
Abstract
Background:
Atopic dermatitis (AD) is a chronic disease requiring regular follow-up. To increase access to dermatological care, online management of AD is being studied. However, a critical knowledge gap exists in determining AD patients' quality of life in direct-to-patient online models. In this study, we examined quality of life in AD patients managed through a direct-access online model.
Materials and Methods:
We randomized 156 patients to receiving care through a direct-access online platform or in person. Patients were seen for six visits over 12 months. At each visit, the patients completed Dermatology Life Quality Index/Children's Dermatology Life Quality Index (DLQI/CDLQI), and Short Form (SF-12).
Results:
Between baseline and 12 months, the mean (standard deviation, SD) within-group difference in DLQI score in the online group was 4.1 (±2.3); for the in-person group, the within-group difference was 4.8 (±2.7). The mean (SD) within-group difference in CDLQI score in the online group was 4.7 (±2.8); for the in-person group, the within-group difference was 4.9 (±3.1). The mean (SD) within-group difference in physical component score (PCS) and mental component score (MCS) SF-12 scores in the online group was 6.5 (±3.8) and 8.6 (±4.3); for the in-person group, it was 6.8 (±3.2) and 9.1(±3.8), respectively. The difference in the change in DLQI, CDLQI, SF-12 PCS, and SF-12 MCS scores between the two groups was 0.72 (95% confidence interval [90% CI], −0.97 to 2.41), 0.23 (90% CI, −2.21 to 2.67), 0.34 (90% CI, −1.16 to 1.84), and 0.51 (90% CI, −1.11 to 2.13), respectively. All differences were contained within their equivalence margins.
Conclusion:
Adult and pediatric AD patients receiving direct-access online care had equivalent quality of life outcomes as those see in person. The direct-access online model has the potential to increase access to care for patients with chronic skin diseases.
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease characterized by type 2 inflammation, skin-barrier disruption, and marked pruritus. 1 The prevalence of AD has been reported at ∼3% to 10% for adults and 20% for children. 1 The burden of AD has been noted to be significant, as it affects activities of daily living, psychosocial well-being, and overall quality of life. 1 –4 Patients with AD, especially those with moderate-to-severe AD, require regular monitoring and management, but there is a workforce shortage among dermatology providers to adequately care for AD patients in the United States. 5 –8 Consequently, many patients lacking access to care experience poor health outcomes and diminished quality of life. 9
Research has suggested telemedicine as a potential solution for the physician shortage. Teledermatology can serve as a resource to provide care to those who otherwise lack access, particularly when dealing with chronic skin conditions. 10,11 Store-and-forward teledermatology, or asynchronous teledermatology, has not only demonstrated diagnostic reliability and accuracy in previous studies, but it has been shown to be comparable to in-person care. 12,13
The use of store-and-forward teledermatology in the context of a “consultative” model has been practiced in underserved areas. However, the consultative model has several limitations. 14 –16 First, patients must find a primary care physician (PCP) who has access to dermatologists practicing telemedicine. Second, patients must still wait for an available PCP appointment, commute to the PCPs office and wait to be seen once in the office. Because the dermatologist is a consultant, patients are not provided with the opportunity to directly communicate with the dermatologist, which makes it difficult for patients to ask questions about their care. PCPs may find the use of teledermatology consultations to be tedious, and implementing the dermatologist's directives increases their workload without providing adequate fiscal compensation in return. Additionally, the PCP must relay patients' questions to the dermatologist, and the dermatologist might not respond promptly or provide targeted explanations. 17
There is a need for new models of delivering specialty care that are independent of time and distance. Direct-access online care is one such store-and-forward teledermatology model in which patients can directly communicate with dermatologists for management of their skin conditions. 18 –20 AD is visible, pruritic, and socially stigmatizing, and therefore it has a constant impact on quality of life. AD patients can particularly benefit from direct-access online care to receive the follow-up necessary to adequately control their disease, and ultimately improve their quality of life. 21
There is a critical gap in assessing quality of life in dermatology patients, especially those with AD, who utilize teledermatology services. 22 To address this gap, this 1-year randomized, controlled equivalency clinical trial compared quality of life outcomes between AD patients who received follow-up care though an online direct-access model with those who received follow-up care in person. We aimed to assess whether AD patients who receive direct-access online care have comparable quality-of-life outcomes to patients managed in person, as measured by Dermatology Life Quality Index (DLQI), Children's Dermatology Life Quality Index (CDLQI), and the Short Form (SF-12) questionnaire.
