
Abstract
Background:
Embedding Web-based interventions within physiotherapy has potential, but knowledge on patient adherence to these interventions is limited.
Introduction:
This study explores which patient-, intervention-, and environment-related factors are determinants of adherence to the online component of e-Exercise, a 12-week blended intervention for patients with hip and/or knee osteoarthritis.
Methods:
A convergent mixed methods study was performed, embedded within an ongoing trial. Quantitative data of 109 participants that received e-Exercise were used for negative binomial regression analysis. Adherence was defined as the number of online evaluated weeks. Next, semistructured interviews on factors related to adherence to the online component were analyzed.
Results:
Nineteen participants with missing outcome data because their program was not started were excluded. Of the 90 analyzed participants, 81.1% were evaluated for at least 8 weeks. Adherence was highest for participants with middle education, 1–5-year osteoarthritis duration, and participants who were physiotherapist recruited. The 10 analyzed interviews revealed that sufficient Internet skills, self-discipline, execution of the exercise plan, the intervention's usability, flexibility, persuasive design, added value, and acceptable required time, and research participation were linked to favorable adherence.
Discussion:
It is unknown if patients who adhered to the online component also adhered to their exercise plans. The relationship between adherence to the online component and clinical outcomes will be addressed in a future study.
Conclusions:
The majority of the participants adhered to the online component of e-Exercise, illustrating its applicability. The integration within the physiotherapy setting and intervention's persuasive design appear to have an important role in optimizing patient adherence.
Introduction
Osteoarthritis is an age-related joint disease that causes stiffness, reduced range of motion, and joint instability that are manifested in pain, disability, and loss of health-related quality of life. 1,2 The hip and knee are the most affected joints. 1 Face-to-face exercise therapy reduces pain levels and increases physical activity in patients with hip and/or knee osteoarthritis, 3,4 but is costly. Cost-effective strategies to manage hip and/or knee osteoarthritis are therefore needed. Web-based interventions (e.g., website with personalized goals, home exercises, and educational modules) have the potential to enhance patient self-management 5 and lower healthcare costs. 6,7 Although some Web-based interventions are offered without professional guidance, they can also be integrated with professional guidance, which is called blended care. 8 For patients with osteoarthritis, Web-based self-management interventions are linked to high acceptance and satisfaction levels, and have shown to modestly improve several health outcomes. 9
An example of such a Web-based intervention without professional guidance for patients with hip and/or knee osteoarthritis is the 9-week physical activity program Join2Move. 10,11 Join2Move was found to improve short-term (3 months) physical function and long-term (12 months) subjective and objective physical activity. 11 However, only 46.0% of the patients were considered adherent, 10 defined as the completion of at least 6 completed online week modules. 12 Since Web-based interventions are more effective for patients who adhere, 13,14 Join2Move's effectiveness potentially can be increased if adherence can be improved. Based on semi-structured interviews, lack of human involvement and professional guidance was named as reasons for nonusage among participants of the Join2Move study. 10
This led to the development of e-Exercise, a 12-week physical activity program for patients with hip and/or knee osteoarthritis that combines an online component based on Join2Move with offline, face-to-face physiotherapy sessions. 12 Furthermore, the intervention's persuasive design was improved by adding several new features. 12 Both therapeutic contact 15,16 and persuasive design 16 are intervention-related factors associated with favorable adherence. The (cost)effectiveness of e-Exercise is currently being studied. 17
Since blended care is a new, upcoming treatment option, knowledge on adherence to the online component of these interventions and how that might differ from fully Web-based interventions is limited. Insight in patients' adherence to the online component of e-Exercise will contribute to this body of knowledge, as well as its implementation. Identifying which subpopulations adhere to the program and which factors are related to these possible differences in adherence will help determine which subpopulations can be targeted and how the program can be improved. Therefore, this study explores what patient-, intervention-, and environment-related factors are determinants of adherence to the online component of e-Exercise.
