1,37 Usability testing and user evaluations were represented as a methodology used in more than half of the studies reviewed in this article, with one study devoted entirely to heuristic evaluation and ethnography 33 ; however, four studies reported low usability 13,14,23 or low transmission quality, 13,18 and one study concluded that the transportation of the telemedicine unit was not feasible in situations where transport on scene to treat a patient outside of the ambulance was needed given the size and weight of the unit. 21 Given the importance of implementing a highly functional system in a time-dependent process, stakeholders such as EMTs, patients, and doctors should be at the heart of the design process. The timing, efficiency, and level of care are paramount in EMS, and design of the telemedicine systems has to be designed with them in mind to be integrated successfully.
One concern in human-centered design is the cognitive and physical stressors put on the stakeholders by the system. 38,39,40,41 Research developing possible stressors, how they affect work in ambulances and with a teleconsultant, and how to eliminate these stressors is needed specifically with telemedicine to be a viable tool for use in ambulances. Another consideration in design is the patient's level of perceived privacy, which has been addressed in one study included in this review. The study cited that patients did not feel that telecommunications intruded on their privacy and felt comfortable in the use of the system, but more studies should include an emphasis on this viewpoint in the patient experience. 10 Another aspect needed to be considered to create effective care when using telemedicine systems is designing those systems in an integrated environment. 38,40,42 This method limits training needed to effectively use the system and reduces probability of errors given that the system is similar to other technologies and systems in the environment that users are familiar with. 40
Simulated Studies
Six of the 23 articles reviewed used a simulation study as their sole method of system testing, 6,13,16,18,26,28 a situation that limited the procedures tested because they used medical dummies. For example, the study evaluating the feasibility of completing ultrasounds and intubation procedures in an ambulance through teleconsultation, used a medical dummy to test intubation with a video laryngoscopy and 1 patient to test the ultrasound process, simplifying the investigation to a still, nonresponsive patient or a healthy participant. 13 A second study used an METI Human Patient Simulator; however, it simulated patient responses using only a limited number of noninvasive procedures to test the system, thus limiting the testing capacity of the study. 16
Another 9% of the studies used actors to simulate patients, specifically in the NIHSS evaluation. One study generated 12 scenario scripts that actors and clinical care transport staff completed, while three evaluators observed either by TV/VCR recording or through a TeleBAT system on a desktop computer, comparing the results to historic patients, 6 while another study used actors trained in simulating right and left middle cerebral artery stroke syndromes with differing severity. 18 These studies may introduce a bias in the simple NIHSS evaluation because of the previous experience of the actors in simulating strokes as well as limitations in evaluating clinical value of vital transmission as these studies used healthy patients. Two studies reviewed completed an onboard trial with a simulated patient to test the feasibility of the system and orient the medical staff with the equipment before a live trial to both test system capabilities in real situations and validate the feasibility results. 10,25
Sample Size and System Testing
A common limitation cited in the studies reviewed was the sample size of the patient trials or simulation runs. Studies cited small sample sizes as they tested the system, using 4 to 12 participants. Similarly, the sample sizes of simulation tests were also small (n = 7) as were simulation scenarios which ranged from a sample size of 3 to 12; however, the number of runs of these scenarios ranged from 24 to 30. Four of the eight studies citing small sample sizes were feasibility or pilot studies, although further studies with larger sample sizes have been conducted in other studies included in this review. Limitations in system use were cited in 4 of the 23 studies reviewed; however, this issue was of particular importance in simulated patient studies. Two such studies only tested specific functions of a system 6,13 rather than running tests in the field. An additional four studies investigated system functionality using simulated patients. 16,18,26,28 Field test studies addressed this limitation by running tests for long periods of time with no dispatch routing rules and large sample sizes of patients, thus requiring a range of system functions to be used.
Bandwidth and Connection Limitations
A common challenge discussed in these studies was the technical issues faced when using public networks. More specifically, 13 studies, which cited this technical challenge or limitation, used this method because of its widespread application and cost. However, this method created a trade-off in data transfer size and speed. In addition, using public networks in rural areas resulted in signal loss. In one study, the system addressed this issue by allowing users to select the frame rate or picture quality for the telemedicine transmissions. 13
EMT Considerations
Interactions among the stakeholders, including patient and EMT personnel, patient and doctor (in a remote facility), and EMT and doctor (remote facility), should be considered when designing a telemedicine-mediated healthcare environment. When designing telemedicine systems, from a human-system integration perspective, consideration should be given for the current tasks completed by EMTs and doctors in a technology-mediated environment. Integrating technology such as a telemedicine-mediated environment into an ambulance setting can change the job requirements of EMTs and could change the methods that have proven to be successful for maintaining their situation awareness. It could create more work because now the telemedicine equipment, as well as the system itself, must be monitored.