Materials and Methods
Study Design
In this randomized controlled equivalency clinical trial, we examined AD disease severity and quality of life in pediatric and adult AD patients who received follow-up online versus in person. This article addresses quality of life outcomes. The duration of patient follow-up was 1 year. This study was approved by the University of California, Davis Institutional Review Board (243201).
Patient Selection
Pediatric and adult patients with AD were recruited from the general greater Sacramento community, dermatology clinic at UC Davis, primary care clinics affiliated with UC Davis, federally qualified health centers, and free clinics providing care to underserved patient populations.
All children and adults had to satisfy the following criteria to be considered for inclusion in the study: (1) were at least 4 years of age; (2) met Hanifin criteria for AD diagnosis; (3) had a digital camera, computer, and Internet access; and (4) were able to photograph their skin on their own or have family members do so.
Patients that did not meet inclusion criteria were excluded, as were patients who (1) necessitated systemic therapy (e.g., phototherapy and cyclosporine); (2) necessitated regular laboratory monitoring; and (3) did not speak Spanish or English.
Study Interventions
At baseline, all participants were examined by a dermatologist via an in-office visit to confirm the diagnosis of AD. Additionally, all adult subjects completed baseline quality of life assessments using the DLQI and SF-12. CDLQI was completed for pediatric patients.
Participants were randomized 1:1 into 1 of 2 arms of the study: the direct-access online group or the in-person group (Table 1). A standardized training session was provided to both the online and in-office study patients and their families. The training focused on basics of image capturing using a camera, with an emphasis on proper focus and lighting to effectively capture high quality images. Participants and their families were also instructed on how to take standardized global and representative close-up lesional photographs. Additionally, subjects in the direct-access online group were taught how to access and utilize the online Web site to receive their dermatologic care. These participants had to demonstrate proficiency in navigating the telemedicine site before concluding their first visit.
Demographics of In-Person and Online Patient Groups
IGA, Investigator Global Assessment; IQR, interquartile range; POEM, Patient-Oriented Eczema Measure; SD, standard deviation.
Five dermatologists from the UC Davis Department of Dermatology were recruited to partake in this study. Four dermatologists provided care to study patients who were randomized to either online or in person. These dermatologists were trained on the use of the online telehealth platform, RelayHealth, which was a Web-based platform that facilitates asynchronous online encounters between patients and physicians. Patients completed the quality of life instruments throughout the study.
In-Person Group (Control Arm)
The subjects randomized to the office visits saw the dermatologist in person once every 2 months over a span of 12 months, for a total of six visits. During these visits, the participants received routine dermatologic care in which their AD was assessed and treatment plans were devised and discussed in person. Additionally, at each of these office visits, all adult subjects were asked to complete DLQI and SF-12. For pediatric subjects, the caregivers were asked to complete the CDLQI. Within 24 h of each office visit, the in-person participants uploaded photographs of their lesions for assessment by the blinded rater.
Direct-Access Online Group (Intervention Arm)
The subjects randomized to the direct-access online group engaged in six online dermatologist visits over 2-month intervals, for a total of six online visits. At each online visit, the participant accessed a secure online healthcare-delivery platform and asynchronously submitted necessary information. This information included photographs of their lesions as well as standardized questionnaires in which the participants recorded their progress and adverse incidents. Over the course of the study, in preparation for the visits, all participants were provided with clear hard copy and online instructions on how to photograph and upload images of the lesions, complete the questionnaires, and view the dermatologist's recommendations. At each of these online visits, DLQI, CDLQI, and SF-12 were completed.
Upon completion of the online visit, research staff reviewed the submitted information to ensure the image quality met necessary standards and the questionnaires were completed in entirety. The research staff then forwarded this information to the dermatologist. The dermatologist had three business days to evaluate the submitted information and make treatment recommendations online. The dermatologists also electronically prescribed medications. If the participants had inquiries regarding their care, they used the same online platform to asynchronously communicate with the dermatologist.