Methods
Study Design
A convergent mixed methods study was executed, embedded within a trial on the (cost)effectiveness of e-Exercise. 17 Qualitative and quantitative data were analyzed during the same time span. Quantitative analysis mostly targeted patient-related factors, while qualitative analysis was expected to particularly yield intervention- and environment-related determinants. The e-Exercise trial was approved by the Medical Ethics Committee of the St. Elisabeth hospital Tilburg (NL 46358.008.13). 17
Participants
Participants of the e-Exercise trial were recruited in Dutch primary care physiotherapy practices or through advertisements from September 2014 to March 2015. Patients were eligible when they (1) were aged 40–80 years and (2) had osteoarthritis of the hip and/or knee according to the American College of Rheumatology criteria. 17 Patients were excluded when they (1) were on a waiting list for a hip or knee replacement surgery, (2) were being contraindicated for physical activity without supervision, (3) were sufficiently physically active based on Dutch physical activity guidelines, 18 (4) had received physical therapy for their osteoarthritis in the last 6 months, (5) did not have Internet access, or (6) were unable to understand the Dutch language. 17 Quantitative data of all 109 participants who were randomized to the intervention group of the e-Exercise trial were used for this study. To limit recall bias during semistructured interviews that were executed in October and November 2015, the 20 last included patients were invited. If necessary, additional participants were recruited for telephonic interviews based on purposeful and theoretical sampling until optimal variability in patient characteristics (age, geographic location, comorbidity, and adherence) and data saturation in two consecutive interviews were achieved.
Intervention
The online component of e-Exercise consists of (1) a 12-week incremental physical activity program based on graded activity, (2) strength and stability exercises, and (3) information on osteoarthritis-related themes. 17 The offline component consists of up to five face-to-face physiotherapy sessions 17 that comply with the Dutch guideline for hip and knee osteoarthritis. 19
In the first session, the physiotherapist created an account, instructed the patient on using the e-Exercise Website, and selected exercises. During the first week, patients submitted their baseline capacity for their central activity through an online form. This baseline capacity was determined by performing the targeted activity on three independent days for as long as acceptable. In the second session, the physiotherapist and patient used this baseline value to set a goal for the short and long term. The physiotherapist would then press the “start the program” button, after which the system automatically created an individual activity scheme that gradually increased to the patient's short-term goal. Pressing the start button was essential, since the patient otherwise would not receive access to the full intervention, including the weekly graded activity and exercise modules, and evaluation forms.
After the program was started, patients received automated weekly e-mails that informed them about new Website content and reminded them to evaluate their weekly graded activity and exercise modules. Evaluation of the graded activity modules consisted of the question if the participant performed more, less, or exactly the assigned minutes of physical activity and an eleven-point Numeric Rating Scale (NRS) for pain during that activity. Evaluation of exercises consisted of an eleven-point NRS for difficulty of the exercise. During face-to-face sessions, the physiotherapist used these evaluations to discuss the patient's progress and if necessary change the intensity or exercise type. A more detailed description of the intervention can be found in the study protocol. 17
Quantitative Data Collection
Outcome variables
Adherence to the online component of e-Exercise was operationalized as the number of weeks that a participant evaluated either a graded activity or exercise module. The main outcome variable was therefore a discrete (count) variable with a minimum of 1 and a maximum of 12 weeks with an evaluated module. In addition, to allow comparison to the Join2Move study, participants were labeled adherent to the online component when they evaluated at least 8 out of the maximum of 12 modules, using the same ratio as the Join2Move study. 10
Independent variables
The measuring instruments, categories, and value ranges of included variables are described in Table 1. The number of treatment sessions was determined after the intervention period. All other variables were measured at baseline. More detailed information can be found in the study protocol. 17
Description of the Used Measurement Instrument, Categories, Value Ranges, and Association with Adherence for Independent Variables Used in Quantitative Analysis
Participants wore the ActiGraph at least 8 h per day for at least 3 days. The physical activity thresholds of Freedson et al. 43 were used as cutoff points for physical activity intensity.
Quantitative Data Analysis
Descriptive statistics for the observed independent and outcome variables were calculated. Depending on their distribution, a percentage (if categorical), mean, and standard deviation (if normal) or a minimum, maximum, and median (if nonnormal) were described. Negative binomial regression analysis, a method that is appropriate to count data that follow the negative binomial distribution, was performed using the inversed outcome data. 20 First, univariate analyses were performed to screen for potential determinants using a p-value of ≤0.2. Second, a multivariate analysis was performed with a backward stepwise procedure, 21 excluding variables with p-value of p ≥ 0.1. To determine the maximum number of independent variables in the final model, a rule-of-thumb that the ratio of participants to independent valuables needed to be 10:1 was applied. 22,23 The final model's Goodness of Fit was evaluated using the omnibus test 24,25 and the ratio of the deviance and Pearson Chi-Square values to the degrees of freedom, which ideally should be close to 1.