In this development of communication systems, EMTs can do much more than just stabilize a patient; they could begin testing, create a tentative diagnosis, or even administer treatment, if authorized. This situation is tested in studies in this review, specifically those measuring diagnosis accuracy. 9,11,24 Additional studies mentioned a pre-hospital diagnosis being performed, but did not measure the accuracy of those diagnoses to the final hospital diagnosis. 17,23 In these studies measuring diagnosis accuracy, the accuracy was found to be high, reflecting clinical value of EMTs diagnosing patients in ambulance or on the scene not just for simplicity of treatment post-transport, but also because this ability to diagnose pre-hospitally could shorten transport time and treatment time.
Financial Implications
Thirteen studies mentioned the limitations of using public networks for cost-effectiveness and common, inexpensive materials to outfit ambulances as teleambulances when available; however, the cost of this initiative remains a concern. One study identified in the literature screening process for this review investigated the cost of using telemedicine to increase the use of rt-PA treatments in eligible patients. The study also evaluated the benefit to cost ratio of the system using different configurations of personnel at varying operating distances, and even the highest cost configuration of personnel achieved a benefit ratio greater than 1 at an operating distance of 20 km. 43
Another study investigated the benefit to cost comparison of congenital heart disease patients using an ambulance equipped with an ECG, a camera, an iPod touch and a laptop connected to a central server. The results of this study found cost savings between 33,586 € and 35,740 € within 1 year. 44 While these studies only represent care for a specific condition rather than general care, they show that it is feasible and cost-effective to implement a telemedicine system. Future study could include the possibility of using private networks with higher bandwidth capabilities and a cost analysis of applying a telemedicine system for general emergency care.
Limitations
This review has limitations. Only peer-reviewed journal articles written in English were included in this review. Defining the search keywords was difficult, and it was learned that not all studies that should have been identified were found in the search.
Future Research Questions
This review suggests a paucity of published studies describing scientifically valid and reproducible evaluations at various stages of telemedicine implementation in ambulances. The common limitations and unique testing challenges found in the studies reviewed here led to the formulation of several recommendations for future studies or for generating a focus for a study to further test the feasibility of telemedicine systems in improving patient care.
A system of systems includes a collection of different systems, originally designed for a specific purpose, are combined and/or coordinated to produce a very large system. Inherently, such a system poses new challenges. 41,45 A telemedicine-integrated ambulance is an example of a system of systems. Human capabilities and limitations must be considered while implementing such a system. A technology-mediated caregiving environment is operated by a team consisting of EMTs and doctors whose interactions must be taken into account while implementing a telemedicine system in an ambulance. System designers need to ensure that in such a remote caregiving process, considering the operational aspects of just the telemedicine system may not be enough. The key stakeholders involved in this process are required to operate multiple systems, including Electronic Health Records (EHRs) telemedicine systems, adding to the complexity of the caregiving process. Extreme cognitive, physical and temporal demands are placed on the caregivers when operating such a system of systems. Further studies need to be conducted to understand the sensemaking process and situational awareness of caregivers while providing care in such technology-mediated, high stress environment.
Four studies reviewed discussed the impact of developing studies in a variety of areas, as the location determines such variables as response and transport times, signal availability, patient acceptance, and population statistics. One simulation study in this review determined that transportation time in rural areas could be as long as 40 to 50 min, thus creating simulations in which a patient would go critical within 40 min to test the capacity of EMTs to perform lifesaving measures over long transport times. The range of transport times, among other factors, suggests the need for future research exploring the implications in patient care and survival rates of implementing a telemedicine system in an urban area versus a rural area.
One future application of telemedicine that could improve emergency department function would be to use teleconsultation to triage emergency patients. The American College of Surgeons suggests an acceptable percentage of overtriaging is 25% to 35% 46 ; however, even in that range, there is a cost associated with this practice. The Center for Disease Control and Prevention (CDC) cites a study comparing triaging guidelines from 1991 to 2006, identifying a potential $568 million cost savings. 47 Telemedicine may be a useful tool for addressing this situation, if pre-hospital diagnosis could be utilized for triaging patients and preparing the hospital for their arrival. Future research need to validate using remote triaging through teleconsultation to reduce overtriage rates and improve patient transfer.
Conclusion
This article reviewed the literature conducted on telemedicine systems in ambulances for emergency care. According to these studies, the usability ratings of the systems tested are high, and the effects of implementation are significant and positive. However, limitations in usability testing, simulation studies, public network bandwidth, sample size, and cost suggest the need for additional research. Thus future work should focus on enhanced human-system integration, developing a high fidelity, usable system at a low cost and testing this system using live patients suffering from a variety of conditions and injuries to fully explore the use of telemedicine in ambulances. Such research studies could further support the use of telemedicine in ambulances as a viable way to treat emergency patients quickly and efficiently, thus improving the healthcare delivery system for this population.
Footnotes
Acknowledgments
This research was supported by a grant from the South Carolina Telehealth Alliance (
Authors' Contributions
H.R.: Article selection, data extraction, analysis, writing, and editing; K.C.M.: study design, writing, and editing; S.A.: study design, Web search, article screening, article selection, and editing; S.N.: Web search, article screening, and editing; A.A.: study design, writing, and editing; A.N.: study design and editing; B.M.W.: study design and editing; J.T.M: study design and editing.
Disclosure Statement
No competing financial interests exist.