Quality of Life Instruments
DLQI and CDLQI are validated questionnaires that are widely used to assess dermatology-specific quality of life. The DLQI and CDLQI measures are comprised of 10 questions each. The scores for DLQI and CDLQI range from 0 to 30, where 0 indicates highest quality of life and 30 indicates lowest quality of life.
The SF-12 is an abbreviated 12-item version of the SF-36. SF-12 provides two measures of health status in adults—physical component score (PCS) and mental component score (MCS). The standard scoring algorithm for SF-12 was used to score adult subjects' responses to the 12 multiple-choice questions. Scores for the SF-12 PCS and MCS summary scales range from 0 to 100, where 0 indicates lowest quality of life and 100 indicates highest quality of life.
Statistical Analysis
This is an equivalency trial comparing the effectiveness of two models of delivering follow-up dermatological care for AD in terms of quality of life improvement.
The power calculations are as follows for the three quality of life measures. With a 1:1 allocation of subjects to the online-visit and office-visit groups and assuming the variance matrix with an autoregression structure, standard deviation for DLQI is σ1 = σ2 = σ = 5.6 and ρ1 = ρ2 = ρ = 0.62. With 70% adult patients, the study has 99% power to detect δ U = 3.25 as the equivalence limit for difference in the DLQI mean. With regards to CDLQI, the standard deviation is σ1 = σ 2 = σ = 5.6 and ρ1 = ρ2 = ρ = 0.55. With 30% (140 × 0.3 = 42) pediatric patients, the study has 80% power to detect δU = 3.25 as the equivalence limit for difference in the CDLQI mean between the comparison