Qualitative Data Collection and Analysis
Initial semistructured interviews were performed by two research assistants using a topic list (Online Appendix 1) that was based on a study by Fleuren et al. 26 Interview audiotapes were transcribed verbatim by HdV. HdV and CK performed open coding independently. 27,28 Investigator triangulation was applied by performing axial and selective coding in cooperation by constant comparison of codes within and between interviews. 27,28 Codes expressing related concepts were grouped to create themes. Respondent validation was performed through member checks by e-mailing participants a summary of the interview. An audit trail, including theoretical memos, was tracked and inspected by DB. 29
Results
For 5 out of the 109 participants who were randomized to the intervention group of e-Exercise, no account was identified. In addition, for 14 participants with an account, the “start the program” button was never pressed by the physiotherapist for unknown reasons. Since no adherence outcome data were available for these 19 participants, they were excluded for quantitative analysis and the remaining 90 (82.6%) were analyzed. No significant difference was found for the baseline characteristics of the 90 participants who were analyzed and the 19 participants who were not. A flowchart of the included participants is depicted in Figure 1.
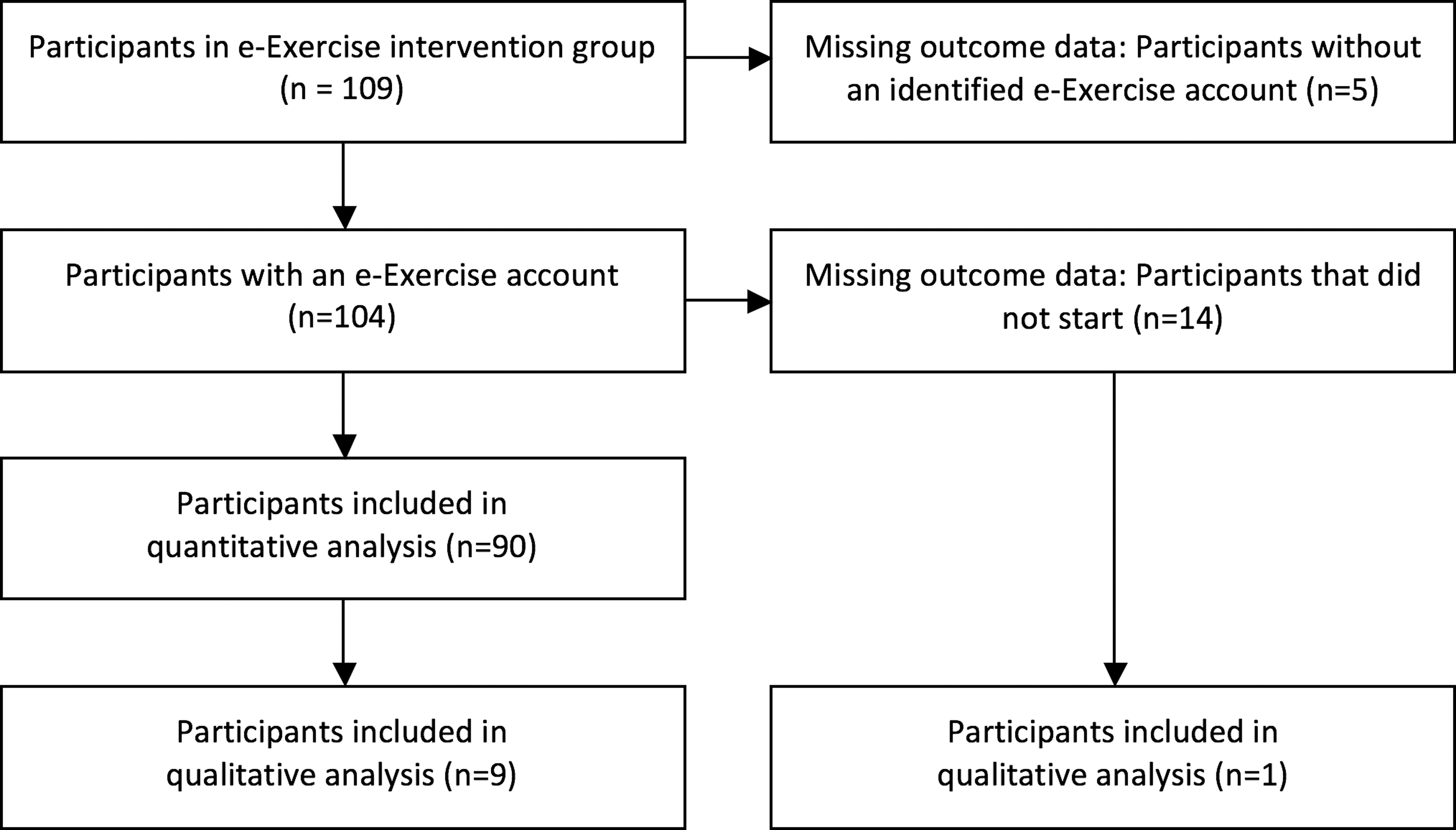
Flowchart of included participants.
