
Abstract
Introduction:
Timely access to orthopedic rehabilitation is an important problem for the Ukrainian healthcare system. The international orthopedic community aims to achieve the best possible outcome for patient care by modifying rehabilitation methods and using telemedicine technology. The theme of this article is to discuss the integration of telemedicine technology in the rehabilitation of patients with injuries of the lower extremities.
Materials and Methods:
Consecutive patients were recruited over a 2-year period. A total of 74 subjects with lower extremity injuries were enrolled in the study and monitored during a 3-month period. Twenty-six patients from the control group underwent traditional rehabilitation procedures for a 3-month period after injury. A total of 48 subjects were enrolled in the telerehabilitation group for a 3-month study period and were trained with a set of exercises for home use. Home remote monitoring for the 48 test subjects included use of a smartphone with gyroscope, G-sensor, magnetometer, and barometer, which was fixed to the injured limb. Software for the smartphone was developed at the I. Horbachevsky Ternopil Medical University, Ukraine. Software permits the monitoring of exercise time, the frequency of active movements of the injured limb, the number of steps per hour, and the walking speed.
Results:
The 3-month rehabilitation period started with the power load of 10% of body weight, following 3–5 steps five times per day with a speed no >1 km/h. The orthopedic surgeon, during telerehabilitation, took significantly less time to consult patients (2.3 min ± 0.4) than the traditional rehabilitation (12.6 min ± 2.9). Patient satisfaction was higher for the telerehabilitation (83.1% ± 14.2) than for the orthopedic surgeon's traditional rehabilitation (33.1% ± 8.9).
Conclusions:
Telerehabilitation is a good alternative for providing access to specialty care for the growing number of patients with traumatic injuries.
Introduction
Timely access to orthopedic rehabilitation is an important problem for the Ukrainian healthcare system. 1 Presently, in a post-USSR country wait times to see an orthopedic surgeon can exceed 2 months and with a rapidly aging population, as well as the increased incidence of obesity, the need for orthopedic care is expected to drastically increase in the coming years. 2 Efforts have been made to ensure timely access to orthopedic care for the population yet, despite an investment in resources, wait times for a consult remain excessively long. 3 –5 The international orthopedic community aims to achieve the best possible outcome for patient care by modifying rehabilitation methods and using telemedicine technology. Furthermore, these techniques demand that surgeons acquire information at a rapid rate while enforcing higher standards in rehabilitation. To meet this need, new telemedicine technology is needed that will significantly influence the rehabilitation of the patients with injuries of the lower extremities. 6 Global insight into the diversity of telemedicine standards should be resolved with a comprehensive plan that considers regulations that are enforced by different countries.
Therefore, the theme of this article is to evaluate of implementation of the telemedicine technology for rehabilitation of the patients with injuries of the lower extremities. The main prerequisite for success within the orthopedic community is to identify indications and contraindications for distance rehabilitation. 7
All of these tasks can be accomplished if we continue to advance technology development. 8 Also needed is access to emerging innovations and projects from other countries to improve musculoskeletal care in Ukraine.
At I. Horbachevskyy Ternopil Medical University in the Ukraine, new models of telerehabilitation are being implemented. These new models are aimed at improving the efficiency of rehabilitation for patients with injuries of the lower extremities. 9,10 One area of innovation is the development of a computerized system (“server and the doctor” — “patient and sensor”), which allows remote monitoring and correction of dosed axial loads on injured limbs in real time to improve outcomes and patient satisfaction. 11 –14
Materials and Methods
Consecutive patients were recruited over a 2-year period—September 2014 to July 2016—from the waiting lists of the department of orthopedic surgery, at Ternopil Emergency Hospital that serves as a trauma center. A total of 74 subjects with lower extremity injuries were enrolled in the study and monitored during a 3-month period.
All enrolled subjects signed a consent form before participating in the study. The Research Ethics Board of the I. Horbachevskyy Ternopil Medical University, Ukraine approved the research study.
Twenty-six patients from the control group underwent traditional rehabilitation procedures for a 3-month period after injury. This usual care group included the generally accepted methods of rehabilitation therapy (i.e., massage, myostimulation, walking without a load on the injured limb, and exercises in the pool).
A total of 48 subjects were enrolled in the telerehabilitation group for a 3-month study period after injury and were trained with a set of exercises for home use.
Home remote monitoring for the 48 test subjects included use of a smartphone, equipped with gyroscope, G-sensor, magnetometer, and barometer, which was fixed to the injured limb. Software for the smartphone was developed at the I. Horbachevskyy Ternopil Medical University, Ukraine. During the execution of home exercises, data from the sensors on the subject's smartphone were measured and transmitted to a server through a cellular Internet connection with a bandwidth of 2 megabits per second (Mbps) and to the personal smartphone of the treating doctor and displayed as digital data and graphically.