groups. With regards to SF-12, the standard deviation is σ1 = σ 2 = σ = 10 and ρ1 = ρ2 = ρ = 0.66. With 70% adult patients, the study has 99% power to detect δU = 6 as the equivalence limit for the difference in the SF-12 mean between the comparison groups.
To analyze the changes in DLQI, CDLQI, and SF-12 over the course of six visits, we performed longitudinal analysis using a repeated measures analysis of variance approach to identify potential differences in the trend over time between the two arms.
Results
A total of 156 patients were randomized to receive follow-up AD care via a direct-access online platform or in-person office visits over the course of 12 months. Among them, there were 110 adults and 46 children. Over the 12-month study period, patients in both the online group and in-person group showed significant improvement in quality of life as demonstrated by DLQI, CDLQI, and SF-12 scores.
Within-Group Comparisons
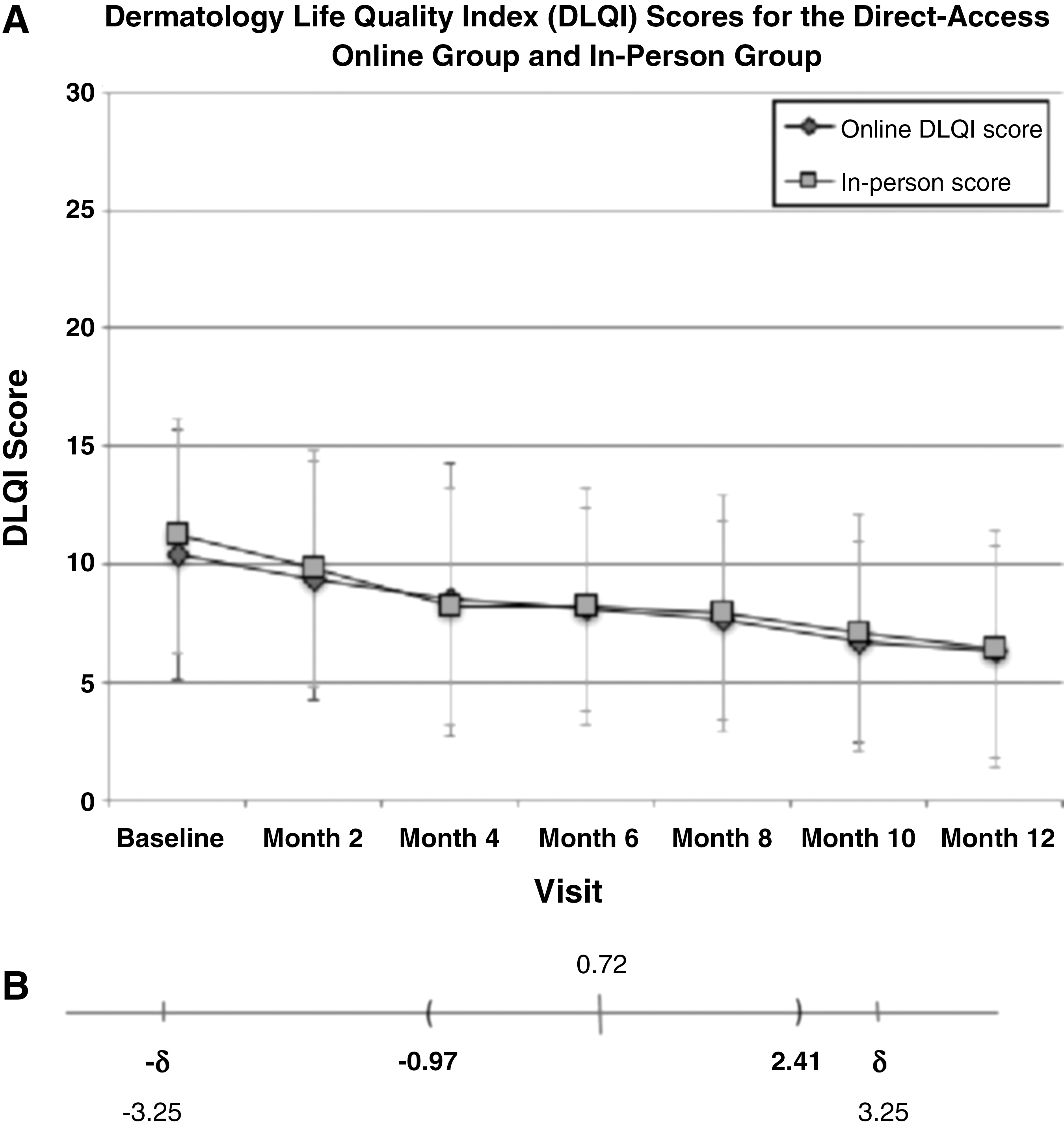
Specifically, in the direct-access online group, patients' DLQI scores improved from a mean (± standard deviation, SD) baseline of 10.4 (± 5.3) to 6.3 (± 4.5) at 12 months. This represented a within-group difference of 4.1 (± 2.3) for the direct-access online arm (Fig. 1A). In the in-person group, the patients' DLQI scores improved from a baseline of 11.2 (± 5.8) to 6.4 (± 4.4) at 12 months. This represented a within-group difference of 4.8 (± 2.7) for the in-person arm.
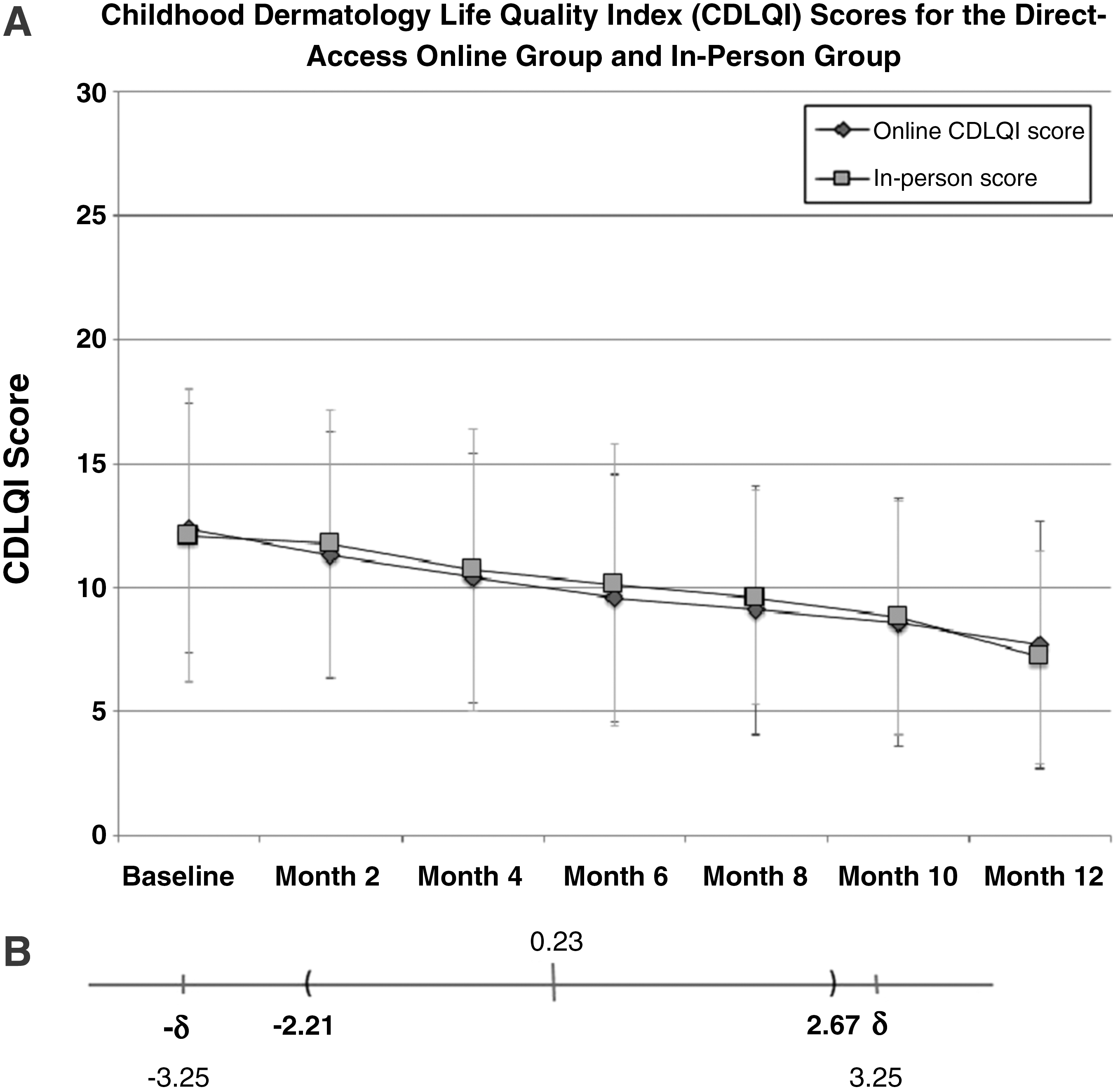