Quantitative Results
For the 90 participants analyzed, values for physical mobility (25.6%) and both sedentary time and MVPA (12.2%) were missing. In total, 81.1% of the analyzed participants evaluated a module during at least 8 weeks and were therefore considered adherent to the online component (Table 2 and Figure 2). Based on univariate negative binomial regression analyses, education (p = 0.092), osteoarthritis symptom duration (p = 0.109), recruitment strategy (p = 0.096), and self-efficacy for symptoms (p = 0.138) were included for multivariate analysis. The final model (Table 3) was significant (Omnibus Test p = 0.015) and fits the negative binomial distribution well (deviance Value/df 1.010 and Pearson Chi-Square Value/df 0.839). Middle educated participants were 39.7% more likely to adhere to the online component than low-educated participants and 31.6% more likely than highly educated participants. Also, participants who were recruited by a physiotherapist were 62.7% more likely to adhere than participants recruited by advertisement. Participants who experienced osteoarthritis symptoms for less than 1 year were 87.3% less likely to adhere than participants with a symptom duration of 1–5 years and 34.0% less likely to adhere than participants who had symptoms for more than 5 years.
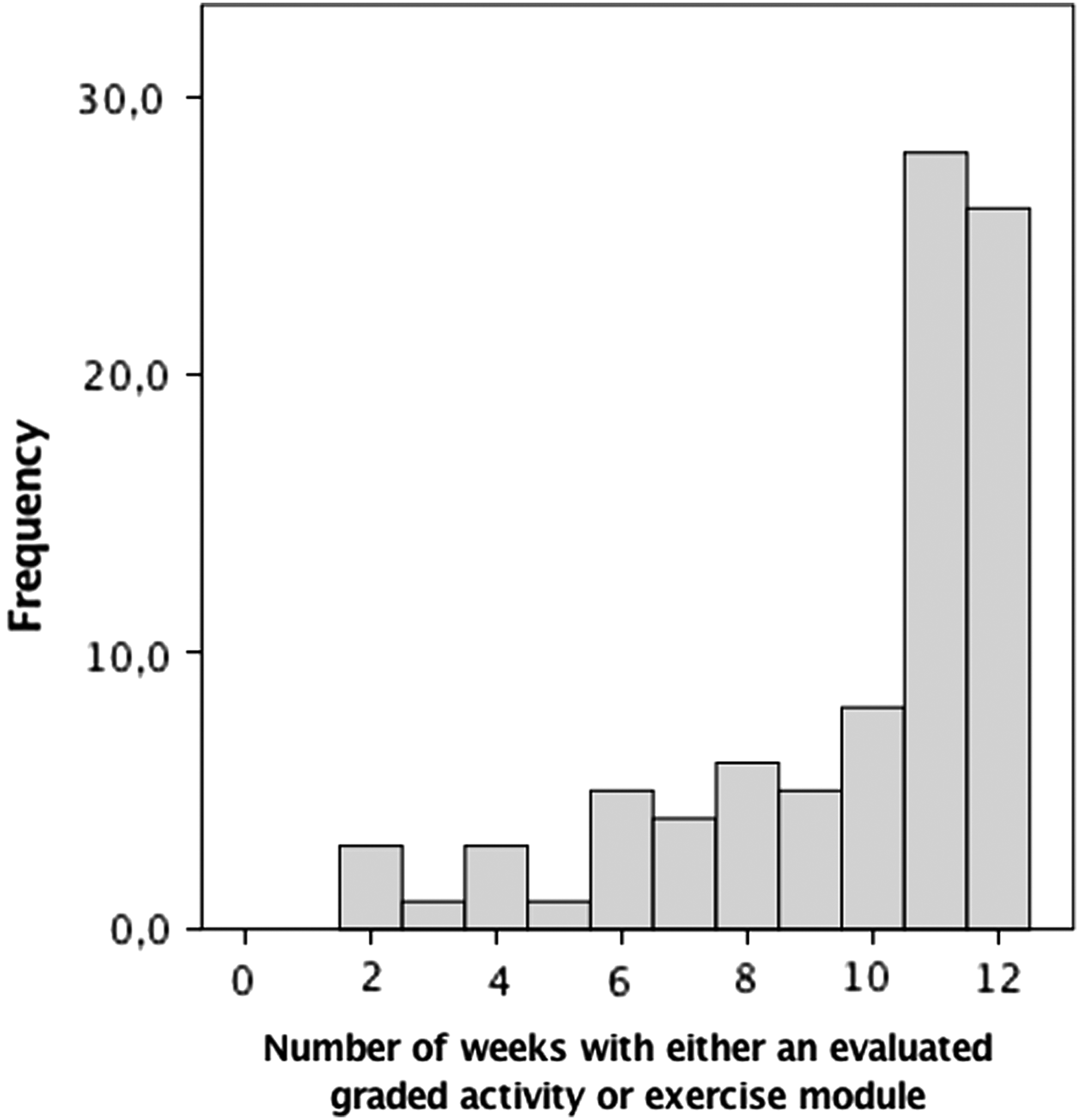
Histogram for the number of weeks that the participant evaluated either a graded activity or exercise module, illustrating substantial negative skewness that favors adherence.
Descriptive Statistics for Independent and Outcome Variables for Participants That Were Included in Quantitative Analysis
Independent variable that was a significant predictor of adherence during univariate binomial regression analysis (p ≤ 0.2).
p-Values and β-Coefficients of Patient- and Environment-Related Determinants of Adherence to the Online Component
Because inversed outcome data were used, negative β-coefficients indicate higher adherence, while positive β-coefficients indicate lower adherence
Qualitative Results
Of the 20 invited participants, 8 responded and were interviewed. Data saturation appeared after six interviews. All participants confirmed the validity of the member checks. To obtain optimal variation in patient characteristics, two more interviews were performed, but no new theme was found. The 10 interviewed participants were mostly female (70%), without comorbidity (60%), aged 51–79 (median: 60) years, received 0–6 (median: 5) treatment sessions, and evaluated a module in 1–12 (median: 10.5) weeks. These characteristics were similar to those of the total sample (Table 2) and were therefore considered representative.