The telerehabilitation protocol included the following: • Fixation of the smartphone to the injured limb and use of customized software • Home exercises: Passive flexion-extension, abduction in the leg, a circular motion in adjacent joints • Home exercises: Active flexion-extension, abduction in the leg, a circular motion in joints • Dosed load on injured limb using crutches • Dosed load on injured limb without using crutches
Patients were also trained for subjective assessment of pain on a 10-point scale and measuring the volume of lower extremity soft tissue using the measuring tape at a point 10 cm proximal to the knee joint before and after each stage of the exercise. The initial implementation of this telerehabilitation model did not include prescription of medications or joint injections.
The smartphone contained a tailored personal rehabilitation record for health information and communication between the patient and health professionals. Outcome measures included movement activity and number of steps recorded daily on a step counter using the smartphone's sensors. Data were transmitted wirelessly from the smartphone to the doctor's server. Based on the patient's individual condition, the rehabilitation doctor created an individualized rehabilitation plan for each subject, containing an activity plan with goals for daily steps. This was done in accordance with the Ukrainian Association of Orthopedic Rehabilitation recommendations and in collaboration with the subject before discharge from the hospital. Both the subjects and the health professionals at the hospital had access to and communicated through the Internet using customized software. All patients had personal goals for daily movement activity and steps in the rehabilitation program. In addition to access to health information, the movement activity sensor and step counter was the only telerehabilitation technology that the patients retained during a 3-month period.
The telerehabilitation technology provided the patients with insights into their own movement and walking activity, enabling them to monitor their own activity plans (Fig. 1). All subjects from telerehabilitation group were assigned a personal doctor. The control group received traditional rehabilitation at home without a personal doctor.

Smartphone attached to the lower limb.
Subjects completed a questionnaire where they provided anthropometric data, as well as information on their education, employment, household income, household living status, and information on clinical variables such as the joints affected, the reason for consulting, the duration of their symptoms, the use of a walking aid, and the presence of any comorbidities. All subjects from both groups also completed the Lower Extremity Functional Scale (LEFS) questionnaire, which is used to evaluate the functional disabilities of a patient with a lower extremity disorder. The LEFS score ranges from 0 to 80 with a higher score indicating a higher functional status. The use of the LEFS in research studies has been validated, and the LEFS is a reliable tool for assessing lower extremity functional status. The majority of patients (75%) cited pain as the reason for consult with the orthopedic surgeon and all of the patients (100%) consulted for a knee disorder (after injuries of the lower extremities). All patients had imaging tests available in their file at the time of consult (X-ray and CT scan).
Results
In the telerehabilitation arm of the study, 74 subjects with injuries of the lower extremities were symptomatic for at least 2 weeks.
Subjects from telerehabilitation group had a mean age of 43.1 years, and the majority of these subjects were men (64.6%). The mean LEFS score of patients was 44.62. Table 1 presents selected characteristics of the participants of the telerehabilitation group.
Characteristics of the Study Participants of the Telerehabilitation Group (n = 48)
In the control group of the study, 26 subjects with injuries of the lower extremities were symptomatic for at least 2 weeks and continued rehabilitation at home without an assigned doctor. Subjects had a mean age of 51.6 years, and the majority of these subjects were men (65.4%). The mean LEFS score of patients was 36.43. Table 2 presents selected characteristics of the participants.
Characteristics of the Study Participants of the Control Group (n = 26)
During the telemonitoring, the physician controls the adequacy of execution of each stage of rehabilitation exercises and has the ability to adjust the load in real time depending on the functional state of the limb (Fig. 2).
Monitoring of the exercises time and the frequency of active movements of injured limb.
Software allows monitoring of the exercises time, the frequency of active movements of injured limb, number of steps per hour, and walking speed.
The 3-month rehabilitation period started with the power load of 10% of body weight, following 3–5 steps five times per day with a speed no >1 km/h.
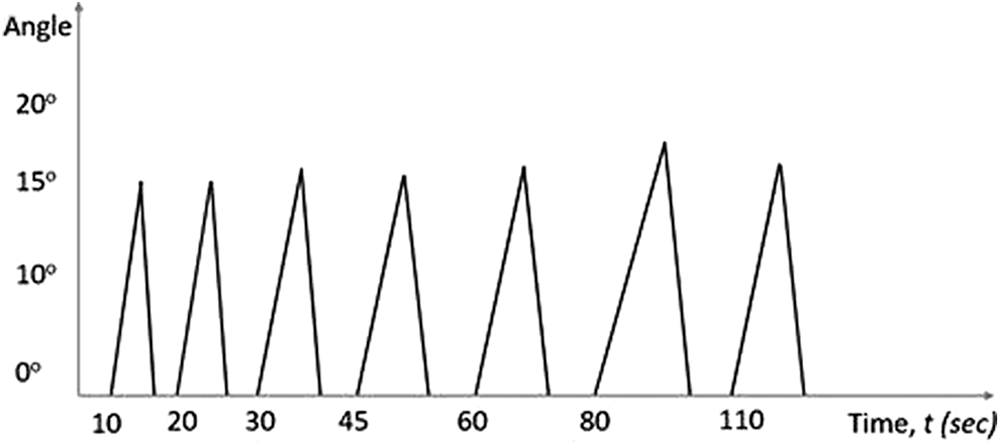
Subjects were also asked if their pain level increased after the first exercise and in the event that it did, they were asked to indicate by how much it increased by picking one of the following three options on the smartphone: 1–4 pain was a bit stronger; 5–7 pain was moderately stronger; and 8–10 pain was much stronger. The algorithm allows increasing the daily load on 1%, if the assessment of pain after exercise was not >7 points on 10-point scale and progressive limb edema was absent (Fig. 3). If pain persisted or questions persisted, subjects were invited for a visit to the doctor with correction of the rehabilitation algorithm.