Among the pediatric patients, those randomized to the direct-access online group demonstrated improvement in CDLQI scores from a mean (± SD) baseline of 12.4 (± 6.1) to 7.7 (± 4.8) at 12 months. This represented a within-group difference of 4.7 (± 2.8) for the direct-access online arm (Fig. 2A). In the in-person group, the patients' CDLQI scores improved from a baseline of 12.1 (± 5.9) to 7.2 (± 4.3) at 12 months. This represented a within-group difference of 4.9 (± 3.1) for the in-person arm.
We assessed SF-12 scores among adult AD patients and report the results in terms of the PCS and MCS separately. In the direct-access online group, the PCS of SF-12 improved from a baseline of 43.6 (± 9.2) to 50.1 (±10.7) at 12 months. This represented a within-group difference of 6.5 (± 3.8) in PCS for the direct-access online arm. In the in-person group, the PCS improved from a baseline of 42.8 (± 9.7) to 49.6 (± 9.3) at 12 months. This represented a within-group difference of 6.8 (± 3.2) in PCS for the in-person arm.
In the direct-access online group, the MCS of SF-12 improved from a baseline of 39.2 (± 9.1) to 47.8 (± 9.3) at 12 months. This represented a within-group difference of 8.6 (± 4.3) in MCS for the direct-access online arm. In the in-person group, the MCS improved from a baseline of 38.3 (± 9.4) to 47.4 (± 9.7) at 12 months. This represented a within-group difference of 9.1 (± 3.8) in MCS for the in-person arm.
Between-Group Comparisons
We compared the differences in DLQI and SF-12 scores among adults with AD between the direct-access online group and the in-person group. The difference in the change in DLQI scores between the two groups was 0.72 (95% confidence interval [90% CI], −0.97 to 2.41); this difference is contained entirely within the equivalence margin of −3.25 to 3.25 (Fig. 1B).