Patient-related determinants
Three patient-related determinants were identified: (1) Internet skills, (2) self-discipline, and (3) execution of the exercise plan. Sufficient Internet skills and self-discipline were described as prerequisite to use the online component. A participant with optimal adherence to the online component explained how she was motivated to keep exercising because of the experienced treatment effect: “Life just becomes better by participating in the program.”
Intervention-related determinants
Six intervention-related determinants were identified: (1) Website usability, (2) persuasive design, (3) flexibility of the exercise schedule, (4) added value, (5) time required, and (6) the physiotherapist. Examples of positively evaluated persuasive features were received through weekly e-mail reminders and monitoring of behavior. One participant described that she wanted the assignments to be more flexible in adjusting exercises and goals. Also, participants described that the online component needed to have an added value over regular therapy options and requires little time to use. A well-travelled participant explained, “We went on vacation for 3 weeks and because of the online program I exercised every morning and evening.”
The physiotherapist's role was mostly described as facilitating, but sometimes as restricting. One interviewed participant reported that her physiotherapist never started the program: “I think it's a shame that the physiotherapist did not know how the program worked.” For others, the physiotherapist had a positive influence by tailoring the exercise program to their needs, offering complementary therapy, monitoring progress, and enhancing self-efficacy. Also, participants felt obliged to adhere because of the anticipated rewards for (non-)adherence by their physiotherapist. One participant explained, “This whole program just uses a carrot-and-stick approach. I think a lot of people — not just me — need that.”
Environment-related determinants
Several participants were extra motivated to adhere because they participated in a study. All themes describing determinants of adherence are summarized in Table 4.