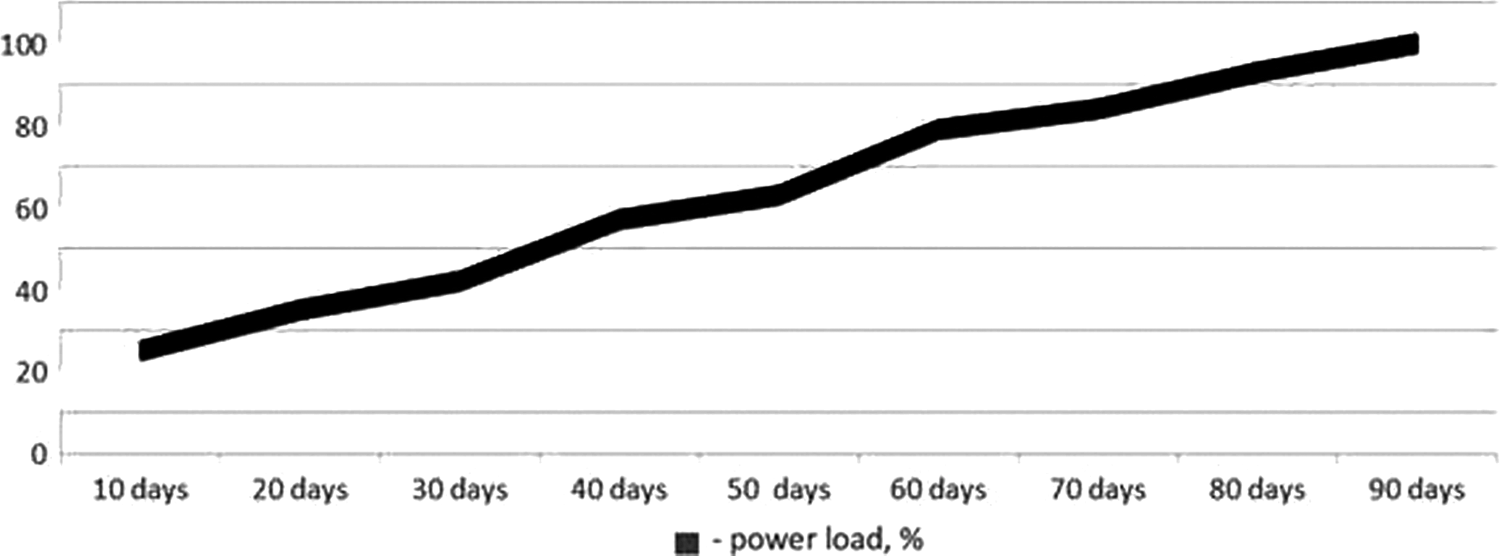
Change of power load for 90 days, %.
The orthopedic surgeon during telerehabilitation took significantly less time to consult patients (2.3 min, SD: 0.4) than the traditional rehabilitation (12.6 min, SD: 2.9). Patient satisfaction was higher for the telerehabilitation (83.1%, SD: 14.2) than for the orthopedic surgeon's traditional rehabilitation (33.1%, SD: 8.9) (Table 3).
Comparison Between Visit Time Length and Patient Satisfaction for Telerehabilitation (n = 48) and Traditional Orthopedic Rehabilitation (n = 26)
Discussion
Subjects reported a higher satisfaction with telerehabilitation than with the traditional orthopedic rehabilitation due to the fact that they spent less time at the hospital and had more time for exercises at home under orthopedic remote monitoring. It is assumed that less clinical time per subject using telerehabilitation translates into reduced costs of rehabilitation during the study period.
Telerehabilitation is a good alternative for providing access to specialty care for the growing number of patients with traumatic injuries. Modern smartphones, computer networks, and software systems allow for a low cost system compared with traditional rehabilitation, and the potential for treatment of patients in the home environment is improved with telerehabilitation.
The telerehabilitation system and dosed load algorithm can be used in complex rehabilitation of patients with injuries of the lower extremities. This will improve the quality of life in this group of patients and significantly reduce the cost of the rehabilitation period. These results provide preliminary evidence supporting the telerehabilitation model for orthopedic care. We conclude that telerehabilitation should be considered a key component in the long-term management of patients who have lower extremity injuries.
Footnotes
Disclosure Statement
No competing financial interests exist.