The difference in the change of PCS of SF-12 scores between the two groups was 0.34 (90% CI, −1.16 to 1.84); this difference is contained within the equivalence margin of −6 to 6. The difference in the change of MCS of SF-12 scores between the two groups was 0.51 (90% CI, −1.11 to 2.13); this difference is also contained within the equivalence margin of −6 to 6. Therefore, in adults with AD, the direct-access online model is equivalent to the in-person model with regards to quality of life as measured by DLQI and SF-12.
In children, the difference in the change in the CDLQI scores between the two groups was 0.23 (90% CI, −2.21 to 2.67); this is contained entirely within the equivalence margin of −3.25 to 3.25. Therefore, in children with AD, the direct-access online model is equivalent to the in-person model with regards to quality of life as measured by CDLQI (Fig. 2B).
Discussion
In this study, we examined quality of life outcomes by comparing patients with AD who received follow-up care through a direct-access online model to patients receiving in-person care. While online care delivery models are being more frequently utilized, we currently lack evidence regarding its impact on quality of life among AD patients. 22 This study is the first to examine quality of life outcomes in an AD population who received follow-up care through a direct-access online model.
Because the AD lesions can cause shame, stigma, and discomfort, regular follow-up care with a dermatologist is critical. However, many patients do not have access to a dermatologist because of regional and financial constraints. Some studies have purported high-quality teledermatology as a potential solution for access to care issues. 17 The traditional asynchronous, “consultative” teledermatology requires patients to see a primary care provider who acts as a liaison between them and the dermatologist. Its adoption has at least been partially constrained due to PCPs' limited bandwidth. 14 –16,23
This study examined a direct-access model for follow-up care that provides patients with the opportunity to directly communicate with the dermatologist without requiring in-person visits or primary care liaisons. This study demonstrated equivalent quality of life outcomes between AD patients who received follow-up care through an asynchronous, online, direct-access model and patients who received care through in-person office visits.
The equivalent improvement in quality of life scores between the two groups may be attributable to characteristics unique to the direct-access model versus traditional telemedicine. The direct-access platform relieves patients from having to locate a primary care provider with telemedicine consultation resources, wait for an appointment with that PCP, take time off work or school to attend said appointment, commute to an office, and wait in the office to see the PCP. Instead, patients have the flexibility of capturing and uploading digital images and their medical histories directly to a dermatologist from the comfort of their homes at times that are most convenient for them. They can communicate directly with the dermatologist instead of relying on a liaison.
This study had various strengths. Because a substantial proportion of the participants hailed from underserved communities, we were able to assess the utility of a direct-access online model and demonstrate equivalent quality of life outcomes in those who tend to have more severe morbidity and less access to technology. 17 Also, this study design allowed for direct comparison of quality of life outcome equivalency between patients who receive online versus in-person follow-up care. Its controlled randomized design minimized selection bias, and there was regular follow-up with, and low attrition among, participants. This study also demonstrated the usefulness of SF-12 in assessing quality of life outcomes in AD patients and can set a precedent for utilizing SF-12 in future AD studies. The SF-12 instrument is advantageous to use, as it is not dermatology specific, thus enabling comparison of quality of life outcomes between dermatologic and nondermatologic conditions. 24
The findings of this study should be interpreted within the context of its limitations. The AD population in our study consisted of many younger individuals so our findings may not be generalizable to older patients. Also, our results may not translate to other skin diseases. Even though our study examined outcomes over a year, longer-term studies assessing the direct-access online model will be helpful to determine whether the improved quality of life outcomes persist.
In conclusion, this study demonstrated that there was no difference in quality of life between patients who were managed online via direct, asynchronous care versus those seen in person. While this study demonstrates the utility of a direct-access online model for AD, further research is needed to determine whether it may be used in other chronic skin disease states. To implement this model widely, it is important to safeguard the quality of the care through measures such as disclosing the licensure of providers, coordinating care with each patient's PCP, and seeking relevant follow-up clinical information. 25 Future studies can focus on how we can augment quality of care by incorporating these strategies into direct-access models.
Footnotes
Disclosure Statement
Dr. Armstrong has served as investigator and/or advisor/consultant for AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Merck, Modernizing Medicine, Novartis, Pfizer, Regeneron, and Sanofi.
No competing financial interests exist for the other authors.