Themes Describing Determinants of Adherence to e-Exercise
Discussion
This study found that 81.1% of the analyzed participants adhered to the online component of e-Exercise. While fully Web-based interventions oftentimes struggle with low adherence, 16,30 this study confirms that e-Exercise is applicable for patients with hip and/or knee osteoarthritis. 12 In a future study, we will investigate the relationship between adherence to the online component and effectiveness in terms of clinical outcomes. 17 Several nuances can be made regarding patient-, intervention-, and environment-related factors to adherence to the online component.
These results are in concordance with the Technology Acceptance Model. 31 They illustrate that perceived ease-of-use and perceived usefulness can determine the attitude and behavioral intention toward use, influencing adherence. Nonetheless, these results also offer insight in the specific factors influencing adherence to e-Exercise. For instance, adherence to the online component of e-Exercise was highest for middle educated participants, while adherence to Web-based interventions is typically highest for highly educated participants. 32 Possible explanations might be that participants with different educational levels might have different needs regarding the form and extent of given information and/or that the addition of videos to communicate information and exercises worked well for this subpopulation.
Furthermore, participants who had osteoarthritis for less than 1 year were less likely to adhere to the online component. It is possible that participants with a shorter osteoarthritis duration perceived less necessity and were therefore less motivated to adhere. This might also explain the finding that participants who were recruited by advertisement were less adherent than patients recruited at a physiotherapy practice, since the latter group actively sought therapy for their experienced problems. Another influential aspect is the intervention's persuasive design. 16 For e-Exercise, 2 behavior change techniques of the CALO-RE taxonomy were found influential: monitoring of outcomes of behavior and prompts/cues. 33 Finally, some participants described to adhere because they participated in a study, which is a well-known environment-related factor, 34 particularly in trials. 16
Little research is available about the adherence of patients with osteoarthritis to online interventions. The online component of e-Exercise was based on Join2Move. This study reported, based on intention-to-treat, that 46% adhered to the online intervention. According to the intention-to-treat principles, the adherence of e-Exercise was 67.0% (73 out of 109 participants). 10 This difference in adherence can be declared by improvements in the design and the addition of 3 extra week modules. However, the most important difference between Join2Move and the online component of e-Exercise is the integration within the physiotherapy setting. Physiotherapists enticed participants to adhere because of perceived rewards or judgment. The physiotherapist could also adjust the treatment plan and stimulate the participant to keep executing it. The differences between both interventions and design characteristics of e-Exercise are described in more detail elsewhere. 12,17
Several limitations of this study need to be addressed. First, it is unknown whether participants who adhered to the online component of e-Exercise also adhered to the intended exercise behavior. It is possible that participants evaluated activities and exercises that they did not perform, but also that they exercised while not evaluating the module online. Second, the interview with one participant illustrated that her physiotherapist did not start her program, what she attributed to him being uninformed. It is unknown to what extent the physiotherapists of the other eighteen participants without an account or program start were accountable or whether these participants dropped out themselves. Finally, a sequential explanatory mixed methods design would have been more appropriate for this study, since the quantitative findings could then potentially be explained during qualitative analysis. However, was not possible due to practical and time-bound reasons.
Both these findings and prior literature 8 underline the importance of the therapeutic role in blended care and that optimal integration is essential for patient adherence. Therefore, implementation of e-Exercise should focus on implementing the online component in the physiotherapists' routines. Although all physiotherapists underwent a half-day of training, 17 some physiotherapists still appeared unaware about how to correctly use the intervention. To facilitate patient adherence, the online component should have added value, be flexible, and easy to use. More persuasive design features can also be expected to influence adherence. Physiotherapists can consider offering patients with insufficient Internet skills or increased physical disabilities more extensive face-to-face treatment next to the online component.
Conclusions
The majority of participants adhered to the online component of e-Exercise, confirming that e-Exercise is applicable for patients with hip and/or knee osteoarthritis. The physiotherapist has an influence on patient adherence due to his role in recruitment, program personalization, and motivating the patient. The online components' usability, flexibility, time required, persuasive design, and added value were linked to adherence.
Footnotes
Acknowledgments
The authors thank all participants for their cooperation, Michelle Eem and Dianne van der Eijk for their efforts in collecting qualitative data, and Peter Spreeuwenberg for his help during statistical analysis.
The project was funded by ZonMW, Dutch Artritis Association, and the Royal Dutch Association for Physiotherapy.
Disclosure Statement
No competing financial interests exist.